Beyond the Apex: A Case Series of Mid-ventricular Takotsubo Cardiomyopathy
Fnu Parul, Karuna Rayamajhi, Rohan Kumar, Akhil Gaderaju, Mahmoud Khairy, Appa Bandi

TL;DR
This paper presents two cases of mid-ventricular Takotsubo cardiomyopathy triggered by physical stressors, emphasizing the importance of recognizing atypical presentations for timely diagnosis and treatment.
Contribution
The novelty lies in highlighting mid-ventricular TCM as an atypical variant and showcasing its clinical presentation and management in real-world cases.
Findings
Mid-ventricular TCM can present with acute cardiac dysfunction and mimic acute coronary syndromes.
Prompt diagnosis and treatment with beta-blockers and ARBs led to full recovery in both cases.
Recognition of atypical TCM variants is crucial for preventing misdiagnosis and recurrence.
Abstract
Takotsubo cardiomyopathy (TCM), also known as stress-induced cardiomyopathy, is characterized by transient, reversible left ventricular systolic dysfunction in the absence of obstructive coronary artery disease (CAD). It can mimic acute coronary syndromes, posing diagnostic challenges that require a high index of suspicion. We present two cases of mid-ventricular TCM, each triggered by distinct acute physical stressors. The first case involves a 63-year-old male with a history of cerebrovascular accident and nicotine dependence who presented following a generalized tonic-clonic seizure. His electrocardiogram demonstrated ST-segment elevations in the inferolateral leads, and laboratory workup revealed elevated cardiac biomarkers. Coronary angiography showed mild non-obstructive CAD, while echocardiography revealed mid-ventricular regional wall motion abnormalities with an ejection…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
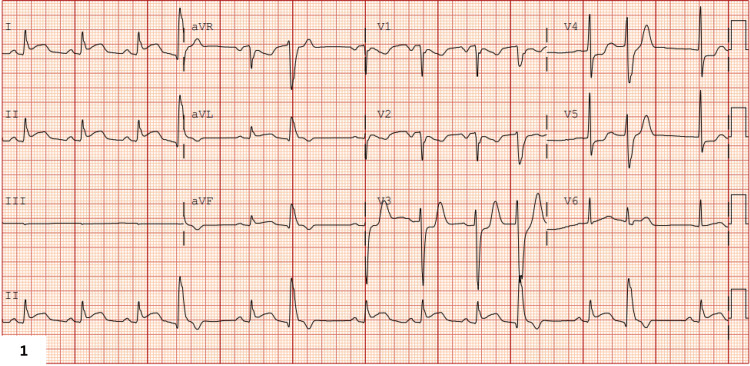 Figure 1
Figure 1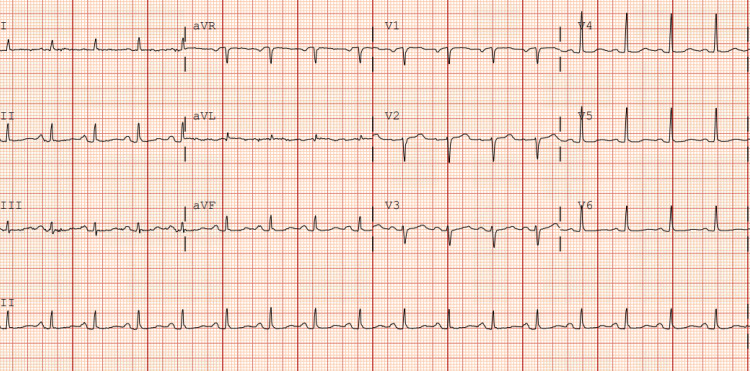 Figure 2
Figure 2| Variables | Value | Reference Range |
| Lactate | 13.3 mmol/L | 0.2-1.8 mmol/L |
| Ammonia | 124 µmol/L | 13-37 umol/L |
| High-sensitivity troponin I | 34->7334->8522 ->5334 ->3005 ng/L | 0-18 ng/L |
| CPK (creatine phosphokinase) | 726U/L | 0-200 U/L |
| Variables | Value | Reference Range |
| Arterial blood pH | 7.29 | 7.35-7.45 |
| White blood cells | 23,900 /µL | 4.0-12.0 10*3/uL |
| High-sensitivity troponin I | 74 -> 382 ->610 ->717 ->457 ng/L | 0-18 ng/L |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTakotsubo Cardiomyopathy and Associated Phenomena · Pericarditis and Cardiac Tamponade · Pathogenesis and Treatment of Hiccups
Introduction
Takotsubo cardiomyopathy (TCM), also known as stress-induced cardiomyopathy, is characterized by a temporary and reversible regional left ventricular systolic dysfunction that mimics an acute coronary event, despite the absence of obstructive coronary artery disease (CAD) [1]. It represents approximately 2% of cases within the ST-elevation myocardial infarction (STEMI) population and predominantly affects postmenopausal women, who account for about 90% of all cases [2]. This condition is typically triggered by sudden, severe emotional or physical stress, which leads to excessive catecholamine release, resulting in microvascular dysfunction and intracellular calcium overload [3].
