Mesenchymal Tumor of the Hand Causing Tumor-Induced Osteomalacia
Andrew Cecil, Meti Shagi, Syed Basit Haider, Syed Ali A Gardezi

TL;DR
A rare hand tumor caused bone weakness and low phosphate levels, but was successfully treated with surgery after a long diagnostic journey.
Contribution
This case highlights the diagnostic challenges and successful treatment of a phosphaturic mesenchymal tumor in an unusual hand location.
Findings
A 55-year-old male with TIO had a mesenchymal tumor in the hand confirmed by imaging and surgery.
Post-surgery normalization of serum phosphorus confirmed biochemical cure.
Expert imaging interpretation was crucial for identifying the tumor after initial scans were non-localizing.
Abstract
Tumor-induced osteomalacia (TIO) is an ultra-rare paraneoplastic syndrome caused by excessive secretion of fibroblast growth factor 23 (FGF23) from phosphaturic mesenchymal tumors, leading to renal phosphate wasting, hypophosphatemia, and osteomalacia. Diagnosis is frequently delayed due to nonspecific symptoms and the difficulty of localizing small, often indolent tumors. We report a 55-year-old male patient who presented with a 16-month history of progressive muscle weakness, chronic bone pain, and multiple bilateral metatarsal fractures. Laboratory