Risk factors for COPD exacerbations and mortality, and variation between primary care settings: the PRAXIS cohort study in Sweden
Carolina Smith, Ayako Hiyoshi, Tor Arnison, Gabriella Eliason, Maaike Giezeman, Mikael Hasselgren, Christer Janson, Mikael Karlsson, Marta A Kisiel, Karin Lisspers, Anna Nager, Hanna Sandelowsky, Björn Ställberg, Josefin Sundh, Scott Montgomery

TL;DR
The study found that COPD exacerbations and mortality are more influenced by individual patient factors than differences between primary care centers in Sweden.
Contribution
The study identifies anxiety and cardiovascular disease as significant risk factors for COPD mortality and highlights the importance of individualized care.
Findings
Variability between primary care centers had minimal impact on COPD outcomes.
Anxiety and cardiovascular disease were strongly associated with increased mortality risk.
Body mass index showed a U-shaped relationship with mortality.
Abstract
We aimed to examine the variability of chronic obstructive pulmonary disease (COPD) exacerbations and mortality, between primary healthcare centres, and their associations with comorbid diseases and body mass index, during an 8-year follow-up. This was a cohort study using multilevel modelling with follow-up from 2014 to 2022. Data came from questionnaires in 2014 and 2022 and medical record reviews between 2004 and 2014. The main outcomes were exacerbations in 2022 and mortality by 2022. Exacerbations were defined as any emergency visit, and/or use of oral steroids or antibiotics due to worsening of COPD symptoms during the previous 6 months. The PRAXIS study included patients at 76 primary healthcare centres in central Sweden. Primary care patients aged ≤75 years and with a diagnosis of COPD in their medical records between 2007 and 2010 were included in 2014 (n=1163) and followed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
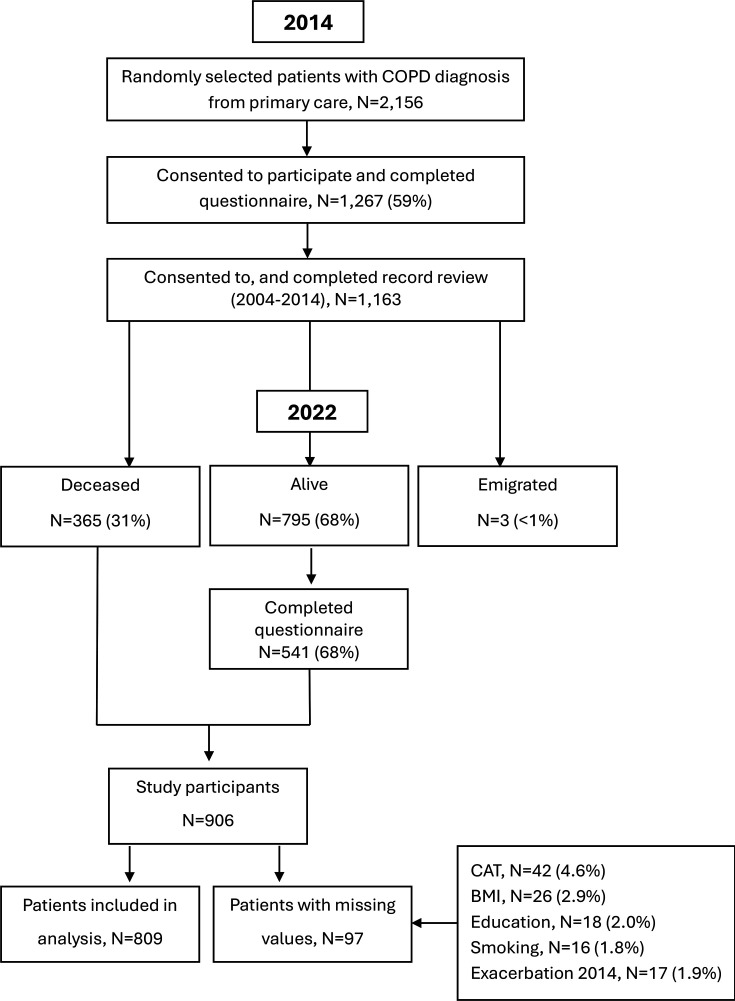 Figure 1
Figure 1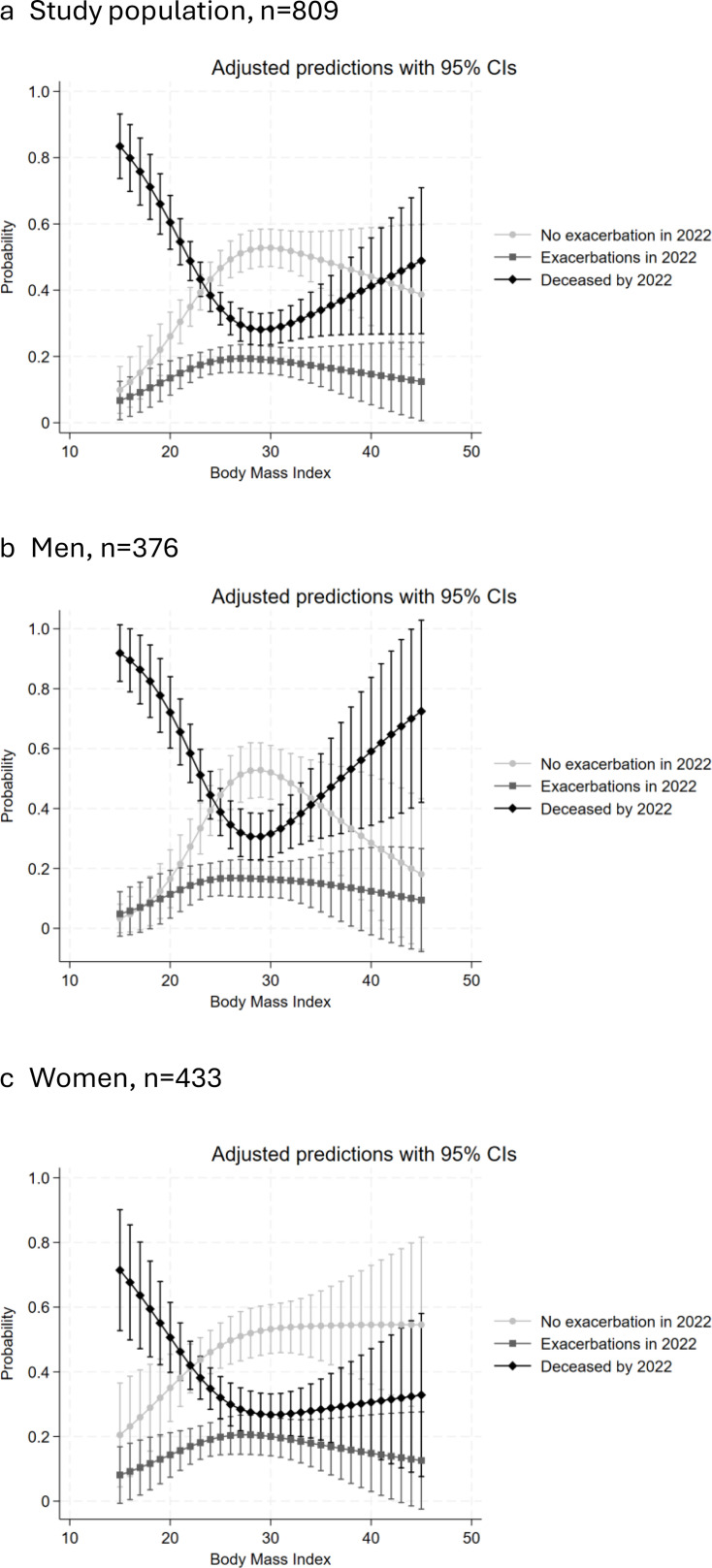 Figure 2
Figure 2| No exacerbation in 2022 | Exacerbations in 2022 | Deceased by 2022 | |
|---|---|---|---|
| N (%) | 355 (43.9) | 140 (17.3) | 314 (38.8) |
| Sex, n (%) | |||
| Female | 197 (55.5) | 82 (58.6) | 154 (49.0) |
| Male | 158 (44.5) | 58 (41.4) | 160 (51.0) |
| Age, n (%) | |||
| <60 years | 51 (14.4) | 28 (20.0) | 19 (6.1) |
| 60–64 years | 63 (17.8) | 17 (12.1) | 30 (9.6) |
| 65–69 years | 108 (30.4) | 37 (26.4) | 89 (28.3) |
| 70–74 years | 105 (29.6) | 44 (31.4) | 120 (38.2) |
