Pain After Brachial Plexus Injury Surgery: Variability in Reporting
Anna Zakusylo, Aryan Borole, Evan Lobato, Andrew G Baddoo, Diana Vitkovska, Daniel Devine, Jomar N Aryee, Ajul Shah, Brian M Katt

TL;DR
This paper highlights the lack of standardized pain reporting after brachial plexus injury surgery, making it hard to compare outcomes across studies.
Contribution
The study identifies significant variability in postoperative pain reporting methods and timepoints in BPI surgery research.
Findings
Nine studies showed more than 15 different postoperative timepoints for pain assessment.
Only a few studies reported pain at comparable intervals, preventing pooled analysis.
Pain was common after BPI, especially in root avulsion cases, with some surgical techniques showing qualitative improvement.
Abstract
Pain is a major contributor to morbidity following brachial plexus injury (BPI), yet pain-related outcomes are inconsistently reported. The extent of postoperative pain improvement after surgical reconstruction remains unclear due to variable measurement techniques and nonstandardized reporting intervals. A systematic review was conducted in accordance with the PRISMA guidelines. Studies involving adults undergoing operative treatment for traumatic BPI that reported pain using the Visual Analog Scale (VAS) were included. Data extraction focused on the timing and methods of postoperative pain assessment. Nine studies met the inclusion criteria. Pain reporting demonstrated substantial heterogeneity, with more than 15 different postoperative timepoints reported across studies. Only a small minority of studies reported pain at comparable intervals, precluding pooled analysis. Pain was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
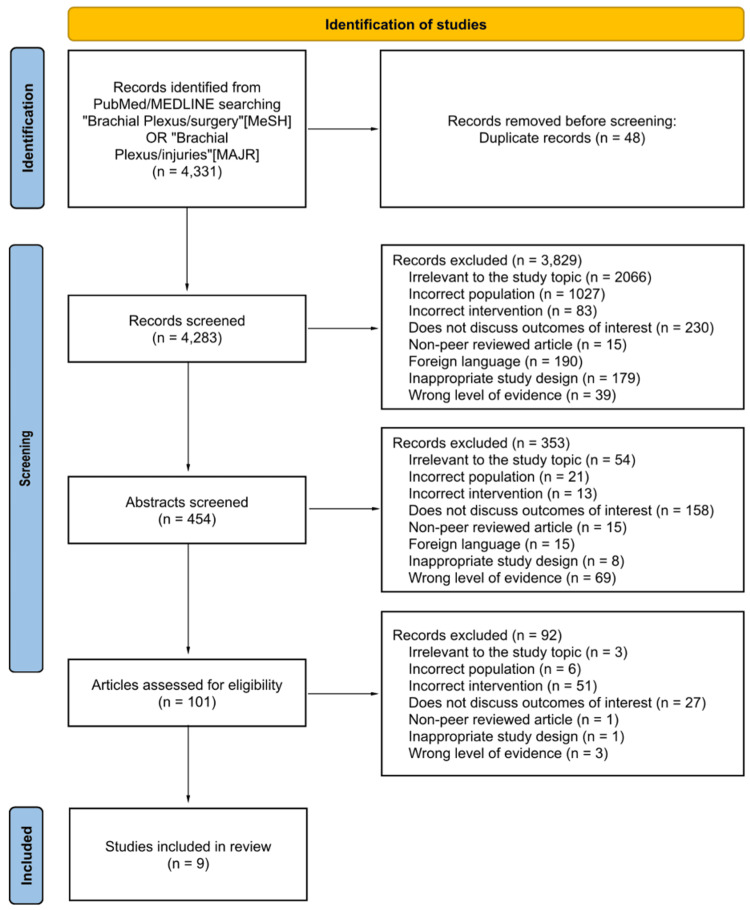 Figure 1
Figure 1| Author (year) | Injury type | Operation | When VAS scores were collected | Pre-op VAS scores | Post-op VAS scores | Sample size |
| Htut et al. (2006) [ | Avulsion | Brachial plexus repair with graft and nerve transfer | Mean time of assessment: 4 years after assessment | Not possible to assess most patients prior to surgery, as many were referred early after injury and surgical repairs were performed urgently | 2.7 | 54 |
| Avulsion | Reimplantation of avulsed nerve roots | 4 | 14 | |||
| Avulsion | No repair at all: late referral | 4.8 | 8 | |||
| Kato et al. (2006) [ | Avulsion | Brachial plexus repair with graft and nerve transfer (patients grouped based on timing from injury to surgery) | Pre-op scores and time of final VAS assessments not stated | Not stated | Group 1 (<1 m), 2.6; Group 2 (1-3 m), 3.7; Group 3 (3-6 m), 4.0; Group 4 (>6 m), 5.3 | 148 |
| Armas-salazar et al. (2022) [ | Injury | Neurolysis (5 roots) | Before surgery and last follow-up (61.9 ± 53.6 months) | 8 | 2.6 | 3 |
| Neurolysis (3 roots) | 8.25 | 5 | 4 | |||
| Neurolysis (2 roots) | 9 | 2 | 3 | |||