evaluation demonstrated profound hypophosphatemia (1.6 mg/dL), markedly elevated FGF23 levels (455 RU/mL), and renal phosphate wasting (tubular reabsorption of phosphate at 35%, tubular maximum phosphate reabsorption per glomerular filtration rate (TmP/GFR) at 1.04 mg/dL). Initial fluorodeoxyglucose positron emission tomography/computed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
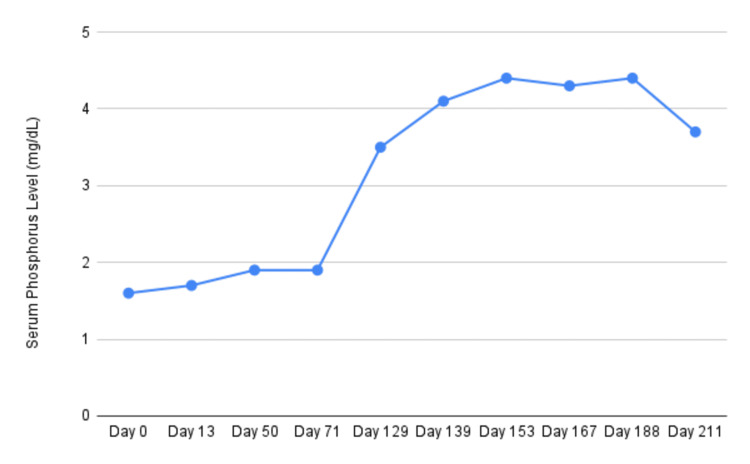 Figure 1
Figure 1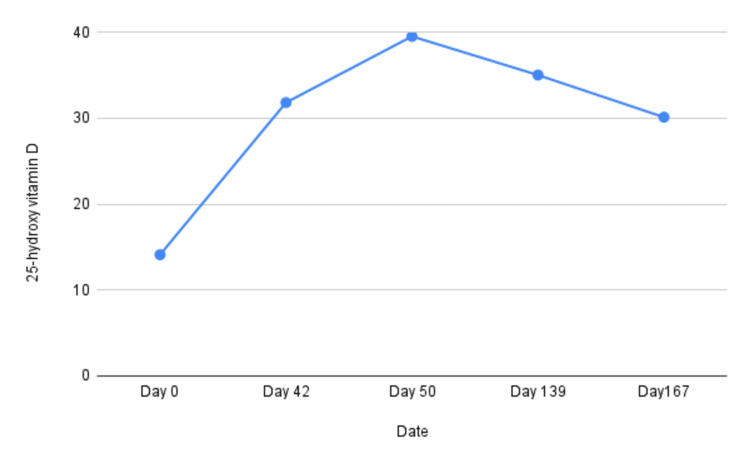 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4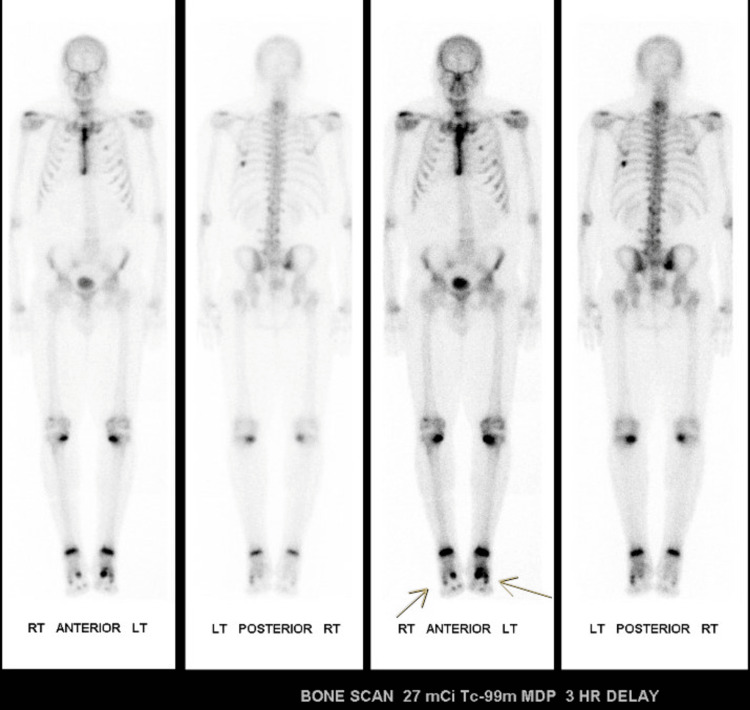 Figure 5
Figure 5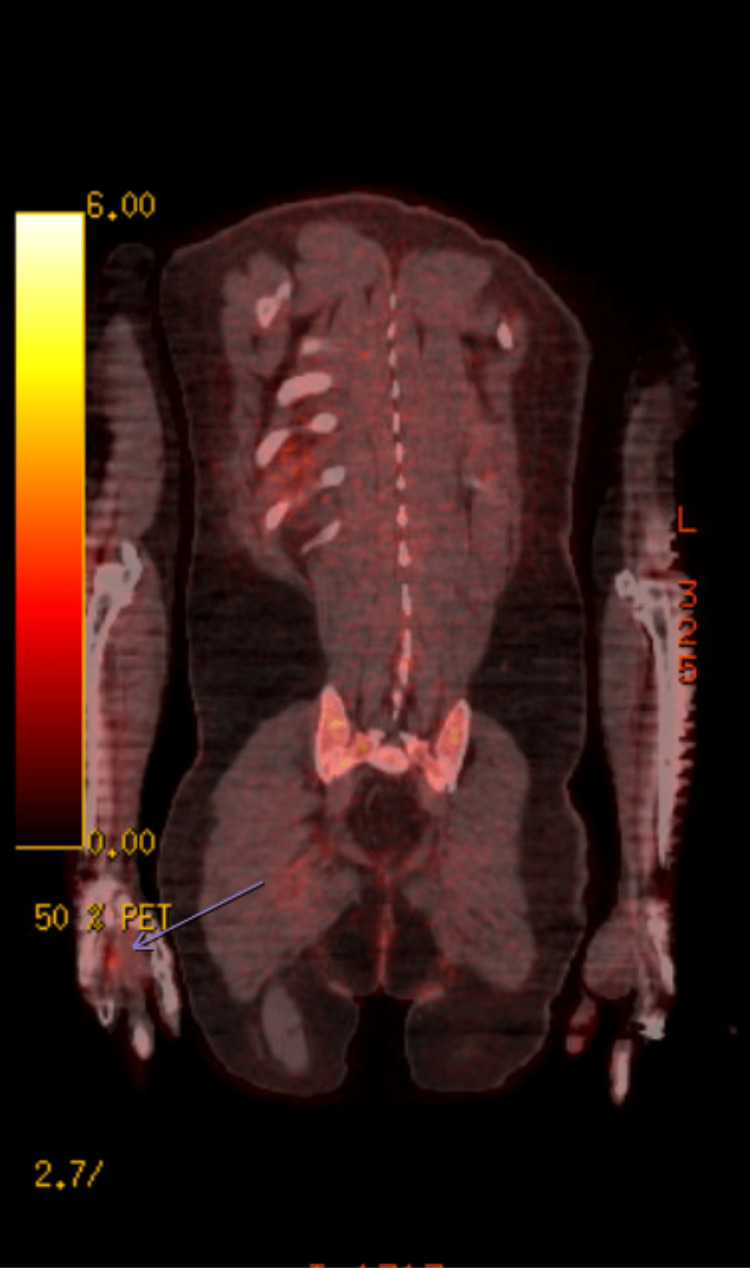 Figure 6
Figure 6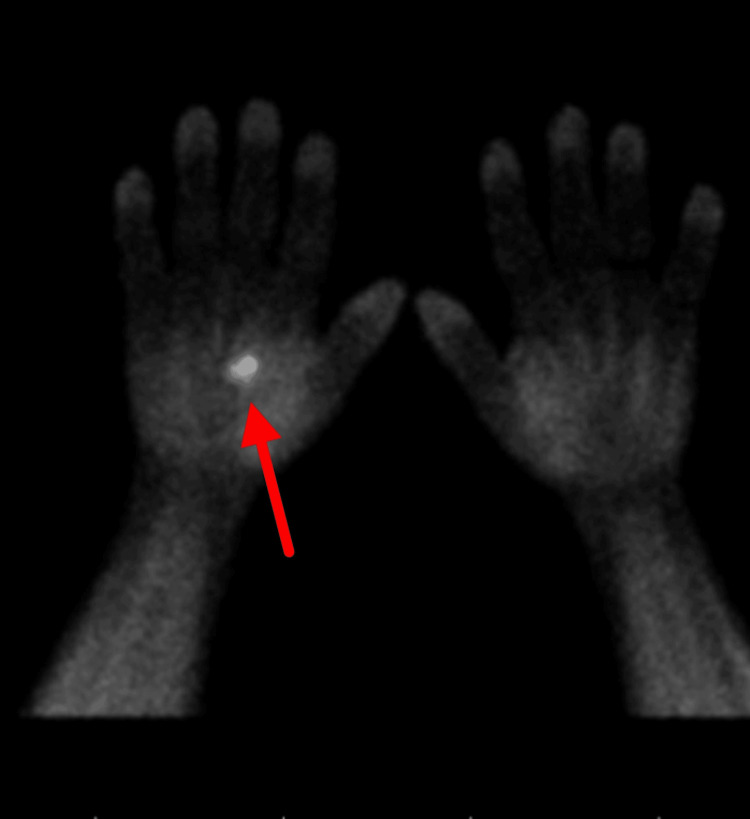 Figure 7
Figure 7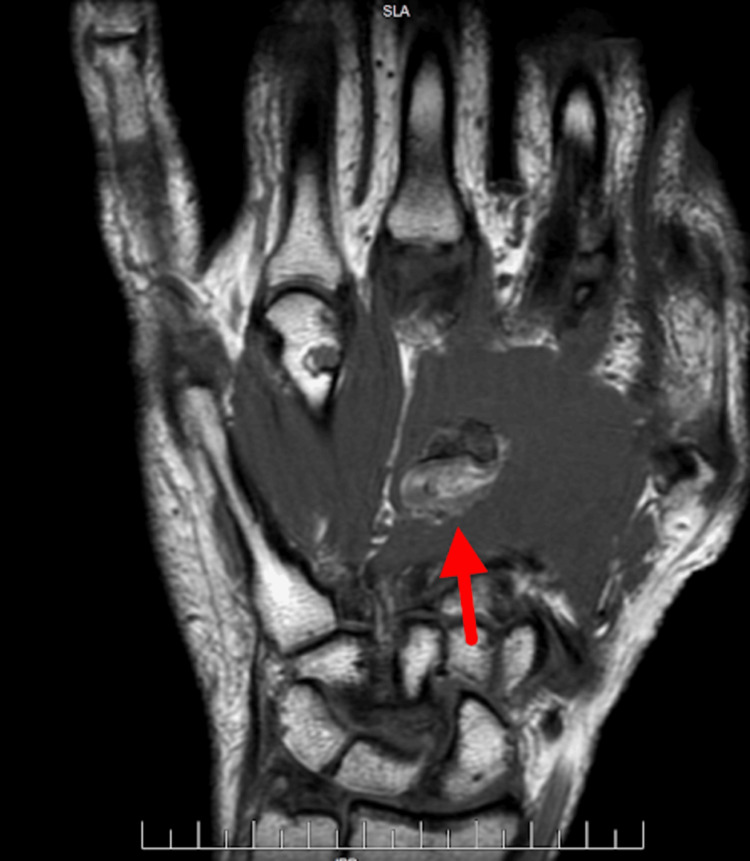 Figure 8
Figure 8| Laboratory tests | Result | Reference range |
| Serum phosphorus (mg/dL) | 1.6 | 2.4–4.7 |
| Alkaline phosphatase (U/L) | 161 | 45–117 |
| 24-hour urine phosphorus (g/24hr) | 1.4 | 0.4-1.3 |
| TmP/GFR (mg/dL) | 1.04 | 2.8-4.4 |
| Vitamin D (ng/mL) | 14.1 | 30-100 |
| Parathyroid hormone (pg/mL) | 66 | 14-72 |
| Fibroblast growth factor 23 (RU/mL) | 455 | 44-215 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Sarcoma Diagnosis and Treatment · Heterotopic Ossification and Related Conditions