| ≥75 years | 28 (7.9) | 14 (10.0) | 56 (17.8) |
| Age (years), median (IQR) | 68 (63–71) | 69 (62–72) | 70 (67–73) |
| BMI, n (%) | |||
| <18.5 kg/m2 | 5 (1.4) | 3 (2.1) | 23 (7.3) |
| 18.5–24.9 kg/m2 | 112 (31.6) | 55 (39.3) | 136 (43.3) |
| 25–29.9 kg/m2 | 154 (43.4) | 48 (34.3) | 89 (28.3) |
| ≥30 kg/m2 | 84 (23.7) | 34 (24.3) | 66 (21.0) |
| CAT score, mean (SD) | 12.6 (7.5) | 17.2 (7.8) | 16.9 (8.5) |
| Smoking, n (%) | |||
| Never smoker | 15 (4.2) | 7 (5.0) | 11 (3.5) |
| Former smoker | 229 (64.5) | 87 (62.1) | 197 (62.7) |
| Current smoker | 111 (31.3) | 46 (32.9) | 106 (33.8) |
| Education, n (%) | |||
| Low | 209 (58.9) | 76 (54.3) | 196 (62.4) |
| High | 146 (41.1) | 64 (45.7) | 118 (37.6) |
| Exacerbation in 2014, n (%) | 70 (19.7) | 66 (47.1) | 120 (38.2) |
| Comorbidity, n (%) | |||
| Chronic heart failure | 19 (5.4) | 10 (7.1) | 53 (16.9) |
| Ischaemic heart disease | 40 (11.3) | 23 (16.4) | 64 (20.4) |
| Atrial fibrillation | 19 (5.4) | 12 (8.6) | 41 (13.1) |
| Stroke/TIA | 27 (7.6) | 9 (6.4) | 35 (11.2) |
| Hypertension | 193 (54.4) | 69 (49.3) | 176 (56.1) |
| Depression | 61 (17.2) | 39 (27.9) | 52 (16.6) |
| Anxiety | 38 (10.7) | 17 (12.1) | 57 (18.2) |
| Diabetes | 55 (15.5) | 24 (17.1) | 55 (17.5) |
| Osteoporosis | 22 (6.2) | 16 (11.4) | 35 (11.2) |
| Cancer | 26 (7.3) | 20 (14.3) | 52 (16.6) |
| Combined measures, n (%) | |||
| Cardiac disease | 68 (19.2) | 32 (22.9) | 103 (32.8) |
| Depression/anxiety | 74 (20.9) | 40 (28.6) | 83 (26.4) |
| N=809 | Exacerbations in 2022, n=140 | Deceased by 2022, n=314 | ||
|---|---|---|---|---|
| Unadjusted | Adjusted | Unadjusted | Adjusted | |
| RRR (95% CI) | RRR (95% CI) | RRR (95% CI) | RRR (95% CI) | |
| Comorbidity | ||||
| Chronic heart failure | 1.36 (0.61 to 3.01) | 0.88 (0.34 to 2.25) | 3.59 (2.07 to 6.22) | 2.69 (1.36 to 5.33) |
| Ischaemic heart disease | 1.57 (0.90 to 2.74) | 1.33 (0.71 to 2.47) | 2.04 (1.32 to 3.15) | 1.30 (0.78 to 2.17) |
| Atrial fibrillation | 1.65 (0.78 to 3.51) | 1.95 (0.81 to 4.73) | 2.65 (1.50 to 4.68) | 1.41 (0.70 to 2.84) |
| Stroke/TIA | 0.84 (0.38 to 1.85) | 0.79 (0.34 to 1.84) | 1.54 (0.90 to 2.62) | 1.52 (0.80 to 2.87) |
| Hypertension | 0.82 (0.55 to 1.22) | 0.77 (0.48 to 1.23) | 1.08 (0.79 to 1.47) | 0.93 (0.63 to 1.37) |
| Depression | 1.86 (1.17 to 2.96) | 1.95 (1.13 to 3.39) | 0.96 (0.64 to 1.44) | 0.66 (0.39 to 1.11) |
| Anxiety | 1.16 (0.63 to 2.13) | 0.74 (0.35 to 1.53) | 1.86 (1.19 to 2.90) | 3.71 (2.06 to 6.87) |
