Augmented Reality–Enhanced Simulation in Surgical Education: A Scoping Review of Implementation, Skill Retention, and Equity in Low-Resource Settings
Ee Hng Ian Lim, Li-Zhang Tan, Hui Min Foo, Samuel S Adrian

TL;DR
This paper reviews how augmented reality (AR) can help train surgeons, especially in low-resource settings, but finds that more research is needed to confirm its long-term effectiveness and fairness.
Contribution
The study provides a scoping review of AR's role in surgical education, focusing on implementation, skill retention, and equity in low-resource contexts.
Findings
AR is mainly used for visual guidance and procedural training in simulated environments.
Evidence for long-term skill retention and clinical transferability is limited.
Low-resource AR systems show promise but are constrained by small samples and subjective measures.
Abstract
Many developments have been made to enhance surgical training, including the usage of augmented reality (AR) simulation. However, its implementation within surgical training programs, impact on skill retention, and applicability in low-resource settings remain unclear. A scoping review was used to explore the role of AR technology and its implementation in surgical education, maintenance of skill retention, and equity and access in low-resource settings. A systematic search was conducted across four databases, which yielded 185 records, of which 30 met the inclusion criteria. Most studies were published after 2019 and evaluated AR interventions in simulated environments involving medical students or residents. AR intervention was primarily used for visual guidance, telestration and image overlay. Evidence for skill retention remains limited, with only four studies assessing retention…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
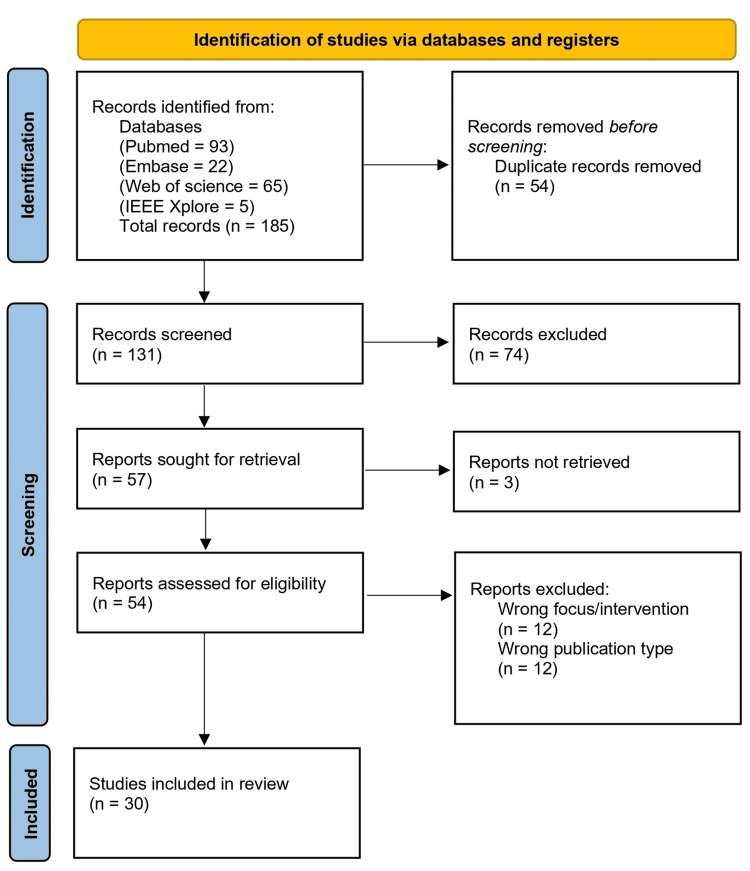 Figure 1
Figure 1| Study (First author) | Year | Country | Study design | Learner level | Surgical specialty | AR intervention |
| Vera et al. [ | 2014 | USA | RCT | Medical students | Laparoscopic surgery | AR telementoring overlays guiding suturing task |
| Heinrich et al. [ | 2021 | Germany | Pre-clinical within-subject crossover trial | Residents, consultants | General surgery | HoloLens-based AR pointer providing task guidance |
| Ghenbot et al. [ | 2024 | USA | Cadaveric within-subject experimental study | Medical student, resident, consultants | Neurosurgery | HoloLens 2 AR navigation with spine anatomy overlays |
| Acar et al. [ | 2024 | USA | Within-subject experimental study | Residents/Fellows, consultants | Urology | Mixed-reality gaze-sharing AR for ureteroscopy training |
| Kambakamba et al. [ | 2024 | Switzerland | Prospective pilot study | Senior residents | General surgery | Smart-glasses AR telementoring during procedures |
| Lovett et al. [ | 2024 | USA | RCT | Medical students | General surgery | HoloLens AR suture-guidance overlays |
| Yeo et al. [ | 2011 | Canada | RCT | Residents, medical/bio-engineering students | Interventional radiology/spinal surgery | AR-guided needle placement using hybrid simulator |
| Felinska et al. [ | 2023 | Germany | Randomised-controlled crossover trial | Medical students | Laparoscopic surgery | iSurgeon (AR telestration) Visual guidance during training. |
| Nagayo et al. [ | 2022 | Japan | RCT | Medical students | General surgery | HoloLens 2-based AR training providing task guidance |
| Guerrini et al. [ | 2024 | Italy | Prospective observational study | Medical students | Neurosurgery | UpSurgeOn simulators (Mycro & AR neuroanatomy)- microsurgical suturing and AR neuroanatomical models. |
| Cizmic et al. [ | 2023 | Germany | Randomized controlled two-arm study | Medical students | Laparoscopic surgery | iSurgeon (AR telestration) visual guidance during training. |