Introduction
Tumor-induced osteomalacia (TIO) is an ultra-rare paraneoplastic disorder caused by excessive secretion of fibroblast growth factor 23 (FGF23), usually from small, slow-growing mesenchymal tumors, leading to hypophosphatemia and defective bone mineralization [1,2]. Patients often present with nonspecific symptoms such as bone pain, muscle weakness, and fractures, resulting in frequent misdiagnosis and prolonged delays to diagnosis [3].
FGF23 disrupts phosphate homeostasis by reducing renal phosphate reabsorption and suppressing conversion of 25-hydroxyvitamin D to its active form, 1,25-dihydroxyvitamin D. This leads to persistent hypophosphatemia, low or inappropriately normal calcitriol, and impaired bone mineralization [1,2]. Laboratory findings typically include low serum phosphate, elevated or inappropriately normal FGF23, low-to-normal 1,25-dihydroxyvitamin D, and elevated alkaline phosphatase [3].
Phosphaturic mesenchymal tumors are usually small (median 2.7-3.0 cm) and can arise in soft tissue or bone, with the lower extremities and pelvis being most common [4]. Due to this, tumor localization is challenging and requires a systematic approach, beginning with functional imaging, preferably somatostatin receptor positron emission tomography/computed tomography (PET/CT), which offers higher sensitivity than fluorodeoxyglucose-PET (FDG-PET) or octreotide scans [5,6]. Once identified, surgical excision with wide margins is curative in most cases [4]. For patients with unresectable or non-localized tumors, medical therapy with phosphate, active vitamin D, or the anti-FGF23 antibody burosumab provides successful disease management [7-9].
Case presentation
A 55-year-old male patient with a history of hypertension, hyperlipidemia, reactive airway disease, and mitral valve prolapse status post mitral valve repair, presented to the endocrinology clinic with multiple recent bilateral metatarsal fractures and 16 months of progressive muscle weakness. His ambulation was significantly limited, necessitating cessation of work as an electrician due to pain.
The patient reported persistent sternal pain since undergoing open-heart surgery in 2013, as well as chronic metatarsal bone pain. Additional pain involved the hips, knees, and ribs. He had a history of military deployment to Afghanistan, during which he remained physically active without notable trauma or fractures. He also noted an increase in shoe size from 11.5 to 13. There was no significant family history of endocrine disorders or fractures.