| Diabetes | 1.13 (0.67 to 1.91) | 1.46 (0.80 to 2.65) | 1.16 (0.77 to 1.75) | 1.22 (0.74 to 2.01) |
| Osteoporosis | 1.95 (0.99 to 3.85) | 1.61 (0.75 to 3.43) | 1.90 (1.08 to 3.32) | 1.00 (0.53 to 1.90) |
| Cancer | 2.13 (1.14 to 3.98) | 1.64 (0.84 to 3.22) | 2.54 (1.54 to 4.20) | 2.52 (1.42 to 4.46) |
| Combined measures | ||||
| Cardiac disease | 1.26 (0.78 to 2.03) | 1.22 (0.71 to 2.08) | 2.08 (1.45 to 2.97) | 1.68 (1.10 to 2.58) |
| Depression/anxiety | 1.44 (0.88 to 2.37) | 1.44 (0.88 to 2.36) | 1.37 (0.95 to 1.96) | 1.82 (1.19 to 2.78) |
| Covariates | ||||
| Exacerbation in 2014 | 3.67 (2.40 to 5.63) | 2.74 (1.71 to 4.39) | 2.55 (1.79 to 3.62) | 1.89 (1.25 to 2.87) |
| Sex, female | 1.13 (0.76 to 1.68) | 0.93 (0.59 to 1.46) | 0.77 (0.57 to 1.05) | 0.67 (0.46 to 0.99) |
| CAT-score in 2014 | 1.08 (1.05 to 1.10) | 1.06 (1.03 to 1.09) | 1.07 (1.05 to 1.09) | 1.07 (1.04 to 1.09) |
| Education, high | 1.20 (0.81 to 1.78) | 1.39 (0.90 to 2.15) | 0.86 (0.63 to 1.17) | 1.02 (0.70 to 1.48) |
| Smoking | ||||
| Former smoker | 0.79 (0.31 to 2.03) | 0.91 (0.33 to 2.47) | 1.44 (0.51 to 2.57) | 1.40 (0.56 to 3.54) |
| Current smoker | 0.87 (0.33 to 2.29) | 0.93 (0.32 to 2.66) | 1.28 (0.56 to 2.93) | 1.71 (0.65 to 4.48) |
| Multilevel modelling | ||||
| Variance (95% CI) | 0.08 (0.01 to 0.73) | |||
| Intraclass correlation coefficient | 0.024 | |||
| N=495 | Exacerbations in 2022 | |
|---|---|---|
| Unadjusted | Adjusted | |
| OR (95% CI) | OR (95% CI) | |
| Comorbidity | ||
| Chronic heart failure | 1.30 (0.57 to 2.93) | 0.80 (0.29 to 2.24) |
| Ischaemic heart disease | 1.60 (0.90 to 2.84) | 1.62 (0.84 to 3.12) |
| Atrial fibrillation | 1.62 (0.75 to 3.50) | 2.46 (0.97 to 6.29) |
| Stroke/TIA | 0.81 (0.36 to 1.80) | 0.72 (0.29 to 1.77) |
| Hypertension | 0.83 (0.55 to 1.23) | 0.79 (0.48 to 1.30) |
| Depression | 1.89 (1.17 to 3.04) | 2.24 (1.21 to 4.15) |
| Anxiety | 1.15 (0.62 to 2.16) | 0.63 (0.28 to 1.44) |
| Diabetes | 1.13 (0.66 to 1.93) | 1.42 (0.80 to 2.65) |
| Osteoporosis | 2.04 (1.01 to 4.11) | 1.57 (0.69 to 3.55) |
| Cancer | 2.18 (1.14 to 4.14) | 1.39 (0.66 to 2.92) |
| Combined measures | ||
| Cardiac disease* | 1.25 (0.77 to 2.04) | 1.36 (0.77 to 2.39) |
| Depression/anxiety | 1.53 (0.97 to 2.42) | 1.49 (0.88 to 2.54) |
| Covariates | ||
| Exacerbation in 2014 | 3.76 (2.42 to 5.85) | 2.92 (1.78 to 4.77) |
| Sex, female | 1.12 (0.75 to 1.68) | 0.99 (0.61 to 1.61) |
| CAT-score in 2014 | 1.08 (1.05 to 1.11) | 1.07 (1.03 to 1.10) |
| Education, high | 1.20 (0.80 to 1.79) | 1.45 (0.92 to 2.31) |