Clinically, TCM often presents with akinesis or hypokinesis of the apical segment of the left ventricle, commonly with hyperkinetic basal segments. However, atypical variants involving regional wall motion abnormalities have been reported, including basal, focal, mid-ventricular, biventricular (involving both the apical and right ventricle), isolated right ventricular, and even global variants [4]. Although apical form remains the most common, the diagnosis of midventricular variant has increased from 18% to 28% from 2004 to 2021 [5]. Recognition of the mid-ventricular subtype of Takotsubo syndrome is clinically important, as this form may be associated with additional complications, including dynamic left ventricular outflow tract (LVOT) obstruction, alongside an increased risk of hemodynamic compromise and cardiogenic shock. Furthermore, compared with the classic apical variant, the mid-ventricular subtype may exhibit more subtle and evolving electrocardiographic changes, which can delay or complicate diagnosis, as previously reported in the literature [6].
Case presentation
Case 1
A 63-year-old male with a medical history of cerebrovascular accident and nicotine dependence presented to the emergency department in a post-ictal, confused state following a generalized tonic-clonic seizure. On admission, the cardiopulmonary examination revealed normal heart sounds and mild bibasilar crackles. His vital signs were within normal limits (heart rate (HR) of 80-90 bpm, blood pressure (BP) of 128/64 mmHg, and SpO_2_ of 94% on room air), except for mild tachypnea with a respiratory rate of 22 bpm. ECG demonstrated ST elevations in the inferior and lateral leads (Figure 1). Initial laboratory evaluation revealed elevated lactate, ammonia, high-sensitivity troponin I, and creatine phosphokinase (CPK) levels (Table 1).
On-admission electrocardiogram showing ST-segment elevation in inferior and lateral leads consistent with acute myocardial infarction
A bedside ultrasound showed a reduced ejection fraction (EF) of 30%. The patient underwent emergent cardiac catheterization, which demonstrated non-obstructive CAD, with patent left main and left anterior descending arteries, mild luminal irregularities in the left circumflex artery with approximately 30% proximal stenosis, and a dominant right coronary artery with moderate (40-50%) proximal stenosis. Left ventriculography revealed reduced systolic function with an estimated EF of 25-30% and mid-ventricular wall motion abnormalities. However, he developed cardiogenic shock, requiring vasopressor support and a brief admission to the intensive care unit. Notably, the patient did not report any subsequent chest pain, and his troponin levels gradually decreased. Echocardiography done during hospitalization revealed regional wall motion abnormalities (RWMAs) of the mid-ventricular segments with an EF of 35-40% (Videos 1-2).
Trans-thoracic echocardiography apical four-chamber viewTrans-thoracic Echocardiography apical four-chamber demonstrating a mid-ventricular variant of takotsubo cardiomyopathy, with akinesis involving the mid-lateral and mid-septal segments, with normal apical motion and hyperkinetic basal segment.
Trans-thoracic echocardiography contrast-enhanced viewTrans-thoracic echocardiography contrast-enhanced view re-demonstrating a mid-ventricular variant of takotsubo cardiomyopathy, with akinesis involving the mid-lateral and mid-septal segments, with normal apical motion and hyperkinetic base.
In the absence of obstructive disease, a setting of acute physical stress (seizure), and RWMAs, the patient was diagnosed with a mid-ventricular variant of takotsubo cardiomyopathy. He was initiated on aspirin, statin, beta-blocker, and angiotensin receptor blocker and discharged in a hemodynamically stable position. On follow-up three months after discharge, the patient was found to be doing well, with the repeat echocardiogram showing improvement in ejection fraction to 60% and resolution of RWMAs.
