Circulating biomarkers in subjects with progressive pulmonary fibrosis: data from the INBUILD trial
Toby M. Maher, R. Gisli Jenkins, Francesco Bonella, Shervin Assassi, Claudia Diefenbach, Carina Ittrich, Klaus B. Rohr, Martin Kolb

TL;DR
The study found that the drug nintedanib lowers specific blood markers linked to lung damage in patients with progressive pulmonary fibrosis.
Contribution
The study shows that nintedanib reduces circulating levels of epithelial dysfunction markers like CA-125 in progressive pulmonary fibrosis patients.
Findings
Baseline s-ICAM levels were significantly associated with faster FVC decline and ILD progression or death.
Nintedanib significantly reduced levels of KL-6, SP-D, CA-125, and CA19-9 compared to placebo.
16.4% of nintedanib's effect on FVC improvement was mediated by reduced CA-125 levels.
Abstract
We investigated the prognostic potential of circulating biomarkers at baseline and the effects of nintedanib on changes in these biomarkers in subjects with progressive pulmonary fibrosis (PPF). In the INBUILD trial, subjects with PPF received nintedanib (n=332) or placebo (n=331). Associations between biomarker levels at baseline and the rate of forced vital capacity (FVC) decline (mL·year−1) over 52 weeks, time to interstitial lung disease (ILD) progression (absolute decline in FVC % predicted ≥10%) or death over 52 weeks, time to first acute exacerbation or death over the whole trial, and time to death over the whole trial were assessed in the placebo group. Changes in adjusted mean levels of biomarkers in the nintedanib and placebo groups were assessed using linear mixed models for repeated measures. Biomarker data were log2 transformed prior to analysis. Analyses were corrected…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