| Smoking | ||
| Former smoker | 0.79 (0.30 to 2.05) | 1.00 (0.34 to 2.94) |
| Current smoker | 0.87 (0.33 to 2.33) | 0.96 (0.31 to 2.98) |
| Multilevel modelling | ||
| Variance (95% CI) | 0.14 (0.01 to 1.76) | |
| Intraclass correlation coefficient | 0.041 | |
- —Vetenskapsrådet -the Swedish Research Council
- —Swedish Heart and Lung Association
- —Swedish Heart Lung Foundation
- —Bror Hjerpstedt Foundation
- —ALF funding Region Örebro County
- —Centre for Clinical Research, Region Värmland, Sweden
- —Swedish Asthma and Allergy Association
- —Centre for Clinical Research, Region Dalarna, Sweden
- —Regional Research Council Mid Sweden
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Pediatric health and respiratory diseases · Respiratory and Cough-Related Research
Introduction
Patients with chronic obstructive pulmonary disease (COPD) and comorbidity face increased risks of exacerbations, mortality and poor quality of life.1 On average, a patient with COPD has five other chronic diseases.2 For example, depression and cancer have been associated with frequent exacerbations and increased healthcare costs.3 4 Anxiety, cancer and cardiovascular disease are associated with a higher risk of mortality.5 Body mass index (BMI) is also associated with COPD outcomes. For mortality, the relationship with BMI is U-shaped, with higher risk for those with low or high BMI.6 For exacerbations, low BMI has been associated with increased risk.7
In Sweden, most patients with COPD, even those with severe COPD and comorbidity, are mainly managed in primary care.8 Primary care centres may have differences in location (rural or urban, with variation in socioeconomic characteristics of patients), number of patients, use of locum physicians and access to specialist primary care nurses for assessment and management of patients with COPD (including nurse-led COPD clinics within the healthcare centre). Previous research has found that only a small part of the variation in health outcomes can be attributed to differences in staffing or other aspects of healthcare centres in countries outside of Scandinavia.9 The degree of variation between primary healthcare centres in Sweden for COPD outcomes is unclear.
This study aims to examine the associations of comorbid diseases and BMI with subsequent exacerbations and mortality in patients with COPD, and specifically to assess the variation of these associations between healthcare centres using multilevel modelling, during an 8-year follow-up.