| Feifer et al. [ | 2008 | Canada | Prospective cohort study | Residents | Urology | ProMIS hybrid simulator (Haptica) –provides haptic feedback and records movement efficiency. |
| Logishetty et al. [ | 2019 | UK | RCT | Medical students | Orthopaedics | HoloLens headset with MicronTracker – Provides real-time holographic feedback during simulated THA. |
| Alaraj et al. [ | 2013 | USA | Descriptive early validation study | Residents | Neurosurgery | ImmersiveTouch system – AR surgical simulator for neurosurgical procedures |
| Wu et al. [ | 2025 | Switzerland | Development/feasibility study | Residents | Orthopaedics | Custom HoloLens 2 AR-based surgical simulator |
| Berger et al. [ | 2025 | Austria | Prospective cohort study | Residents | Neurosurgery | Video + AR training with neurosurgical simulators |
| Coelho et al. [ | 2020 | Brazil | Phase I mixed-methods validation study | Consultants | Neurosurgery | Mixed-reality neurosurgical simulation platform |
| Alonso-Silverio et al. [ | 2018 | Mexico | Experimental development and validation study | Consultants, residents, medical students | General surgery | Low-cost hybrid laparoscopic trainer with AR guidance |
| Moglia et al. [ | 2024 | Italy | Preclinical usability and performance study | Consultants, residents, medical students | Orthopaedics | Holoknee (AI + MR) – AR knee planning and guidance with AI 3D segmentation. |
| Barzilai et al. [ | 2025 | Israel | RCT | Medical students | Otolaryngology | HoloLens 2 - AR-guided mastoidectomy simulator |
| Wolf et al. [ | 2024 | USA | Experimental | Surgical trainees | General surgery | Tablet-based AR surgical training environment |
| Shaaban et al. [ | 2024 | USA | Cross-sectional pre/post survey study | Medical students, residents | Neurosurgery | Hybrid physical–AR anatomical simulation model (UpSurgeOn system) |
| Cuba et al. [ | 2024 | Switzerland | Prospective performance and learning curve study | Residents | Neurosurgery | Patient-specific mixed-reality surgical simulator (HoloLens 2) |
| Ropelato et al. [ | 2020 | Switzerland | Experimental validation study | Physician trainees | Opthalmology | Custom AR microsurgery training simulator with HoloLens display |
| P. Jain et al. [ | 2024 | India | Two-phase mixed-methods user perception study | Residents, consultants | Laparascopic surgery | Conceptual AR simulator for surgical education |
| Shepard et al. [ | 2025 | USA | Prospective randomized crossover trial | Residents | Neurosurgery | Remote mixed-reality training using Vuzix smart glasses |
| Aydoseli et al. [ | 2024 | Turkey | Quantitative descriptive survey study | Residents | Neurosurgery | Illumetry XR screen with ArSurgeon software used to display segmented 3D MRI and CT images of neurosurgical cases |
| Nugent et al. [ | 2013 | Ireland | Prospective validation and skill acquisition study | Consultants, Medical students, surgical trainees | General surgery | ProMIS AR laparoscopic simulation system |
| Stone et al. [ | 2022 | USA/Netherlands | Proof-of-concept and beta testing study | Surgical trainees/ residents | Urology | Custom AR headset with heads-up display for task guidance |
| Colman et al. [ | 2025 | UK | Mixed-methods multicenter pilot validation study | Trainees, consultants | General Surgery | LapAR™ augmented-reality laparoscopic simulator |
| Study | Retention interval | Retention type | Retention measure | Retention findings |
| Berger et al. [ | 14 days | Short-term | Tremor metrics, performance trend: reduction in wrist tremor over training. | Significant tremor reduction across groups and experience levels |
| Moglia et al. [ | 1 week between trials | Short-term | Task completion time, usability | Significant improvement in task speed, MR effective for training, planning and guidance |
| Wolf et al. [ | 1 week between AR training and cadaveric assessment | Short-term | Procedural knowledge MCQ, tablet-based procedural skills, cadaveric procedural performance | Significant improvement in tablet procedure knowledge and skills. No transfer to cadaveric skill performance |