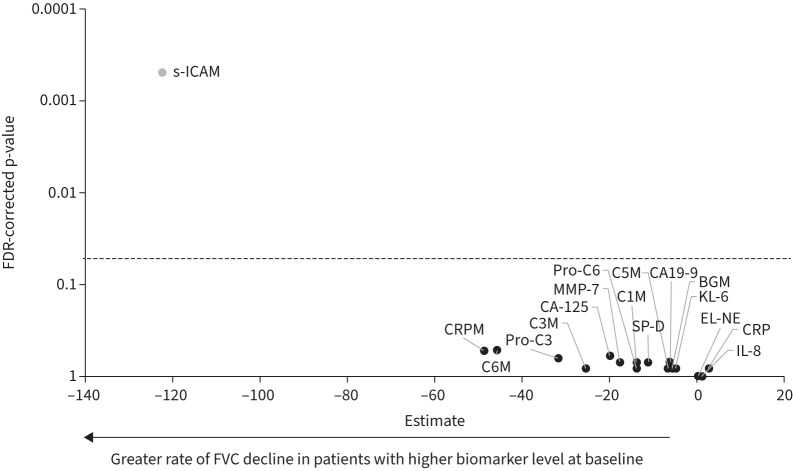 FIGURE 1
FIGURE 1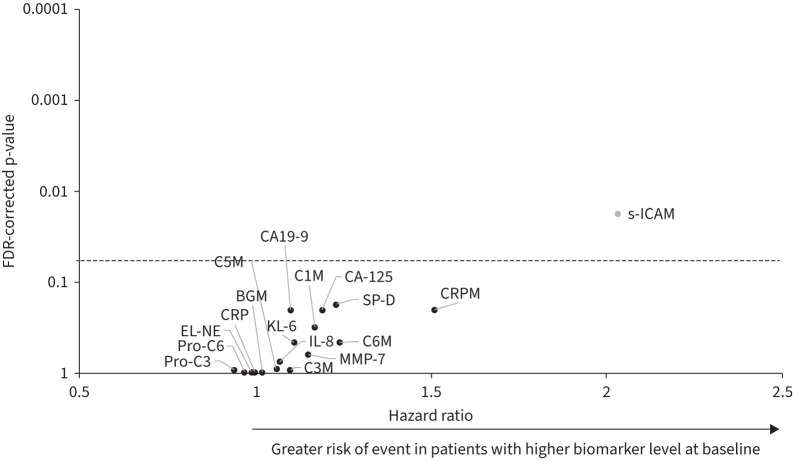 FIGURE 2
FIGURE 2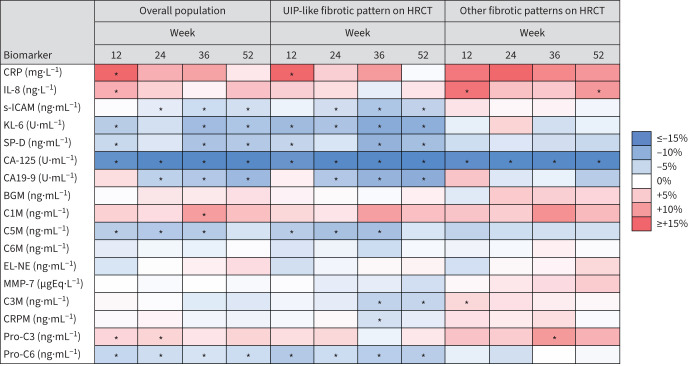 FIGURE 3
FIGURE 3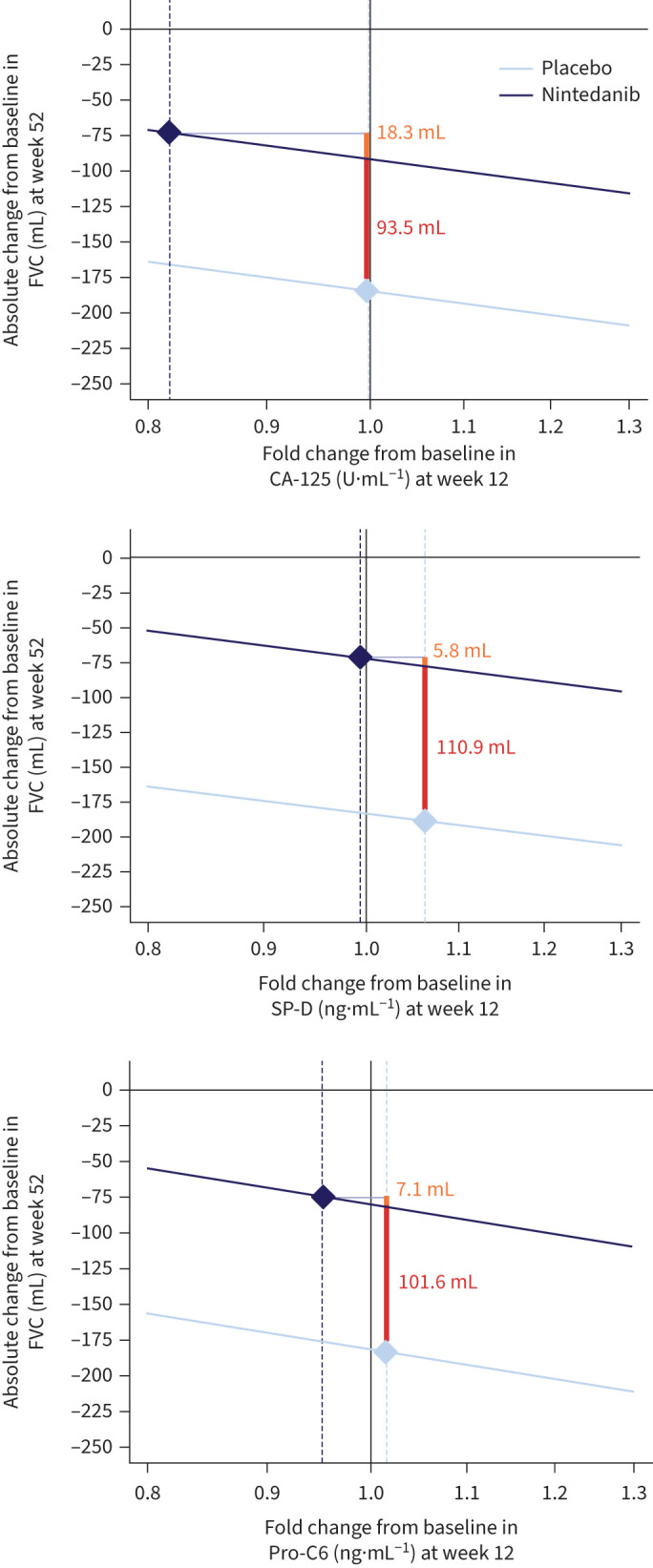 FIGURE 4
FIGURE 4| Overall population | UIP-like fibrotic pattern on HRCT | Other fibrotic patterns on HRCT | ||||
|---|---|---|---|---|---|---|
| Nintedanib | Placebo | Nintedanib | Placebo | Nintedanib | Placebo | |
|
| 1033±1016 | 1035±878 | 943±843 | 894±756 | 1182±1243 | 1274±1012 |
|
| 772±543 | 732±528 | 715±436 | 700±501 | 867±677 | 787±569 |
|
| 19.2±16.9 | 21.8±20.6 | 19.1±14.1 | 21.0±20.6 | 19.5±20.8 | 23.3±20.6 |
|
| 48.7±82.0 | 47.6±83.4 | 53.4±89.3 | 45.3±73.1 | 40.4±66.8 | 51.4±98.2 |
|
| 6.8±12.9 | 6.1±13.1 | 7.7±15.4 | 6.7±15.8 | 5.3±6.6 | 5.1±6.1 |
|
| 29.8±36.6 | 33.5±108.1 | 31.1±38.7 | 36.5±132.2 | 27.6±32.9 | 28.4±42.5 |
|
| 714±230 | 710±242 | 707±213 | 681±205 | 727±257 | 758±289 |
|
| 15.1±8.8 | 16.2±10.0 | 14.1±8.5 | 16.2±10.3 | 16.6±9.2 | 16.3±9.6 |
|
| 48.1±37.0 | 49.5±39.5 | 47.8±36.1 | 49.0±41.8 | 48.6±38.5 | 50.4±35.6 |
|
| 14.9±5.1 | 14.9±4.5 | 15.5±5.8 | 15.0±4.9 | 13.8±3.5 | 14.9±3.7 |
|
| 8.1±4.2 | 8.1±3.9 | 8.2±4.3 | 8.5±4.2 | 7.8±4.2 | 7.4±3.3 |
|
| 30.9±17.9 | 29.5±12.7 | 31.8±19.8 | 29.7±13.4 | 29.5±14.0 | 29.0±11.6 |
|
| 6.7±6.6 | 7.5±6.9 | 6.2±6.2 | 7.5±7.2 | 7.6±7.3 | 7.4±6.5 |
|
| 10.9±5.7 | 10.9±5.5 | 10.9±5.2 | 10.8±5.0 | 10.9±6.5 | 11.2±6.2 |