Case 2
A 66-year-old female with a medical history of moderate persistent asthma, obstructive sleep apnea, alpha-1-antitrypsin deficiency, and prior right breast cancer treated with lumpectomy, chemotherapy, and radiation presented to the emergency department with acute shortness of breath following hashish inhalation. Her symptoms were accompanied by central chest pain radiating to the left arm, jaw, and neck.
On admission, she was tachycardic (HR of 110-115), tachypneic (RR of 24-28), hypertensive (BP of 150/90-160/100), and hypoxemic, with oxygen saturation falling to 80% on room air. Examination revealed bilateral expiratory wheezing in the lungs with otherwise normal heart sounds. Chest radiograph showed no acute cardiopulmonary findings, and the initial ECG did not demonstrate ST-segment elevations (Figure 2). Arterial blood gas analysis demonstrated acidemia. Laboratory studies revealed leukocytosis, mildly elevated CRP, and elevated high-sensitivity troponin I levels, peaking at 717 ng/L (Table 2). Further, chest computed tomography with contrast showed no evidence of pulmonary embolism or other significant abnormalities, except for mild emphysematous changes.
On-admission electrocardiogram showing sinus tachycardia with no significant changes consistent with acute ischemia
She was managed for acute hypoxic respiratory failure with noninvasive positive-pressure ventilation, intravenous corticosteroids, antibiotics, magnesium sulfate, and inhaled long-acting muscarinic (LAMA) and β-adrenergic (LABA) agents. Given concern for a non-ST elevation myocardial infarction, she received aspirin and intravenous heparin. A transthoracic echocardiogram revealed RWMAs involving the mid-ventricular segments of the left ventricle, with a reduced ejection fraction of 30-35% (Videos 3-4). In view of rising troponins and new systolic dysfunction, she underwent left heart catheterization, which demonstrated no significant obstructive coronary artery disease. Left ventriculography revealed reduced systolic function with an estimated ejection fraction of 30-35% and mid-ventricular wall motion abnormalities.
Trans-thoracic echocardiography apical two-chamber viewTrans-thoracic echocardiography apical two-chamber imaging demonstrates a mid-ventricular variant of stress cardiomyopathy (takotsubo), characterized by akinesis of the mid-anterior and mid-inferior walls, with sparing of the basal and apical segments.
Trans-thoracic echocardiography contrast-enhanced viewTrans-thoracic echocardiography contrast-enhanced apical four-chamber view demonstrating a mid-ventricular variant of takotsubo cardiomyopathy, with akinesis involving the mid-lateral and mid-septal segments, while apical and basal segments exhibit normal systolic function.
In the absence of ischemic coronary pathology and in the setting of acute physical stress due to hypoxemia, the presentation was consistent with a mid-ventricular variant of stress (takotsubo) cardiomyopathy. She was initiated on aspirin, statin, beta-blocker, and angiotensin receptor blocker and discharged in a hemodynamically stable position. On one-month follow-up, she continued to recover well with no residual symptoms. Her repeat echocardiography done on follow-up demonstrated resolution of RWMAs with normalisation of ejection fraction to 60-65%.
Discussion
TCM, also known as “broken heart syndrome,” is estimated to affect approximately 1-3% of patients presenting with symptoms of acute coronary syndrome (ACS), with the majority of cases occurring in women, particularly postmenopausal women [2]. Although the prevalence is lower in younger age groups, it has been observed to affect more males in this population, especially those with fewer comorbidities or with acute neurological or psychiatric disorders. In such cases, it often presents as atypical variants or as an in-hospital complication [7]. Although apical form remains the most common, the diagnosis of midventricular variant has increased from 18% to 28% from 2004 to 2021 [5]. Patients with this variant typically exhibit mid-ventricular wall motion abnormalities with hyperdynamic apical and basal segments.
Several theories have been proposed regarding the pathogenesis of TCM, with the adrenergic hypothesis being the most widely accepted. In response to severe acute emotional or physical stress, excessive catecholamines are released, resulting in microvascular dysfunction and intracellular calcium overload, further causing catecholamine-induced myocardial damage [3].