| Shepard et al. [ | 2 months | Long-term | Procedural success, puncture attempts, procedure time, retention scores | Skills maintained at 2 months, MR training equivalent to IP training, preference of IP training due to hardware discomfort |
| Study | Equity focus/Objective | Key findings on equity | Challenges/Barriers | Reviewer notes |
| Guerrini et al. [ | Address neurosurgical training gaps through sustainable, low-cost simulation programs targeting low-resource settings | Simulation increased interest in surgical careers and self-reported confidence; program model supports repeated training in low-resource regions | No control group; self-reported outcomes; short-term exposure; no skill or retention measures | Direct equity focus via Mission:Brain’s LMIC-oriented training and sustainability model |
| Coelho et al. [ | Develop a reusable, lower-cost ventriculostomy simulator suitable for resource-limited training environments | Simulator demonstrated high perceived realism and usability; reusability and local production support affordability in LMIC contexts | No objective performance or retention outcomes; subjective measures only. Small expert-only sample. | Direct equity relevance; developed in an LMIC with explicit low-resource training rationale |
| Alonso-Silverio et al. [ | Develop a low-cost, open-source AR training system for use in resource-limited settings | Significant task improvement with AR system. Demonstrated reliable, affordable, and objective laparoscopic skill assessment | No long-term retention or clinical transfer assessment. Small sample size. | Strong direct equity relevance; open-source, LMIC-developed, highly scalable |
| Barzilai et al. [ | Evaluate AR-guided mastoidectomy using low-cost 3D-printed models as an alternative to cadaveric training | AR significantly improved novice performance; low-cost printed models support repeatable training | High cost of AR headset; single-session design; no LMIC deployment | Direct but moderate equity relevance; affordability discussed but tested in high-resource setting |
| Wolf et al. [ | Tablet-based AR designed for distributed, portable training in austere/limited-access settings | AR improved knowledge and procedural planning; portable tablet allows deployment in field-like environments | No haptic feedback; short-term evaluation; no actual skill transfer to cadaveric performance | Directed toward access in resource-limited/expeditionary contexts; moderate equity relevance |
| Shaaban et al. [ | Demonstrate AR-physical hybrid simulation as cost-effective, reusable, and scalable for low-cadaver-access / LMIC settings | Participants reported improved confidence and satisfaction; course setup eliminates biohazard and storage barriers, supporting scalable training | Single-session survey; no objective skill or retention data; conference setting limits realism | Direct high-equity relevance; explicit LMIC applicability and low-resource design |
| Jain et al. [ | Develop cost-effective, scalable video-based AR workflow for laparoscopic/MIS training in low-resource settings | Strong user interest and perceived usefulness; scalable, low-cost workflow suitable for institutions without expensive hardware | Perception-only study; no hands-on performance or retention data; small follow-up cohort | High equity relevance; LMIC-focused, feasibility demonstrated; next step: prototype testing |
| Shepard et al. [ | Evaluate remote MR training as an alternative to in-person instruction, potentially expanding access to smaller or resource-limited centers | MR training equivalent to in-person for skill acquisition and retention; enables remote expert guidance | Hardware cost and connectivity; small sample; single institution; trainee preference for in-person | Moderate equity relevance; demonstrates remote access potential but limited by equipment and connectivity |