On examination, he demonstrated a markedly slow gait and required a cane for ambulation. Vital signs were stable: blood pressure 106/78 mmHg, heart rate 84 bpm, respiratory rate 18/min. Laboratory evaluation revealed hypophosphatemia (serum phosphate 1.6 mg/dL; reference range: 2.4-4.7 mg/dL), elevated alkaline phosphatase (161 U/L; reference range: 45-117 U/L), and 25-OH vitamin D (14.1 ng/mL; reference range: 30-100 ng/mL). His 24-hour urine phosphate was 1.4 g (reference range: 0.4-1.3 g/24 h), tubular reabsorption of phosphate (TRP) was 35% (reference range: 85-95%), and tubular maximum phosphate corrected for glomerular filtration rate (TmP/GFR) was 1.04 mg/dL (reference range: 2.8-4.4 mg/dL), consistent with renal phosphate wasting (Figures 1, 2).
Serum phosphate level over disease course and after tumor resection (9/15/2014)
Serum 25-hydroxy vitamin D levels
FGF23 was markedly elevated at 455 RU/mL (Table 1).
Other laboratory studies, including serum and urine protein electrophoresis, testosterone, insulin-like growth factor-1, and intact parathyroid hormone, were within normal limits. The patient was initiated on vitamin D supplementation (4000 units daily) and oral potassium phosphate therapy (1 gram three times daily).
Radiographs of the feet showed healing bilateral fourth metatarsal fractures with diffuse osteopenia (Figures 3, 4).
Radiograph of the left footDemonstrates healing of a proximal diaphyseal fracture of the fourth metatarsal with interval healing, along with inferior and posterior calcaneal spurring, and generalized osteopenia.
Radiograph of the right footDemonstrates healing proximal diaphyseal fracture at the fourth metatarsal and presence of inferior calcaneal spurring with generalized osteopenia.
Bone scan revealed mild increased uptake at the base of the first metatarsal, moderate uptake in the distal tibias, and marked uptake in the sternum, left ribs, and feet (Figure 5).
Bone scanDemonstrates increased uptake in the left first metatarsal, distal tibias bilateral, bilateral medial tibias and multiple less intense radiotracer uptake within the feet. Increased uptake in the sternum and ribs is consistent with recent open heart surgery.
Initial PET/CT did not identify abnormal FDG uptake concerning for malignancy and was considered non-localizing. A re-interpretation of imaging identified faint focal FDG uptake in the right third metacarpal (Figure 6).
Faint focal FDG activity within the right third metacarpal visualized on the reinterpretation of PET/CTFDG: fluorodeoxyglucose; PET/CT: positron emission tomography/computed tomography.
Technetium-99m sestamibi scanning confirmed tracer uptake in the right palm (Figure 7).
Increased radiotracer uptake noted in the right palm on the sestamibi scan
MRI demonstrated a 1.9 × 1.8 × 1.2 cm heterogeneously enhancing ovoid soft-tissue mass within the palmar tissues, centered over the proximal shaft of the third metacarpal and extending into the interspace between the second and third metacarpals, consistent with a phosphaturic mesenchymal tumor (Figure 8).
MRI imagingDemonstrates a 1.9 × 1.8 × 1.2 cm heterogeneously enhancing ovoid soft-tissue mass within the palmar tissues, centered over the proximal shaft of the third metacarpal and extending into the interspace between the second and the third metacarpals.
The patient underwent surgical excision of the mass. Histopathology confirmed a phosphaturic mesenchymal tumor with positive FGF23 mRNA on in situ hybridization. Postoperatively, serum phosphorus normalized within two months of the procedure.
Discussion
This case emphasizes the diagnostic challenges of TIO, including its nonspecific symptoms and the difficulty in localizing the tumor. Notably, the patient experienced 16 months of progressive weakness, fractures, and chronic bone pain. These symptoms are consistent with the insidious course reported in the literature, where diagnosis can be delayed over several years [3].
Laboratory findings, including marked hypophosphatemia, elevated FGF23, and renal phosphate wasting, were diagnostic in this context. These values are consistent with reported series, confirming that biochemical evaluation is critical for identifying TIO [1,3].