|
| 11.0±3.5 | 11.5±4.1 | 11.0±3.6 | 11.3±3.9 | 10.9±3.4 | 11.7±4.5 |
|
| 13.4±6.0 | 14.1±6.5 | 13.7±6.3 | 14.6±7.2 | 13.0±5.4 | 13.3±5.1 |
|
| 9.7±3.6 | 9.7±4.0 | 9.7±3.8 | 9.6±4.1 | 9.6±3.2 | 9.8±3.9 |
- —Boehringer Ingelheimhttp://dx.doi.org/10.13039/100001003
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
The term progressive pulmonary fibrosis (PPF) is generally used to describe progressive lung fibrosis in a patient with an interstitial lung disease (ILD) other than idiopathic pulmonary fibrosis (IPF) [1]. Although different criteria are used to define PPF, based on varying parameters of decline in lung function, worsening of symptoms and worsening of radiological abnormalities [1–4], progression of pulmonary fibrosis is invariably associated with poor outcomes [5, 6].
The development of lung fibrosis involves interplay among inflammatory, immune and fibrotic mechanisms. The current paradigm proposes that repeated epithelial injury results in the release of pro-inflammatory and pro-fibrotic mediators, the differentiation of fibroblasts into myofibroblasts and excess deposition of extracellular matrix (ECM), which further activates fibroblasts, ultimately leading to a self-sustaining process of fibrosis [7]. Nintedanib, an intracellular inhibitor of tyrosine kinases, shows both anti-inflammatory and antifibrotic effects in nonclinical studies [8]. In placebo-controlled clinical trials, nintedanib slowed the rate of decline in forced vital capacity (FVC) in subjects with IPF [9], ILD associated with systemic sclerosis [10] and PPF [2].