| Aydoseli et al. [ | Evaluate low-cost XR/AR neuronavigation for neurosurgery training, with potential applicability in low-resource settings | AR improved motivation and perceived anatomical mastery; device is affordable and easily reproducible | Single-session, subjective survey; no objective performance or retention metrics; not tested in LMICs | Moderate equity relevance; cost-effective design with potential for low-resource deployment |
| Stone et al. [ | Evaluate remote AR telementoring platform to expand access and reduce travel/costs for surgical training | Remote AR enabled successful simulated procedures across geographic distances; inexpensive phantoms and consumer hardware support scalable training | Small sample, no objective skill metrics or retention testing; single-session; high-resource sites | Moderate equity relevance; strong feasibility demonstration with potential for low-resource deployment |
| Colman et al. [ | Evaluate home-based AR laparoscopic simulator to increase accessibility and equity in early surgical training | Trainees improved completion time (52%), instrument path (38%), and qualitative feedback strongly positive; remote, low-infrastructure design supports broader access | Small sample, no real-OR transfer, no long-term retention; minor technical issues | High equity relevance; decentralized, low-resource-compatible AR training with strong feasibility and trainee acceptance |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical Simulation and Training · Augmented Reality Applications · Simulation-Based Education in Healthcare
Introduction and background
Surgical training increasingly faces challenges like limited operative exposure, patient safety concerns and disparities in access between low and high-income areas [1]. Simulation-based technology has emerged as a solution to address these issues, enabling autonomous and low-stakes surgical training [2]. Among upcoming simulation technologies, augmented reality (AR) provides a combination of digital imaging with physical interactions, making it a useful adjunct for traditional surgical teaching [3].
AR is defined as technology that overlays computer-generated digital content onto the real-world environment in real time [4]. This differs from virtual reality (VR), which consists entirely of virtual objects, and mixed reality (MR), that merge real and virtual worlds such that physical and digital objects coexist and are presented together [4]. By augmenting digital media over the physical environment, AR can serve as a technological platform to deliver surgical education, such as displaying surgical techniques over a human cadaver [5]. Despite growing interest and technological advances, it is unclear whether AR is effective in its implementation in surgical education, including its usefulness in skill retention and applicability in low-resource settings.
This scoping review was used to provide a comprehensive overview of the research conducted within AR in surgical education, as well as identify potential gaps in the literature. Specifically, this review was conducted to evaluate the approaches to integration of AR in its: (1) implementation in surgical education, (2) skill retention, and (3) equity and feasibility in low-resource settings.
Review
Methods
Study Design
The protocol for this review was conducted using the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA), specifically the PRISMA extension for scoping reviews (PRISMA-ScR) [6]. Institutional Review Board (IRB) and ethical approvals were not required, as this was a secondary data synthesis of published literature. Moreover, the personal information of participants was not revealed in the reviewed studies, and no external funding was involved.