Methods
Study population and design
The study population consisted of the second PRAXIS COPD cohort (https://praxisstudien.com/). It was created in 2014, by inviting randomly selected patients who were treated at 76 primary healthcare centres in central Sweden with a physician’s diagnosis of COPD (ICD-10 code J44) in their medical records between 2007 and 2010, and aged ≤75 years. There were no other exclusion criteria. Among 2156 patients who were invited to the study, 1267 (59%) consented and returned a self-completion questionnaire in 2014 (figure 1). Some 1163 patients agreed to a medical record review (2004–2014) performed by two research nurses using a detailed template. In 2022, the 795 (68%) patients who were alive were invited to participate in a follow-up, and 541 (68%) completed the second questionnaire. The participating healthcare centres filled in a questionnaire in 2012 about the characteristics of their centre.
Flow chart of the study population. BMI body mass index; CAT, COPD Assessment Test; COPD, chronic obstructive pulmonary disease.
This was a cohort study using multilevel modelling with follow-up from 2014 to 2022. Individuals with missing data for covariates (N=97) were excluded from the analysis; for details, see figure 1.
Setting and exposures
Primary healthcare centres
The healthcare centres were in seven county councils in central Sweden, where the largest city has approximately 250 000 inhabitants. Both private and state-operated practices were included. Patients were assigned to the centre where they were listed at study start in 2014. Data on centre characteristics such as number of patients, presence of nurse-led COPD clinic and guidelines for COPD were obtained from the healthcare centre questionnaire in 2012.
Comorbidity
Comorbid diseases between 2004 and 2014 were identified in the medical record review by the ICD-10 codes or as free text. Type 1 and 2 diabetes were recorded together as diabetes.
Body mass index
Self-reported weight and height were obtained from the questionnaire in 2014. BMI was calculated as the ratio between weight in kilograms (kg) and height in metres squared (m^2^).
Outcomes
Information on exacerbations during the previous 6 months was obtained from the 2022 questionnaire and defined as any unscheduled/emergency visit to primary or secondary care, and/or use of oral steroids, and/or antibiotics due to worsening of COPD symptoms. Data on mortality were supplied by Statistics Sweden. As the mortality rate was relatively high in the study population, mortality was included as an outcome to consider competing risks, rather than excluding those who had died. Therefore, the outcome variable had three categories: alive without any reported exacerbation during the previous 6 months at follow-up in 2022, alive with at least one reported exacerbation during the previous 6 months at follow-up in 2022 or died by 2022.
Covariates
COPD exacerbations in 2014 were defined in the same way as described for 2022. Data were obtained from the 2014 questionnaire. To measure COPD-specific health status, we used the COPD Assessment Test (CAT),10 which includes eight items on symptoms scored by the patient on a scale from 0 to 5: the sum may vary between 0 and 40. A higher score indicates worse health status. We used the CAT score at baseline in 2014 as a measure of pre-existing COPD severity.
Data on smoking and attained level of education were obtained from the 2014 questionnaire. Smoking was categorised as never smoker, former smoker or current smoker (daily or occasionally). Education, as a marker of socioeconomic characteristics, was dichotomised to identify at least 2 years of continued education beyond the 9 years of Swedish compulsory school or less.
Statistical analyses
Categorical variables were described using frequencies and percentages, while continuous variables were described using means and SD or medians and 25–75 IQR. The χ² test and Student’s t-test were used to compare differences between the participants and those lost to follow-up.
We used multilevel multinomial logistic regression to assess the risk of exacerbations and mortality, including the variation between the primary healthcare centres. To evaluate variation in outcomes across centres, we fitted three models: (1) an empty model without covariates, (2) a model including all comorbid diseases and individual characteristics and (3) a model additionally including centre characteristics. The variance from each model was used to calculate the intraclass correlation coefficient (ICC) which quantifies the proportion of variance that is attributed to the variability between the healthcare centres.11 ICC was calculated as: variance/(variance+(π^2^/3)). The multinomial component of the model compared the likelihood of the two outcomes, alive with at least one reported exacerbation in 2022 or died by 2022, against the reference category of being alive with no reported exacerbations in 2022. We estimated relative risk ratios (RRRs) with 95% CIs. The comorbid diseases were analysed separately without adjustment, and in the main analysis, all comorbid diagnoses were included together with sex, age, smoking, attained level of education, BMI, CAT score and exacerbations in 2014. Chronic heart failure, ischaemic heart disease and atrial fibrillation were included as separate exposure variables in the main analysis. In a second analysis, they were combined into one variable: cardiac disease. Similarly, anxiety and depression were analysed separately in the main analysis, and as a combined variable (depression or anxiety) in a second analysis. Additional analyses were stratified by sex, and differences assessed by multiplicative interaction testing.
BMI was modelled as a continuous variable with restricted cubic splines with three knots positioned at the 10th, 50th and 90th percentiles, to allow for a non-linear relationship with the outcomes and to provide comprehensive adjustment, as use of a categorical variable may lead to inaccurate estimations.12 Age was modelled using age and age squared. The CAT score was modelled as a continuous variable.