| Gebreyohanes et al. (2023) [ | Avulsion | Dorsal root entry zone (DREZ) | Median follow-up 37 months | 9.1 | 3.5 | 10 |
| Maldonado et al. (2023) [ | Injury | Gracilis muscle transfer | Mean follow-up of 37 months | 5.3 | 4.5 | 27 |
| Dukan et al. (2023) [ | Avulsion | Nerve transfer | Pre-op not stated; post-op time at the last follow-up not stated, but inclusion criteria required at least 10 years from surgery | Not stated | 3.2 | 16 |
| Emamhadi et al. (2017) [ | Avulsion | Nerve transfer | Pain before surgery was compared to that at the six-month follow-up | 8.5 | 0.7 | 11 |
| Baruah et al. (2024) [ | Avulsion | DREZotomy | Preop and post-op VAS scores | 7.3 | 3.8 | 18 |
| Dong et al. (2012) [ | Avulsion | DREZ lesioning | Pre-op and 12 months post-op | 8.9 | 0.9 | 7 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNerve Injury and Rehabilitation · Anesthesia and Pain Management · Pain Management and Treatment
Introduction and background
Traumatic brachial plexus injuries (BPIs) cause devastating motor and sensory deficits in a young, active population. The incidence of BPI has increased with the rise of high-energy trauma. Epidemiological data suggest a growing incidence of BPIs, estimated at 1.6 per 100,000 persons annually in the United States. BPIs are particularly prevalent in urban areas due to the high risk of BPI associated with motorcycle crashes [1]. Although reconstructive strategies have improved motor outcomes, such as elbow flexion and shoulder stability, neuropathic pain remains one of the most disabling consequences of BPI.
Neuropathic pain after BPI arises from peripheral and central mechanisms. Root avulsion injuries, in particular, generate severe deafferentation pain with potential central sensitization. This persistent pain impairs sleep, psychological well-being, functional recovery, and rehabilitation engagement [2]. Yet despite its clinical importance, pain remains underreported in the BPI literature. Several authors have noted that pain outcomes are inconsistently reported in the brachial plexus literature, with most studies emphasizing motor recovery while underrepresenting pain-specific measures [3].
Pain trajectories after surgery are poorly defined. Some studies demonstrate substantial pain improvement with nerve reconstruction or microsurgical dorsal root entry zone (DREZ) lesioning, whereas others report persistent or worsening pain, particularly in complete avulsion injuries [4-8]. The inconsistent measurement of postoperative pain has resulted in a fragmented body of evidence, limiting the ability to counsel patients reliably.
This systematic review was designed to synthesize postoperative pain outcomes following operative treatment of BPI. However, during data extraction, it became clear that the literature is too heterogeneous to support quantitative comparison. Instead, this review describes the variability in pain reporting and highlights the need for standardized reporting guidelines.