Inclusion and Exclusion Criteria
To map out our objectives, this review follows the PICO (population, intervention, comparator, outcome) framework. The target population was medical students, doctors, and surgical trainees. The intervention investigated was an AR-based simulation. As a comparison, the population subjects had to use or have access to AR technology, versus a control setting (e.g., video tutorials). Some single-arm studies were also included to map the breadth of existing evidence and implementation experiences. The outcomes assessed included its effectiveness in surgical education, long-term skill retention, or equity and feasibility in resource-limited settings. In addition, peer-reviewed articles were included if they were: in English, primary research, and from any publication year.
To be included in the review, studies needed to focus on AR-based simulations in surgical training, adhering to the PICO framework. Examples of why papers were excluded involved VR simulations, not written in English, first-aid/multiple casualty incident simulations, review-type articles and animal studies without human training outcomes. Reports where full text was not retrievable (e.g., abstract-only publications) were not assessed for eligibility and excluded under “reports not retrieved” as shown in the PRISMA-ScR flow diagram (Figure 1).
PRISMA flow chartPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Search Strategy and Planning
To identify the relevant studies, the following bibliographic databases were searched on the 21st of August 2025: Embase, Web of science, IEEE web Xplore and Pubmed. Boolean logic, keywords, phrases and synonyms were applied to title and abstract field to expand the literature search. Controlled vocabulary (e.g., MeSH) was not used because emerging immersive technologies are frequently described interchangeably (e.g., AR, MR, and VR) without consistent or formal definitions, resulting in unreliable indexing. An example of the search strategy is included in the Appendices section. The final search results were uploaded to Rayyan (Rayyan Systems Inc., Cambridge, MA, US), a web tool for sorting articles. Rayyan was then used to detect duplicate studies which were subsequently removed. Three researchers (IL, EF, LZT) individually sorted abstracts of articles based on the inclusion and exclusion criteria. An external reviewer (SS) was used to resolve any conflicts that arose during decision-making. Next, the abstracts that were included were reuploaded onto Rayyan as full-text articles. The three researchers then evaluated the full text of the included studies. Further conflicts between the reviewers were resolved in a 2:1 favor. A review of the finalized studies was conducted by all the researchers to appraise their quality and check for adherence to the eligibility criteria.
Results
The literature search identified 185 records. After removing 54 duplicates, 131 records were screened by title and abstract. During this process, 74 results were excluded. 57 full-text articles were sought for retrieval, and three were removed due to lack of full-text availability. The remaining 54 articles were assessed for eligibility, with 30 studies included in the final synthesis.
The articles are described in Table 1 together with the publication year, country, study design, learner level, surgical specialty and AR intervention.
Most included studies were published after 2019. Early articles focused on hybrid simulators and guidance using AR, whereas more recent studies emphasize head-mounted displays, mixed reality simulators, AI integration and telementoring. Residents dominated feasibility, validation, and learning-curve studies, while medical students were the primary participants of randomized control trials (RCTs), particularly in general surgery and laparoscopic training (Table 1).
Implementation of AR-Enhanced Simulation
Across included studies, AR technology served three primary roles: (1) visual guidance/image overlay, (2) navigation and anatomy visualisation, and (3) telestration and gaze-sharing. Visual guidance and image overlay was mainly applied to RCTs, involving novice learners such as medical students (Table 1). This role primarily evaluated short-term performance outcomes and had the largest representation among study types. In contrast, navigation and anatomy visualization was often applied to specialized surgical fields, such as ear, nose, or throat (ENT) or neurosurgery, with outcomes focusing on enhancing spatial understanding and pre-operative planning (Table 1). Telestration and gaze-sharing were examined in fewer studies and were mainly implemented with senior trainees, emphasizing real-time expert feedback and mentorship (Table 1).
Reporting of study settings and curricular integration was variable. Twenty-two out of the 30 included studies explicitly reported study settings (73%), such as simulation/skills labs, operating theatres and home-based/remote training. Formal integration into surgical curricula was reported in six out of 30 studies (20%).