The clinical course of PPF is variable [11, 12]. Thus, the identification of circulating biomarkers prognostic of short-term outcomes, or indicative of response to nintedanib in an individual with PPF, would be of clinical value. In this analysis, we used data from the INBUILD trial to evaluate the prognostic potential of circulating biomarkers and the effects of nintedanib on these biomarkers in subjects with PPF.
Methods
Trial design
The design of the INBUILD trial (NCT02999178) has been published [2]. In summary, subjects had an ILD other than IPF, an extent of fibrosis on high-resolution computed tomography (HRCT) >10% and FVC ≥45% predicted. Subjects met ≥1 of the following criteria for ILD progression within the prior 24 months despite management in clinical practice: relative decline in FVC % predicted ≥10%; relative decline in FVC % predicted ≥5–<10% and increased extent of fibrosis on HRCT and/or worsened respiratory symptoms; worsened respiratory symptoms and increased extent of fibrosis on HRCT [2]. Subjects were randomised to receive nintedanib or placebo, stratified by fibrotic pattern on HRCT (usual interstitial pneumonia (UIP)-like fibrotic pattern or other fibrotic patterns).
The INBUILD trial was carried out in compliance with the principles of the Declaration of Helsinki and the Harmonised Tripartite Guideline for Good Clinical Practice from the International Conference on Harmonisation and was approved by local authorities. All subjects provided written informed consent before trial entry.
Blood sample collection and biomarker analysis
Samples for biomarker analysis were collected at baseline and at weeks 12, 24, 36 and 52. Serum samples were prepared using anticoagulant-free, gel-containing serum separation tubes, which were left to clot for ∼1 h at room temperature. Plasma samples were prepared using K_2_ EDTA plasma tubes. Serum and plasma were separated by centrifugation and aliquoted prior to freezing. Krebs von den Lungen-6 (KL-6), surfactant protein D (SP-D), CA-125 and CA19-9 were assessed as biomarkers of epithelial dysfunction. C-reactive protein (CRP), interleukin-8 (IL-8) and soluble intercellular adhesion molecule (s-ICAM) were assessed as biomarkers of inflammation. Biglycan degraded by MMP (BGM), collagen 1 degraded by MMP-2/9/13 (C1M), collagen 3 degraded by MMP-9 (C3M), collagen 5 degraded by MMP-2/9 (C5M), collagen 6 degraded by MMP-2/9 (C6M), neutrophil-specific elastin fragments (EL-NE), MMP-7, CRPM, N-terminal propeptide of type III collagen (pro-C3) and N-terminal propeptide of type VI collagen (pro-C6) were assessed as biomarkers of ECM turnover. Commercially available ELISA methods were used to measure plasma concentrations of KL-6 and SP-D. The Sanko Junyaku Co., Ltd./EIDIA Co., Ltd test kit was used for KL-6, with the assay performed according to the manufacturer's protocol. The human SP-D ELISA test kit from Biovendor was used for SP-D. Serum concentrations of CA-125 and plasma concentrations of s-ICAM and CA19-9 were measured using an electrochemiluminescence immunoassay. Concentrations of CA-125 were assessed using the CA-125 antigen Beckman DxI 800 assay (a two-site immunoenzymatic assay). Concentrations of s-ICAM were assessed using the Vascular Injury Panel 2 (human) K15198 test kit from Meso Scale Discovery. CRP concentrations were measured via immunonephelometry using the Siemens BNII Nephelometer. IL-8 concentrations were measured using the Quantikine Human CXCL8/IL-8 enzyme immunoassay. Serum concentrations of the biomarkers of ECM turnover were measured using ELISA methods.