Sensitivity analyses
We performed three sensitivity analyses. First, to examine the effect of missing data, we compared RRRs obtained from unadjusted analysis including and excluding individuals with missing data from one or more covariates. Second, since the main analysis included deceased individuals, we performed multilevel logistic regression analysis to assess the risk of exacerbation only among those who remained alive. Third, small group sizes (<5 patients per centre) may have a disproportionate influence on the estimates, so we performed an analysis excluding individuals who belonged to centres with fewer than five individuals.13
Data management and statistical analysis were performed using Stata V.18.
Patient and public involvement
There was no specific patient or public involvement in planning or execution of the study.
Results
Population and healthcare centre characteristics
At study start in 2014, 59% of the invited patients completed the questionnaire. The patients who did not respond tended to be younger, with a mean age of 65.4 years compared with 67.5 years among respondents (p<0.001). At follow-up in 2022, 68% of the survivors completed the new questionnaire. While there were no statistically significant differences in age, sex, education, BMI or number of comorbid diseases between the participating patients and the non-participants, the participating patients had a slightly lower mean CAT score in 2014 than the non-participants: 14 compared with 15, respectively (p=0.04).
The final study population consisted of 809 patients with COPD, attending 70 primary healthcare centres. The centres had between 2000 and 20 300 registered patients (median 9605, IQR 6612–12 400). The majority of centres, 60 of 70 (86%), had nurse-led COPD clinics and 61 (87%) had local or regional guidelines for management of COPD. The median number of participating patients per healthcare centre was 12, IQR 10–14 and range 1–18. There were five centres with fewer than five participants. The patients’ median age in 2014 was 69 (IQR 64–72), and 53.5% were female (see table 1).
Variation by healthcare centres
The variance in the unconditional (empty) model was 0.04 (95% CI 0.01 to 1.20), with ICC 0.012. When comorbidity and other patient characteristics were added to the model, the variance was 0.08 (95% CI 0.01 to 0.73), giving an ICC of 0.024. When centre characteristics (existence of nurse-led COPD clinic) were added, the variance was 0.06 (95% CI 0.01 to 1.13), ICC 0.018. This indicates that only 1.2%–2.4% of the risk of exacerbations or mortality is explained by differences between healthcare centres and, thus, the variability in outcomes between centres was small.
Exacerbations and mortality
The adjusted RRRs were obtained by mutually adjusting for all comorbid diseases as well as age, sex, smoking, attained level of education, BMI, CAT score and exacerbations in 2014 (see table 2). Patients with a history of depression had a statistically significantly increased risk ratio for having at least one exacerbation during the previous 6 months in 2022, compared with having no recent exacerbations, RRR 1.95 (95% CI 1.13 to 3.39). Exacerbations in 2014 were also associated with an increased risk of subsequent exacerbations, RRR 2.74 (95% CI 1.71 to 4.39). We did not find any statistically significant associations between cardiac disease, diabetes, smoking or education and risk of exacerbations.
Predicted probabilities with 95% CIs for outcomes by body mass index with the other variables fixed at their means (fully adjusted model) in (a) the whole study population, n=809, (b) men, n=376 and (c) women, n=433. The probabilities for the three outcomes sum up to 1.0.
For patients with COPD and a history of anxiety or cancer, we found statistically significantly increased risk ratios for mortality, compared with having no recent exacerbations. When stratified by sex, women had an RRR of 3.31 (95% CI 1.64 to 6.68) and men 4.62 (95% CI 1.42 to 15.09) for mortality associated with anxiety in 2014, but interaction testing did not indicate statistically significant effect modification by sex. The presence of cardiac disease in 2014, especially chronic heart failure, was associated with increased mortality risk, RRR 2.69 (95% CI 1.36 to 5.33). In unadjusted analyses, there were increased risks for all cardiac diseases, but after adjustment, it remained statistically significant only for chronic heart failure. We also found a raised risk of mortality for those who had exacerbations in 2014. There were no statistically significant associations with mortality for smoking or education.
The risk of mortality was found to be increased for both lower and higher values of BMI (figure 2a). For exacerbations, there was a slightly decreased risk with lower BMI. When stratified by sex, the U-shaped association with mortality was more evident for men than women, as the increased risk of mortality at higher BMI was less prominent among women (figure 2b,c).
Sensitivity analyses
The first sensitivity analysis found that results were consistent when the sample with complete data for covariates was compared with all available participants (data not shown). Second, multilevel logistic regression (for the surviving subpopulation) produced similar results for exacerbations in 2022 as the multilevel multinomial regression, although the risk estimates were of slightly, but not significantly, higher magnitude for positive associations, and of slightly lower magnitude for inverse associations (table 3). Also, the risk of exacerbations in 2022 increased with declining BMI for this population (online supplemental figure 1). Third, the results were consistent after removing the five centres with <5 participants.
Discussion
The main finding of this cohort study with an 8-year follow-up was that the variance between healthcare centres for COPD outcomes was small and individual patient factors appeared to be of greater importance. Patients with COPD and a history of depression had a doubled risk of new exacerbations, and those with a history of anxiety had an almost four times increased risk of mortality. The selection effect of mortality in a panel study may affect the magnitude of some associations, and its influence on results must be considered carefully.