Skill Retention Outcomes
Skill retention is defined as the maintenance of acquired skills following a period without practice [37]. As seen from Table 2, four out of 30 studies assessed skill retention outcomes.
Short-term retention was evaluated by three of the four studies [22,25,27]. The retention intervals ranged from one week to two months. Berger et al. reported a significant reduction in wrist tremor (56-69%) even after a one-week delay, consistent among junior and senior residents [22]. There were also improvements in task time completion after a one-week interval in Moglia et al., indicating short-term maintenance in procedural efficiency [25]. Wolf et al. also displayed improvements in AR procedural skills and knowledge (p<0.001) on tablet-based platforms. However, no significant improvement in cadaveric task performance was observed [27].
Long-term retention was assessed by one out of the four studies. With a two-month retention interval, urological residents were still able to carry out ultrasound-guided percutaneous nephrolithotomy in both AR and in-person training groups. Post-test to retention test yielded insignificant decreases in average performance scores. Procedural skill was maintained two months post-training [32].
Equity and Low-Resource Settings
Several studies (n=11/30) designed affordable, usable, and scalable simulation tools for surgical training in low-resource settings/low-middle income countries (LMICs) by using open-source approaches and local production. Many of these systems were created to reduce reliance on cadavers or high-cost infrastructure (Table 3).
Across studies, AR interventions were associated with increased learner confidence, motivation, and procedural understanding, alongside improved task performance and procedural planning (Table 3). Several AR systems supported remote training, enabling repeated practice at low cost (Table 3).
This scoping review synthesizes evidence in three areas: implementation of AR into surgical education, skill retention using AR, and equity and access in low-resource settings. Most AR systems were mainly focused on visual guidance and image overlay, primarily involving medical students or novice trainees (Table 1). Evidence on long-term skill retention, clinical transfer, and implementation in low-resource settings remains limited.
Discussion
Implementation of AR
Most AR interventions are carried out in simulated environments, limiting evidence on skills transfer to operating theatres, reflecting on the early developmental stage of AR surgical education [38]. The heterogeneity of AR systems presents a challenge to standardized curriculum integration, with variable performance metrics, training requirements, and inconsistent equivalence to in-person instruction [39]. AR provides a low-stakes environment for surgical training, potentially increasing competence, confidence, and patient safety [40]. Certain AR devices support remote or home-based practice, increasing training opportunities outside clinical settings [36]. However, the inconsistent reporting of study settings and limited documentation of curricular integration restricts assessments on the feasibility and scalability of AR training. Overall, AR provides a promising platform for surgical training, but effectiveness in clinical settings with standardization of performance metrics need to be evaluated.
Impact on Skill Retention
The evidence on AR skill retention remains limited. Short-term retention outcomes suggest improvements in procedural efficiency (Table 2). However, only one out of the 30 studies assessed long-term skill retention, hence evidence for sustained skill transfer remains limited. Moreover, AR-enhanced training remained unable to transfer to cadaveric performance - indicating further refinement is needed before application to real-world contexts [26]. AR systems provide objective feedback on metrics such as skill scores, movement efficiency and technique consistency, allowing potential standardization of training compared with traditional hands-on sessions [38]. This finding, along with opportunities for autonomous practice and spatial guidance, may support skill retention; however, the extent to which these features confer long-term advantages over conventional methods remain uncertain and require further evaluation [41].
Equity and Access in Low-Resource Settings
AR-based simulations are frequently shown as tools to reduce disparities in surgical training by offering low-cost, reusable, and decentralized training opportunities [42]. However, most AR studies were conducted in high-resource settings, limiting the extent of its evaluation of equity and access in low-resource environments. In addition to small sample sizes, a lack of objective skill metrics, single training sessions, high production cost, and ergonomic constraints [40], successful AR implementation depends on infrastructure requirements such as reliable high-speed internet, compatible hardware, and technical support. The availability of such infrastructure across many LMIC training institutions is uncertain and inconsistently reported, complicating assessments of real-world feasibility and scalability [43]. Subsequently, well-designed studies conducted directly within low-resource settings are required to evaluate whether AR-based training can be equitably and practically implemented.