The diagnosis of TCM is based on clinical presentation, laboratory findings, and diagnostic imaging. The revised Mayo Clinic diagnostic criteria, which include (a) transient dyskinesis of the left ventricular (LV) mid-segments, (b) regional wall motion abnormalities extending beyond a single epicardial vascular distribution, (c) absence of obstructive CAD or acute plaque rupture, and (d) new electrocardiographic changes or modest troponin elevation, along with the exclusion of pheochromocytoma and myocarditis, is used for establishing the diagnosis [8]. Although it typically mimics ACS, with ischemic changes on the electrocardiogram and elevated troponin levels (as seen in the case presented here), coronary angiography typically reveals no significant obstructive coronary disease [1]. However, co-existing CAD may be present in approximately 15% of patients [9,10]. In such cases, careful correlation between angiographic findings and wall motion abnormalities is necessary. Additional assessments, such as optical coherence tomography and intravascular ultrasound, can help evaluate plaque rupture, which is not characteristic of TCM [11]. Echocardiography is a valuable tool for assessing the location, extent, and severity of RWMAs and detecting complications. Cardiac magnetic resonance imaging (MRI) with gadolinium contrast can further differentiate takotsubo syndrome from acute myocardial infarction and myocarditis by demonstrating an absence of fibrosis, which is consistent with TCM [12].
Follow-up management of TCM focuses on potential relapse due to the recurrence of stressors and resolution of RWMAs, in addition to monitoring for the development of comorbidities and CAD risk factors. Repeat echocardiograms within a few weeks or cardiac MRI when necessary are often used for this purpose. Treatment aims to prevent recurrence, alleviate symptoms, and manage complications. Current protocols recommend using beta-blockers, renin-angiotensin-aldosterone system inhibitor (RAASi), and statins to reduce myocardial stress induced by excessive catecholamine release [13].
Given the risk for the development of complications, the most common of which include LVOT obstruction secondary to hyperdynamic basal segments and cardiogenic shock, the potential for reversibility, and atypical presentations, early diagnosis is crucial for TCM. Prompt and accurate identification allows for effective management of complications and prevention of syndrome recurrence.
Conclusions
We present a case series of mid-ventricular TCM, an uncommon variant of stress-induced cardiomyopathy, triggered by distinct forms of acute physical stress-seizure and hypoxemia. These cases underscore the heterogeneous presentations and multifactorial triggers associated with this atypical subtype. Early recognition, guided by clinical suspicion and confirmed through echocardiography and coronary angiography, is critical for accurate diagnosis and management. Awareness of mid-ventricular variants can prevent misdiagnosis, unnecessary invasive procedures, and ensure timely initiation of supportive therapy, leading to favorable outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reverse takotsubo cardiomyopathy: two case reports and review of the literature J Med Case Rep Patankar GR Choi JW Schussler JM 84720132351007810.1186/1752-1947-7-84PMC 3668300 · doi ↗ · pubmed ↗
- 2Apical ballooning syndrome or takotsubo cardiomyopathy: a systematic review Eur Heart J Gianni M Dentali F Grandi AM Sumner G Hiralal R Lonn E 152315292720061672068610.1093/eurheartj/ehl 032 · doi ↗ · pubmed ↗
- 3Takotsubo cardiomyopathy: a brief review J Med Life Amin HZ Amin LZ Pradipta A 371320203234169310.25122/jml-2018-0067 PMC 7175432 · doi ↗ · pubmed ↗
- 4International expert consensus document on takotsubo syndrome (Part I): clinical characteristics, diagnostic criteria, and pathophysiology Eur Heart J Ghadri JR Wittstein IS Prasad A 203220463920182985087110.1093/eurheartj/ehy 076PMC 5991216 · doi ↗ · pubmed ↗
- 5Temporal trends in takotsubo syndrome: results from the International Takotsubo Registry J Am Coll Cardiol Schweiger V Cammann VL Crisci G 117811898420243921755110.1016/j.jacc.2024.05.076 · doi ↗ · pubmed ↗
- 6Comparison of electrographic changes, clinical features and outcomes in different variants of takotsubo syndrome Int J Cardiol Looi JL Voss J Gilmore J Heaven D Lee M Kerr AJ 13207240620243864379510.1016/j.ijcard.2024.132072 · doi ↗ · pubmed ↗
- 7Age-related differences in takotsubo syndrome: results from the multicenter GEIST registry J Am Heart Assoc El-Battrawy I Santoro F Núñez-Gil IJ 013202410.1161/JAHA.123.030623 PMC 1101007838348805 · doi ↗ · pubmed ↗
- 8Stress cardiomyopathy diagnosis and treatment: JACC state-of-the-art review J Am Coll Cardiol Medina de Chazal H Del Buono MG Keyser-Marcus L Ma L Moeller FG Berrocal D Abbate A 195519717220183030947410.1016/j.jacc.2018.07.072PMC 7058348 · doi ↗ · pubmed ↗