Statistical analyses
Spearman's correlation coefficients (rho) between FVC (mL) and concentrations of each biomarker at baseline were calculated in all patients (nintedanib and placebo). Associations between baseline biomarker levels and the following end-points were assessed in the placebo group: rate of decline in FVC (mL·year^−1^) over 52 weeks; time to ILD progression (absolute decline in FVC % predicted ≥10%) or death over 52 weeks; time to first acute exacerbation or death over the whole trial; and time to death over the whole trial. Biomarker data were not normally distributed and were log_2_ transformed prior to analysis. The rate of decline in FVC (mL·year^−1^) over 52 weeks was analysed using random coefficient regression. Estimates represented the rate of decline in FVC (mL·year^−1^) over 52 weeks associated with a difference of one in the log_2_ transformed level of the biomarker at baseline. Time to event end-points were analysed using Cox regression models. Hazard ratios (HR) represented the risk of an event associated with a difference of one in the log_2_ transformed level of the biomarker at baseline. Analyses were adjusted for baseline FVC % predicted (or FVC in mL for the rate of decline in FVC in mL·year^−1^), diffusing capacity of the lung for carbon monoxide % predicted, age, sex, HRCT pattern (UIP-like pattern or other fibrotic patterns), inclusion criteria for ILD progression and batch (for C3M, CRPM, pro-C3 and pro-C6). p-values were corrected for multiple comparisons using the Benjamini–Hochberg method [13] to control the false discovery rate (FDR) at 5%.
Changes from baseline in adjusted mean levels of biomarkers at each visit were assessed in the overall population and in subgroups by HRCT pattern using linear mixed models for repeated measures. Models included fixed categorical effects of treatment at each visit, sex, race, ILD subtype, inclusion criterion for ILD progression, batch (for C3M, CRPM, pro-C3 and pro-C6), and fixed continuous effects of the baseline value of the biomarker at each visit and age. Within−patient errors were modelled by an unstructured variance−covariance matrix. Biomarker data were log_10_ transformed before analysis.
Mediation analyses assessed the extent to which the effect of nintedanib on the change in a biomarker at week 12 was related to the effect of nintedanib on change in FVC at week 52. Biomarkers that demonstrated an indirect relationship with FVC with p<0.1 (i.e., a notable relationship between change in the biomarker and change in FVC), a negative estimated slope of the regression line with p<0.05 (i.e., a negative linear relationship between change in the biomarker and change in FVC) and a decrease with nintedanib versus placebo at week 12 with p<0.05 were included in mediation analyses. Correlations (rho) between changes in these biomarkers at weeks 12, 24, 36 and 52 and the rate of decline in FVC over 52 weeks were calculated.
Results
Subjects
A total of 663 subjects received trial medication (332 nintedanib, 331 placebo). Their baseline characteristics have been published [2]. The majority of subjects were male (53.7%) and white (73.6%). Mean±sd age was 65.8±9.8 years and mean±sd FVC was 69.0±15.6% predicted; 412 subjects (62.1%) had a UIP-like pattern on HRCT. The baseline levels of each biomarker are shown in table 1.
Prognostic value of circulating biomarkers in the placebo group
Correlations between baseline FVC (mL) and baseline concentrations of each biomarker are shown in supplementary table S1. Rates of decline in FVC (mL·year^−1^) in subgroups by baseline levels of biomarkers (based on the optimal cut-off) are shown in supplementary table S2. Only s-ICAM showed a significant (FDR-corrected p<0.05) association between continuous baseline level and the rate of decline in FVC over 52 weeks (estimate −122.4, 95% CI −179.2– −65.5) and time to ILD progression or death over 52 weeks (HR 2.03, 95% CI 1.33–3.11) (figures 1 and 2). None of the biomarkers showed a significant association between baseline level and time to first acute exacerbation or death, or death alone (supplementary figures S1 and S2). Associations between baseline biomarker levels and outcomes by fibrotic pattern on HRCT are shown in supplementary tables S3–S6. Baseline level of s-ICAM was significantly associated with the rate of decline in FVC over 52 weeks in subjects with a UIP-like pattern, but not in subjects with other patterns on HRCT (estimates of −162.9 (95% CI −246.9– −78.9) and −74.3 (95% CI −152.0–3.3), respectively).