Review
Methods
Search Strategy
A systematic search was performed across PubMed, Embase, and the Cochrane Library following the PRISMA guidelines using keywords related to BPI, surgery, and pain outcomes.
Studies that met the following inclusion criteria were included for review: adult patients (≥18 years), patients who underwent operative treatment for traumatic BPIs, pain outcomes reported using the Visual Analog Scale (VAS), and peer-reviewed articles with extractable data. Studies were excluded from our review if they involved patients treated nonoperatively, included pediatric cohorts, lacked validated pain outcome measurement tools, or lacked extractable postoperative pain data.
Data Extraction and Synthesis
Extracted data included injury pattern, surgical technique, pain scale used, and postoperative timepoints. Because of substantial heterogeneity, a pooled meta-analysis was not performed. A descriptive synthesis was produced (Figure 1).
PRISMA flow diagram of the study selection process
Results
Nine studies met the inclusion criteria (Table 1). These papers represented a wide range of operative treatments for traumatic BPIs, including nerve transfers, nerve grafts, vascularized nerve grafts, free muscle transfers, and dorsal root entry zone (DREZ) procedures. Study sizes varied from small single-surgeon experiences to larger series of more than 100 patients. The follow-up ranged from several months to multiple years.
Pain reporting was inconsistent across the literature. Investigators measured pain at more than 15 different postoperative intervals. Some included very early postoperative scores, others reported short- or mid-range follow-up at three or six months, and many provided only a single final follow-up value. The timing of this final measurement ranged widely, from less than six months to more than five years after surgery. Only a small number of studies reported pain at comparable timepoints, and even those differed in scale or reporting format.
The structure of pain reporting also varied. Some authors provided mean values with standard deviation. Others reported medians or ranges. Several studies included pain only in figures or narrative descriptions without extractable numerical data. A number of papers listed preoperative and postoperative values but failed to specify when the postoperative measurement was collected. Because of these inconsistencies, the pain data could not be combined or analyzed quantitatively.
Even with the heterogeneity, several broad descriptive trends were visible. Pain after BPI was common across nearly all cohorts. Many patients continued to report burning, aching, or neuropathic symptoms after surgery. Studies that stratified by injury pattern consistently found that more severe injuries, particularly root avulsions, exhibited higher preoperative pain and more persistent symptoms after reconstruction. Many reports also described some degree of postoperative improvement in pain, but the variation in measurement methods and follow-up intervals prevented comparison of the magnitude or timing of that improvement.
Overall, pain outcomes across these studies show consistent evidence of postoperative symptoms but substantial inconsistency in how results are measured and reported. These descriptive findings set the stage for interpreting the underlying trends observed in the wider literature.
Discussion
The primary finding of this review is that pain reporting after brachial plexus surgery is profoundly inconsistent. Although pain is a major determinant of disability and overall quality of life, the literature does not use a uniform approach to measuring or reporting pain outcomes. In our review, we found an additional 35 studies that utilized standardized instruments, such as Disabilities of the Arm, Shoulder and Hand (DASH) and Numerical Rating Scale (NRS); however, the sample sizes were significantly smaller compared to those using VAS, with widely variable collection timepoints, making comparison unfeasible. Because of this substantial heterogeneity in both measurement tools and follow-up timepoints, these studies were excluded from our analysis entirely. The heterogeneity making study comparison difficult also makes it challenging to counsel patients with confidence about expected postoperative pain trajectories.
Multiple studies highlight the heavy pain burden faced by patients with root avulsion injuries. Bertelli et al. reported that 64% of individuals with avulsion injuries experienced substantial preoperative pain, and many continued to report persistent symptoms after surgery [16].