Our study included patients from 70 primary care centres with differences in size, location, staffing and proximity to secondary care. The majority had nurse-led COPD clinics and local or regional guidelines for management of COPD. Despite this, the estimated variability in COPD outcomes between centres was small. A possible interpretation is that management of patients with COPD in primary care in Sweden is rather uniform and standardised among the centres included in this study. A previous Swedish study reported that structured management of patients with COPD in primary care was increasing during 1999–2009, and patients who attended healthcare centres with nurse-led COPD clinics had fewer exacerbations and hospital admissions.14 However, our finding of small variability between centres aligns with previous studies of low variability in primary care. A Canadian study reported variability of 1%–3% between primary care clinics for recognition and treatment of depression.15 A Spanish study of variability in health outcomes and costs found that less than 3% of the prescriptions, 5% of referrals and 9% of visits to primary care physicians were attributed to the differences between healthcare centres.9 Although these earlier studies are from different countries and diagnoses, the results seem consistent and support the finding that outcomes are explained more comprehensively by individual patient factors. Our use of multilevel modelling in this context can provide more effective adjustment for centre characteristics, reducing the risk of residual confounding, while improving accuracy by allowing estimates of associations between patient characteristics and outcomes to vary by centre.
Comorbid depression has been associated with increased risk of both exacerbations and mortality in patients with COPD.3 16 17 Anxiety has been identified as one of twelve diseases predictive of mortality in patients with COPD, especially in women.5 In some studies, anxiety has been associated with increased risk of exacerbations, while others have not shown an association.3 17 18 We found that depression was associated with an increased risk of recent exacerbations in the patients surviving to 2022, but there was no association with mortality. Our study indicated an increased risk of mortality in both men and women associated with anxiety. Anxiety is common in patients with multimorbidity, and the high magnitude risk estimate we found might reflect anxiety as an independent risk factor or as a marker of chronic disease severity and worse health status.19 Anxiety and depression often co-occur in patients with COPD.20 When we repeated the analysis with anxiety and depression combined as one variable, we found increased risks for both mortality and future exacerbations, although statistically significant results were only seen for mortality. A potential reason for the somewhat divergent results may be that anxiety and depression diagnoses were identified in the medical record review, so we have no knowledge of the diagnostic criteria, or the duration of symptoms. Similarly, we could only identify exacerbations during the previous 6 months through the questionnaire 2022, thereby likely only identifying surviving participants with more frequent exacerbations. We have no knowledge of exacerbations occurring between 2014 and 2022, and participants who died before 2022 are likely to have had unreported exacerbations prior to their death. However, by modelling both exacerbations and mortality as outcomes in the same model, it was possible to assess markers of adverse outcomes more comprehensively than if those who died were simply excluded.
Comorbid cardiovascular disease has been associated with increased mortality, and chronic heart failure as well with an increased risk of exacerbations.3 21 In our study, we found increased risks for mortality associated with all cardiac diseases in the univariate analyses. The risk remained statistically significant only for heart failure and the combined cardiac disease variable in the adjusted models, due to multicollinearity, as patients often have more than one cardiac diagnosis: the combined cardiac disease variable may give an indication of risk magnitude that is more readily interpretable.
Our finding that a history of exacerbations is associated with both increased risk of future exacerbations and mortality is consistent with previous studies, including those that used spirometry.3 22 Even though we were unable to distinguish between severe and moderate exacerbation episodes in our study, the associations were statistically significant. The most recent years of our follow-up period were during the COVID-19 pandemic, and this may have influenced the results. During the pandemic, there was an increase in prescriptions of steroids and antibiotics used for COPD exacerbations, and this prescription pattern may have been reflected in the information collected in 2022.23 Other exposures that have changed over time include the prevalence of smoking. Prior studies have reported heterogeneous results for the association of smoking with exacerbations, and we found no association between smoking and risk of exacerbations.24 25
For BMI, we observed a U-shaped association with mortality, as reported in a recent meta-analysis.6 For exacerbations, we did not find any difference in risk between normal and high BMI, consistent with previous research.7 However, an increased risk of exacerbations in underweight patients has been reported,7 which we did not find in the multinomial logistic regression where mortality was one of the outcome categories. When analysing the survivors separately, without having mortality as a competing risk, we did find an increased risk of exacerbations associated with lower BMI. Thus, the patients with low BMI in 2014, who survived until 2022, appear to have an increased risk of exacerbations that was not seen in the entire sample as low BMI was a greater risk for mortality.
The clinical relevance of our findings is the importance of individualised care of patients with COPD in primary care, as in a uniform primary care system, individual patient factors such as comorbidity and BMI may be the main drivers of adverse outcomes. This includes identifying and treating mental health conditions (including identifying somatic risks that underlie these conditions) and closer monitoring of patients with heart failure or previous exacerbations could help prevent poor outcomes.