Associations between baseline biomarker levels and rate of decline in forced vital capacity (FVC) in the INBUILD trial. Estimates represent the rate of decline in FVC (mL·year−1) over 52 weeks associated with difference of one in the log2 transformed level of the biomarker at baseline. Biomarker shown as a grey circle had a significant association between the baseline value and the outcome (FDR-corrected p<0.05). FDR: false discovery rate; KL-6: Krebs von den Lungen-6; SP-D: surfactant protein D; CRP: C-reactive protein; IL-8: interleukin-8; s-ICAM: soluble intercellular adhesion molecule; BGM: biglycan degraded by MMP; C1M: collagen 1 degraded by MMP-2/9/13; C3M: collagen 3 degraded by MMP-9; C5M: collagen 5 degraded by MMP-2/9; C6M: collagen 6 degraded by MMP-2/9; EL-NE: neutrophil-specific elastin fragments; pro-C3: N-terminal propeptide of type III collagen; pro-C6: N-terminal propeptide of type VI collagen.
Associations between baseline biomarker levels and time to ILD progression or death over 52 weeks in the INBUILD trial. Hazard ratios represent the risk of an event associated with a difference of one in the log2 transformed level of the biomarker at baseline. Biomarker shown as a grey circle had a significant association between the baseline value and the outcome (FDR-corrected p<0.05). FDR: false discovery rate; KL-6: Krebs von den Lungen-6; SP-D: surfactant protein D; CRP: C-reactive protein; IL-8: interleukin-8; s-ICAM: soluble intercellular adhesion molecule; BGM: biglycan degraded by MMP; C1M: collagen 1 degraded by MMP-2/9/13; C3M: collagen 3 degraded by MMP-9; C5M: collagen 5 degraded by MMP-2/9; C6M: collagen 6 degraded by MMP-2/9; EL-NE: neutrophil-specific elastin fragments; pro-C3: N-terminal propeptide of type III collagen; pro-C6: N-terminal propeptide of type VI collagen.
Effects of nintedanib on circulating biomarkers
In the overall population, there were decreases in KL-6, SP-D, CA-125 and CA19-9 in subjects who received nintedanib versus placebo over 52 weeks (figure 3). The largest decrease was observed for CA-125. Increases in CRP and IL-8 were observed in subjects who received nintedanib versus placebo at week 12 but not at week 52. Small decreases in pro-C6 and s-ICAM were observed in subjects who received nintedanib versus placebo over 52 weeks, starting from week 12 and week 24, respectively. A small decrease in C5M and a small increase in pro-C3 were observed in subjects who received nintedanib versus placebo at weeks 12 and 24, but not at week 52. The effects of nintedanib on KL-6, SP-D, CA19-9, s-ICAM and pro-C6 appeared to be driven by the subjects with a UIP-like pattern on HRCT. The effect of nintedanib on reducing CA-125 was consistent between subgroups by HRCT pattern (figure 3).
*Heat map depicting the effects of nintedanib on changes in biomarkers overall and in subgroups by fibrotic pattern on high-resolution computed tomography (HRCT) in the INBUILD trial. Shading denotes the relative difference versus placebo in change from baseline in the biomarker. : p≤0.05. At baseline, n=252 to n=318 for nintedanib and n=273 to n=312 for placebo in the overall population; n=156 to n=201 for nintedanib and n=174 to n=196 for placebo among subjects with usual interstitial pneumonia (UIP)-like fibrotic pattern on HRCT; n=94 to n=117 for nintedanib and n=105 to n=116 for placebo among subjects with other fibrotic patterns on HRCT. At week 52, n=177 to n=230 for nintedanib and n=182 to n=253 for placebo in the overall population; n=104 to n=142 for nintedanib and n=103 to n=152 for placebo among subjects with UIP-like fibrotic pattern on HRCT; n=65 to n=89 for nintedanib and n=76 to n=101 for placebo among subjects with other fibrotic patterns on HRCT. KL-6: Krebs von den Lungen-6; SP-D: surfactant protein D; CRP: C-reactive protein; IL-8: interleukin-8; s-ICAM: soluble intercellular adhesion molecule; BGM: biglycan degraded by MMP; C1M: collagen 1 degraded by MMP-2/9/13; C3M: collagen 3 degraded by MMP-9; C5M: collagen 5 degraded by MMP-2/9; C6M: collagen 6 degraded by MMP-2/9; EL-NE: neutrophil-specific elastin fragments; pro-C3: N-terminal propeptide of type III collagen; pro-C6: N-terminal propeptide of type VI collagen.