Surgical technique also appears to influence postoperative pain. Authors have reported improvements with neurotization. DREZ procedures have shown consistent benefit for refractory neuropathic pain. Chen et al. reported a decrease in VAS scores from >9 preoperatively to just >3 at final follow-up among patients with long-standing avulsion pain [17]. Vascularized ulnar nerve grafts produced improvements in pain and disability scores in the cohort reported by Lin et al. [18]. Combined contralateral C7 transfer with free functioning muscle transfer also produced symptomatic improvement, with moderate or mild relief noted in the majority of treated patients [19]. Although the degree of improvement cannot be compared across studies because of inconsistent timing and inconsistent scoring methods, the overall direction of improvement was similar.
Pain trajectories varied widely across the included studies. Some authors noted early improvement shortly after surgery, while others described more gradual reduction in symptoms that appeared only when patients began to demonstrate reinnervation or functional return. Several investigations commented that patients who recovered useful motion tended to experience greater pain improvement than those who did not. Although this relationship cannot be quantified based on available data, it suggests that motor recovery and pain reduction may follow similar paths in a subset of patients.
Despite broad agreement that pain is important, this review highlights the remarkably inconsistent ways in which pain outcomes are recorded in the literature. Investigators used different scales, different intervals, and different reporting formats. Some provided clear preoperative and postoperative values, others reported single timepoints without context, and many used graphical formats without extractable numbers. This limits the ability to identify typical pain patterns or compare the effectiveness of different surgical techniques. Future work will need to adopt more uniform pain reporting methods to better understand recovery trajectories and guide clinical expectations.
Conclusions
Pain is a major and persistent consequence of BPI, but postoperative pain outcomes are reported with substantial inconsistency across the literature. Because few studies use standardized scales at comparable timepoints, meaningful pooled analysis is not possible. Standardized pain reporting is urgently needed to improve the ability to compare outcomes, guide treatment decisions, and provide more reliable expectations for patients undergoing reconstruction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of brachial plexus injuries in a multitrauma population Neurosurgery Midha R 11821189401997917989110.1097/00006123-199706000-00014 · doi ↗ · pubmed ↗
- 2Daily life impact of brachial plexus reconstruction in adults: 10 years follow-up J Hand Surg Am Dukan R Gerosa T Masmejean EH 116748202310.1016/j.jhsa.2022.03.02235641388 · doi ↗ · pubmed ↗
- 3Outcomes of surgery in 1019 brachial plexus lesions treated at Louisiana State University Health Sciences Center J Neurosurg Kim DH Cho YJ Tiel RL Kline DG 100510169820031274436010.3171/jns.2003.98.5.1005 · doi ↗ · pubmed ↗
- 4Pain after avulsion injuries and complete palsy of the brachial plexus. The possible role of nonavulsed roots in pain generation Neurosurgery Bertelli JA Ghizoni MF 110411146220081858080810.1227/01.neu.0000325872.37258.12 · doi ↗ · pubmed ↗
- 5Pain phenomena and sensory recovery following brachial plexus avulsion injury and surgical repairs J Hand Surg Br Htut M Misra P Anand P Birch R Carlstedt T 5966053120061682259810.1016/j.jhsb.2006.04.027 · doi ↗ · pubmed ↗
- 6Microsurgical lesioning in the dorsal root entry zone for pain due to brachial plexus avulsion: a prospective series of 55 patients J Neurosurg Sindou MP Blondet E Emery E Mertens P 1018102810220051602876010.3171/jns.2005.102.6.1018 · doi ↗ · pubmed ↗
- 7Factors affecting long-term outcome in dorsal root entry zone lesioning for brachial plexus avulsion Pain Du T Ji F Ni B 97798316420233615653010.1097/j.pain.0000000000002788 PMC 10108586 · doi ↗ · pubmed ↗
- 8Microscissor DRE Zotomy for post brachial plexus avulsion neuralgia: a single center experience Clin Neurol Neurosurg Doddamani RS Garg S Agrawal D 10684020820213441870610.1016/j.clineuro.2021.106840 · doi ↗ · pubmed ↗