Research Gaps, Limitations, and Future Directions
Overall, AR is a potential tool for surgical training, but there are gaps in the literature that need to be addressed before its implementation. Future research should employ more rigorous and standardized designs, including clearly-defined retention intervals (e.g., three to six months), validated objective performance metrics and assessment of skill transfer to real-world clinical settings. Studies conducted in low-resource settings are needed to evaluate feasibility and equity, alongside cost-effectiveness and infrastructure requirements. Such approaches would strengthen the evidence base for AR integration into surgical training.
Our scoping review has limitations. Firstly, since this is a scoping review, we did not conduct a thorough quality appraisal of each study. Secondly, publication bias may be present, as studies reporting negative or null findings are less likely to be published and therefore underrepresented. Moreover, heterogeneity in study design, interventions, and outcome measures limited direct comparisons of effectiveness. Finally, limiting inclusion to English-language publications may have introduced language bias.
Conclusions
This scoping review highlights the growing potential of AR in surgical education, applied across three domains: implementation into surgical curricula, skill retention and equity in low-resource settings. AR interventions were primarily focused on image overlay and visual guidance for novice learners, demonstrating short-term improvements in procedural efficiency and spatial understanding. However, evidence on long-term skill retention, transfer to real-world clinical practice, and standardized curriculum integration remains limited. Similarly, while AR has the potential to provide low-cost and decentralized training opportunities, most studies were conducted in high-resource environments, and real-world feasibility in LMICs is yet to be thoroughly evaluated.
Future research should focus on rigorous, longitudinal, and equity-oriented studies to assess skill retention over longer intervals, objective performance metrics and transfer to real clinical environments. In addition, studies implemented directly in low-resource settings are needed to demonstrate feasibility, cost-effectiveness, and infrastructure requirements. Addressing these gaps in AR will be critical to ensure AR technology can be effectively, equitably and sustainably integrated into surgical training, overall enhancing learning outcomes and potentially improving patient care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Challenges and opportunities to advance surgical education: a qualitative study Global Surg Educ Yan Y Krusing MB Awad MM Stefanidis D 7842025
- 2A systematic review of the educational effectiveness of simulation used in open surgery Simul Healthc Heskin L Simms C Holland J Traynor O Galvin R 51581420193060146910.1097/SIH.0000000000000349 · doi ↗ · pubmed ↗
- 3Validity and effectiveness of augmented reality in surgical education: a systematic review Surgery Kovoor JG Gupta AK Gladman MA 889817020213374400310.1016/j.surg.2021.01.051 · doi ↗ · pubmed ↗
- 4Augmented reality: a class of displays on the reality-virtuality continuum Telemanipul Telepresence Technol Milgram P Takemura H Utsumi A Kishino F 23511994
- 5Augmented reality-based surgery on the human cadaver using a new generation of optical head-mounted displays: development and feasibility study JMIR Serious Games Puladi B Ooms M Bellgardt M 010202210.2196/34781 PMC 908687935468090 · doi ↗ · pubmed ↗
- 6PRISMA extension for scoping reviews (PRISMA-Sc R): checklist and explanation Ann Intern Med Tricco AC Lillie E Zarin W 46747316920183017803310.7326/M 18-0850 · doi ↗ · pubmed ↗
- 7Augmented reality telementoring (ART) platform: a randomized controlled trial to assess the efficacy of a new surgical education technology Surg Endosc Vera AM Russo M Mohsin A Tsuda S 346734722820142496285610.1007/s 00464-014-3625-4 · doi ↗ · pubmed ↗
- 8Holo Pointer: a virtual augmented reality pointer for laparoscopic surgery training Int J Comput Assist Radiol Surg Heinrich F Huettl F Schmidt G Paschold M Kneist W Huber T Hansen C 1611681620213309542410.1007/s 11548-020-02272-2PMC 7822765 · doi ↗ · pubmed ↗