Mediation analyses
Three biomarkers met the criteria for a mediation analysis: CA-125, SP-D and pro-C6 (figure 4). In the mediation analysis of CA-125, the total treatment effect of nintedanib on change in FVC at week 52 was 111.8 mL; of this, a change of 18.3 mL (16.4%) was attributed to the treatment-related decrease in CA-125 at week 12. For SP-D, the total treatment effect of nintedanib on change in FVC at week 52 was 116.7 mL; of this, a change of 5.8 mL (5.0%) was attributed to the treatment-related decrease in SP-D at week 12. For pro-C6, the total treatment effect of nintedanib on change in FVC at week 52 was 108.6 mL; of this, a change of 7.1 mL (6.5%) was attributed to the treatment-related decrease in pro-C6 at week 12. Scatterplots depicting correlations between changes in these biomarkers at weeks 12, 24, 36 and 52 and the rate of decline in FVC over 52 weeks are shown in supplementary figures S3–S5.
Changes in forced vital capacity (FVC) at week 52 attributable to treatment-related changes in CA-125, surfactant protein D (SP-D) and N-terminal propeptide of type VI collagen (pro-C6) at week 12. The orange values denote the indirect effect that the treatment-related change in the biomarker at week 12 has on the change in FVC (mL) at week 52. The red values denote the direct effect of nintedanib on the change in FVC (mL) not mediated by the change in the biomarker. The diamonds indicate the adjusted mean changes in the biomarker and in FVC in the nintedanib and placebo groups.
Discussion
These analyses of data from the INBUILD trial suggest that in subjects with PPF, other than ICAM-1, baseline levels of circulating biomarkers were not associated with the rate of decline in FVC over 52 weeks or other clinically relevant outcomes. Previous studies have suggested that circulating biomarkers such as CA-125, KL-6, MMP-7 and ICAM-1 are associated with ILD progression or mortality in subjects with fibrosing ILDs [14–19]; however, the sensitivity and specificity of these biomarkers appear to be limited [20–22]. To our knowledge, only one previous study of the prognostic potential of circulating biomarkers has been conducted in patients enrolled based on having PPF. In that study, among 77 subjects with PPF defined using the INBUILD trial criteria, elevated KL-6 at baseline, assessed as a continuous variable, was associated with an increased risk of death over 3 years in univariable analyses [23]. The difference in findings of our analysis compared with studies conducted in broader populations of subjects with fibrosing ILDs may reflect the fact that all the patients in the INBUILD trial were enrolled based on having progressive disease. Our current analyses of data from the INBUILD trial are consistent with those from the INMARK trial conducted in subjects with IPF and preserved lung function, in which there were no significant associations between baseline biomarker levels and disease progression over 52 weeks in analyses adjusted for multiple comparisons and the addition of biomarkers to models based on demographic and clinical factors did not improve prediction of disease progression [22].
In these analyses of data from the INBUILD trial, treatment with nintedanib reduced circulating levels of markers of epithelial injury over 52 weeks, with effects observed as early as week 12. The greatest effect of nintedanib was observed on CA-125. The effect of nintedanib on reducing CA-125 was consistent between subgroups by HRCT pattern. A mediation analysis suggested that in the overall population, approximately 16% of the effect of nintedanib on reducing decline in FVC over 52 weeks was attributed to the treatment-related change in CA-125 over 12 weeks. CA-125 is the peptide epitope of MUC16, a membrane-bound mucin that plays a key role in maintaining the epithelium [24]. MUC16 has been shown to be overexpressed in lung tissue of patients with IPF compared with healthy controls and to be localised in fibroblasts from fibrotic foci and proliferative alveolar type II cells [25]. In the PROFILE study, CA-125 was increased throughout the metaplastic epithelium in pulmonary fibrotic lesions from patients with IPF [14]. Elevated levels of CA-125 have been observed in patients with various ILDs compared with people without ILD [26–29]. Consistent with our findings, nintedanib also reduced levels of CA-125 in the INMARK trial in subjects with IPF [30] and in a trial in subjects with ILD associated with systemic sclerosis [31]. In the INMARK trial, a mediation analysis suggested that approximately 40% of the effect of nintedanib on change in FVC over 12 weeks was attributed to the change in CA-125 over 12 weeks [30]. Based on these findings, we believe that CA-125 represents a promising pharmacodynamic biomarker for nintedanib at the population level. However, large variability at the patient level limits the use of CA-125 as a biomarker for individual treatment decisions.