Tumor localization proved challenging in this patient, as initial FDG-PET/CT was non-diagnostic. However, a specialized review ultimately demonstrated faint uptake in the right third metacarpal, which was confirmed by sestamibi scintigraphy and MRI. This sequence underscores the critical role of expert interpretation and stepwise functional imaging, particularly using somatostatin receptor-based PET/CT, for accurate localization and surgical planning [5,6]. Of note, this case predates the 2023 Global Guidance for TIO, which now recommends somatostatin receptor-based PET/CT (e.g., 68Ga-DOTATATE) as first-line functional imaging due to its superior sensitivity over FDG-PET/CT [2,10,11].
Histopathology confirmed a phosphaturic mesenchymal tumor with positive FGF23 in situ hybridization, a highly sensitive and specific diagnostic method [12]. Postoperative normalization of serum phosphate demonstrated cure, consistent with the rapid biochemical response expected following complete excision [13-17].
Key clinical lessons from this case include the need to consider TIO in any patient with unexplained hypophosphatemia, bone pain, and fractures, and the utility of early, systematic imaging to localize the tumor. Complete surgical resection remains essential to prevent recurrence, while patients with unresectable or non-localized disease benefit from phosphate, vitamin D, or burosumab therapy. This case highlights that multidisciplinary care optimizes outcomes in this rare but treatable condition [1,3,5,6,8,10,18].
Conclusions
This case highlights the diagnostic and therapeutic challenges of TIO and demonstrates the excellent outcomes achievable with complete surgical resection. Prolonged nonspecific musculoskeletal symptoms in the setting of hypophosphatemia and elevated FGF23 levels should raise clinical suspicion for TIO. Accurate tumor localization is critical and often requires advanced functional imaging interpreted at specialized centers.
Surgical excision with wide margins remains the definitive treatment, typically resulting in rapid normalization of serum phosphorus and symptomatic improvement. In patients with unresectable or non-localizing tumors, medical therapy with phosphate, active vitamin D, or burosumab offers effective disease control by targeting FGF23 excess. Early recognition, systematic diagnostic evaluation, and multidisciplinary management are essential to optimize outcomes in this rare but treatable condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tumor-induced osteomalacia: a comprehensive review Endocr Rev Minisola S Fukumoto S Xia W 3233534420233632729510.1210/endrev/bnac 026 · doi ↗ · pubmed ↗
- 2Global guidance for the recognition, diagnosis, and management of tumor-induced osteomalacia J Intern Med Jan de Beur SM Minisola S Xia WB 30932829320233651165310.1111/joim.13593 PMC 10108006 · doi ↗ · pubmed ↗
- 3Tumor-induced osteomalacia: a systematic clinical review of 895 cases Calcif Tissue Int Bosman A Palermo A Vanderhulst J 36737911120223585706110.1007/s 00223-022-01005-8PMC 9474374 · doi ↗ · pubmed ↗
- 4Postoperative outcome and clinical management of tumor-induced osteomalacia: a single-center retrospective cohort study on 117 patients Osteoporos Int Shan C Wei Z Li S 191919303620254049324110.1007/s 00198-025-07527-9PMC 12612011 · doi ↗ · pubmed ↗
- 5Performance of 68Ga-DOTA-SST PET/CT, octreoscan SPECT/CT and 18F-FDG PET/CT in the detection of culprit tumors causing osteomalacia: a meta-analysis Nucl Med Commun Jiang Y Hou G Cheng W 3703764120203200017310.1097/MNM.0000000000001163 PMC 7077972 · doi ↗ · pubmed ↗
- 6Diagnostic utility of Ga-68 DOTA-SSTR and F-18 FDG PET/CT in the detection of culprit tumours causing osteomalacia: a systematic review and meta-analysis Nucl Med Commun Agrawal K Padhy BM Meher BR Mohanty RR 6466554220213362518710.1097/MNM.0000000000001379 · doi ↗ · pubmed ↗
- 7Burosumab: current status and future prospects Best Pract Res Clin Endocrinol Metab Goyal A Tandon N 1018263820243785847910.1016/j.beem.2023.101826 · doi ↗ · pubmed ↗
- 8Interim analysis of a phase 2 open-label trial assessing burosumab efficacy and safety in patients with tumor-induced osteomalacia J Bone Miner Res Imanishi Y Ito N Rhee Y 2622703620213296704610.1002/jbmr.4184 PMC 7988547 · doi ↗ · pubmed ↗