Strengths and limitations
This study had more than 800 randomly selected patients with COPD from primary care with an 8-year follow-up. The use of both medical record reviews and questionnaires for data collection enabled us to use the combination of prospectively recorded diagnoses with the patients’ own experience of their health. Another strength was the use of multilevel multinomial logistic regression for the analysis. Multilevel modelling accounts for differences between healthcare centres more effectively than some other methods, and multinomial logistic regression allowed mortality to be modelled as a competing outcome. Considering the high mortality rate at follow-up (31%), it was important to account for the role of mortality in shaping the results. A sensitivity analysis, including only the survivors, found similar but subtly different results for associations with exacerbations in 2022 for comorbidity and previous exacerbations. The choice of study population at follow-up in a panel study may thus influence the magnitude of the results, although the direction of associations remained similar in this study. This emphasises the importance of considering the influence of mortality in a panel study, as selection effects may alter the magnitude of some associations.
There are some potential limitations. The non-response rate in 2014 was 41%, and 32% at follow-up in 2022. The respondents in 2014 were somewhat older than those who did not respond, and the respondents in 2022 may have had a slightly better COPD-specific health status in 2014 (14 compared with 15), although the suggested minimal clinically important difference for CAT is two units.26 Non-response may be a cause of potential selection bias and may also limit variability between centres. The loss of patients in the main analysis due to missing data for covariates was 11%. To examine the consequences, we performed a sensitivity analysis, with consistent results. Data on exacerbations were obtained from the questionnaires, and to reduce the risk of recall bias, a period of 6 months was used. Hence, we lack knowledge of exacerbations occurring for most of the time between 2014 and 2022, and participants with frequent exacerbations during this time may have died prior to 2022. Thus, the estimates of risk of exacerbation should only be understood as the risk of exacerbation in 2022, among patients who were still alive. Similarly, we have no knowledge of comorbid conditions that developed during the follow-up, or treatment compliance. Height and weight were self-reported, but BMI based on self-reported measures has been found to have acceptable agreement with measured BMI in Sweden.27
Some participants may have changed healthcare centres during follow-up, possibly making the estimation of variability among the healthcare centres less precise. Finally, while healthcare centres in more disadvantaged areas of Sweden may have been under-represented, our study population likely broadly represents Swedish patients with a diagnosis of COPD. Patients may have had respiratory symptoms for a long time before being diagnosed with COPD, but having comorbidity might lead to an earlier diagnosis.28 Thus, there is a possibility of selection bias: individuals with other pre-existing chronic diseases are more likely to seek care and receive a COPD diagnosis.
Conclusions
The variability between healthcare centres for the likelihood of COPD exacerbations and mortality is small, indicating that individual patient factors may be of more importance for COPD outcomes than differences in primary care settings. It is of note that a history of anxiety was associated with future excess mortality risk, and this finding should be investigated further for replication. As expected, pre-existing cardiovascular disease, particularly heart failure, is associated with increased mortality risk in patients with COPD.
Supplementary material
10.1136/fmch-2025-003713online supplemental file 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Smith MC Wrobel JP Epidemiology and clinical impact of major comorbidities in patients with COPD Int J Chron Obstruct Pulmon Dis 201498718810.2147/COPD.S 4962125210449 PMC 4154888 · doi ↗ · pubmed ↗
- 2Divo MJ Celli BR Poblador-Plou B et al Chronic Obstructive Pulmonary Disease (COPD) as a disease of early aging: Evidence from the Epi Chron Cohort P Lo S One 201813 e 019314310.1371/journal.pone.019314329470502 PMC 5823454 · doi ↗ · pubmed ↗
- 3MüllerováH Shukla A Hawkins A et al Risk factors for acute exacerbations of COPD in a primary care population: a retrospective observational cohort study BMJ Open 20144 e 00617110.1136/bmjopen-2014-006171 PMC 427567225524545 · doi ↗ · pubmed ↗
- 4Husaini B Levine R Lammers P et al Smoking, depression, and hospital costs of respiratory cancers: Examining race and sex variation Fam Med Community Health 20175294210.15212/FMCH.2017.010929057243 PMC 5648368 · doi ↗ · pubmed ↗
- 5Divo M Cote C de Torres JP et al Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease Am J Respir Crit Care Med 20121861556110.1164/rccm.201201-0034 OC 22561964 · doi ↗ · pubmed ↗
- 6Tenda ED Henrina J Setiadharma A et al The impact of body mass index on mortality in COPD: an updated dose-response meta-analysis Eur Respir Rev 20243323026110.1183/16000617.0261-202339603663 PMC 11600125 · doi ↗ · pubmed ↗
- 7Wang M Ni X Yu F Impact of Body Mass Index on Risk of Exacerbation in Patients With COPD: A Systematic Review and Meta-Analysis Chronic Obstr Pulm Dis 2024115243310.15326/jcopdf.2024.050739213382 PMC 11548972 · doi ↗ · pubmed ↗
- 8National board of health and welfare: nationella riktlinjer för astma och KOL 2020 Availablehttp://www.socialstyrelsen.se