Strengths of our analysis include the use of data from a large, prospective, randomised placebo-controlled trial. Limitations include the need for batch correction for some of the biomarkers. The potential effect of combinations of biomarkers was not studied. Other therapies previously/currently taken by the patients in the study may have introduced confounding effects. Although nintedanib reduced circulating levels of markers of epithelial injury, it is not known whether nintedanib has a direct effect on epithelial dysfunction. The mechanisms by which nintedanib reduces levels of CA-125 are unknown.
In conclusion, data from the INBUILD trial suggest that in subjects with PPF, nintedanib may have an early effect on reducing circulating CA-125 and, to a lesser extent, other markers of epithelial dysfunction. Further studies are required to inform the clinical utility of blood biomarkers in patients with PPF.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Raghu G, Remy-Jardin M, Richeldi L, et al. Idiopathic pulmonary fibrosis (an update) and progressive pulmonary fibrosis in adults: an official ATS/ERS/JRS/ALAT clinical practice guideline. Am J Respir Crit Care Med 2022; 205: e 18–e 47. doi:10.1164/rccm.202202-0399 ST 35486072 PMC 9851481 · doi ↗ · pubmed ↗
- 2Flaherty KR, Wells AU, Cottin V, et al. Nintedanib in progressive fibrosing interstitial lung diseases. N Engl J Med 2019; 381: 1718–1727. doi:10.1056/NEJ Moa 190868131566307 · doi ↗ · pubmed ↗
- 3Maher TM, Corte TJ, Fischer A, et al. Pirfenidone in patients with unclassifiable progressive fibrosing interstitial lung disease: a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet Respir Med 2020; 8: 147–157. doi:10.1016/S 2213-2600(19)30341-831578169 · doi ↗ · pubmed ↗
- 4Behr J, Prasse A, Kreuter M, et al. Pirfenidone in patients with progressive fibrotic interstitial lung diseases other than idiopathic pulmonary fibrosis (RELIEF): a double-blind, randomised, placebo-controlled, phase 2b trial. Lancet Respir Med 2021; 9: 476–486. doi:10.1016/S 2213-2600(20)30554-333798455 · doi ↗ · pubmed ↗
- 5Hambly N, Farooqi MM, Dvorkin-Gheva A, et al. Prevalence and characteristics of progressive fibrosing interstitial lung disease in a prospective registry. Eur Respir J 2022; 60: 2102571. doi:10.1183/13993003.02571-202135273032 · doi ↗ · pubmed ↗
- 6Khor YH, Farooqi M, Hambly N, et al. Patient characteristics and survival for progressive pulmonary fibrosis using different definitions. Am J Respir Crit Care Med 2023; 207: 102–105. doi:10.1164/rccm.202205-0910 LE 35943331 PMC 9952865 · doi ↗ · pubmed ↗
- 7Selman M, Pardo A. When things go wrong: exploring possible mechanisms driving the progressive fibrosis phenotype in interstitial lung diseases. Eur Respir J 2021; 58: 2004507. doi:10.1183/13993003.04507-202033542060 · doi ↗ · pubmed ↗
- 8Wollin L, Distler JHW, Redente EF, et al. Potential of nintedanib in treatment of progressive fibrosing interstitial lung diseases. Eur Respir J 2019; 54: 1900161. doi:10.1183/13993003.00161-201931285305 PMC 6751387 · doi ↗ · pubmed ↗