Tumour microenvironment and HER2-low status dictate response and resistance to anthracycline-taxane chemotherapy in premenopausal TNBC: a retrospective multicohort study
Shuanglong Cai, Shaohong Yu, Quan Zhou, Fangyuan Kuang, Lingyan Rao, Zhen Fang, Xiaoxin Zheng, Yong Shi, Jingdan Li

TL;DR
This study shows that the tumor environment and HER2-low status affect how premenopausal TNBC patients respond to standard chemotherapy, offering new ways to personalize treatment.
Contribution
The study identifies sTIL levels and HER2-low status as novel biomarkers for predicting chemotherapy response in premenopausal TNBC.
Findings
Low stromal tumor-infiltrating lymphocytes (sTIL) and HER2-low status are linked to worse disease-free survival in premenopausal TNBC patients.
A predictive nomogram combining sTIL, HER2 status, and staging achieved high accuracy in predicting chemotherapy outcomes.
HER2-low tumors may benefit from antibody-drug conjugates, while sTIL-low tumors could respond better to immunomodulatory therapies.
Abstract
Premenopausal women with triple-negative breast cancer (TNBC) exhibit considerable heterogeneity in their response to standard anthracycline and taxane-based chemotherapy, yet the underlying mechanisms remain poorly understood. We aimed to investigate the combined role of the tumour immune microenvironment and HER2-low status in predicting chemosensitivity and intrinsic resistance in this specific population. We retrospectively analysed data from 767 premenopausal patients with TNBC across two Chinese medical centres. All patients underwent primary surgery followed by adjuvant chemotherapy based on anthracyclines and taxanes. Patients were randomly assigned to training and internal validation cohorts. Independent predictors of DFS were identified using multivariable Cox proportional hazards regression, and a nomogram was constructed accordingly. The model’s discrimination was assessed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
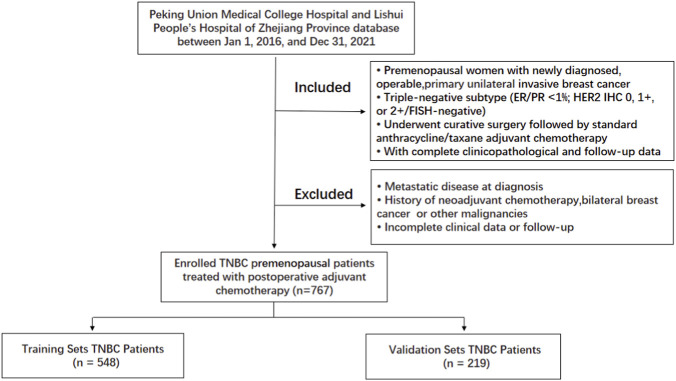 FIGURE 1
FIGURE 1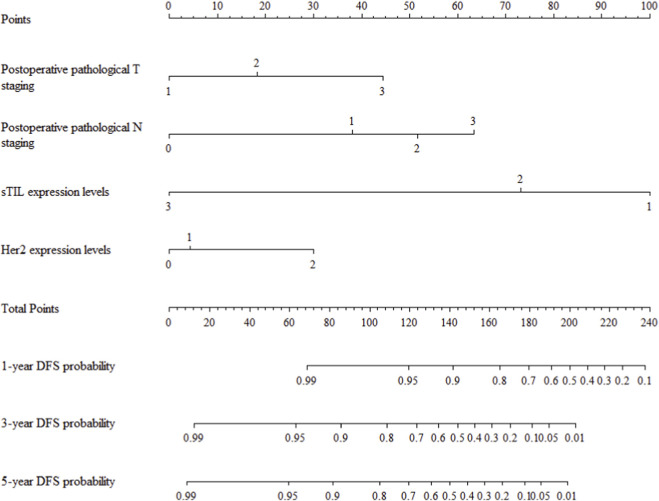 FIGURE 2
FIGURE 2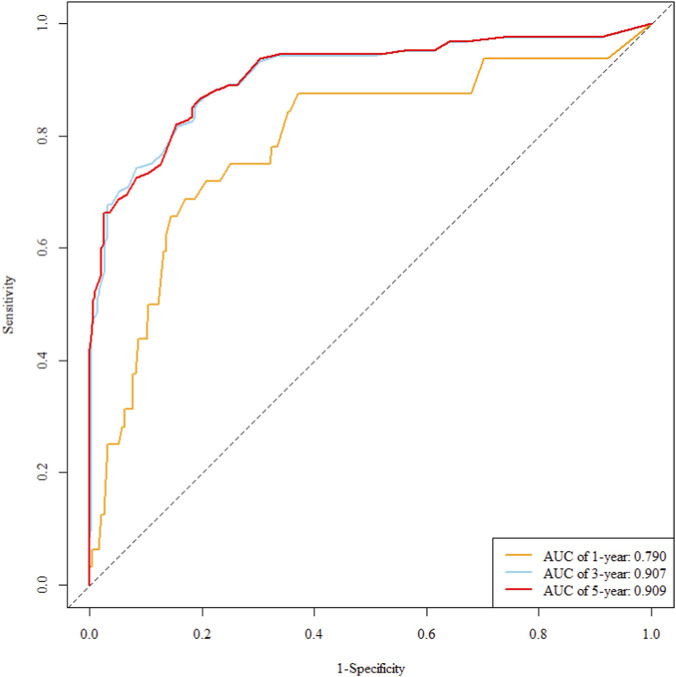 FIGURE 3
FIGURE 3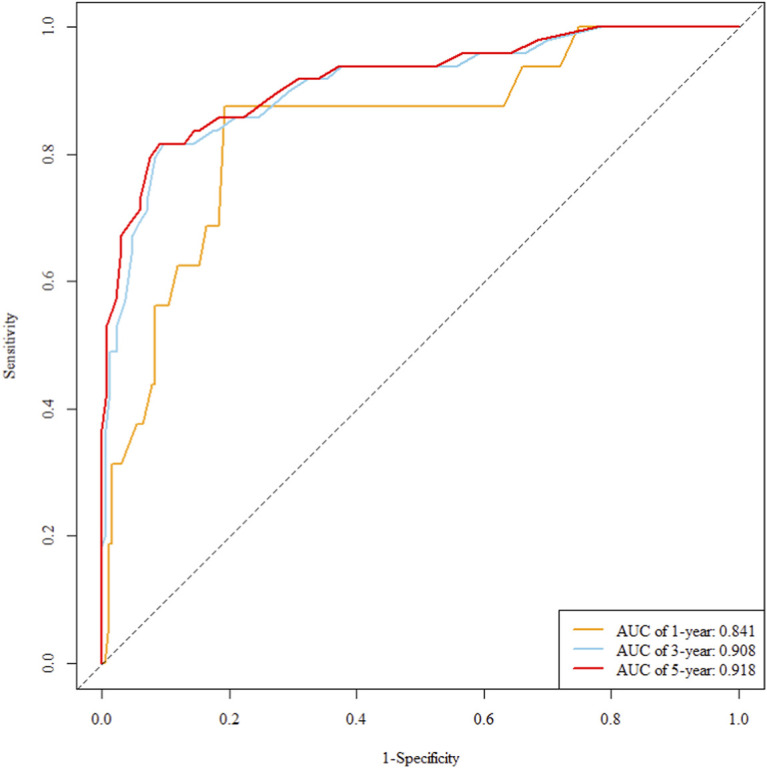 FIGURE 4
FIGURE 4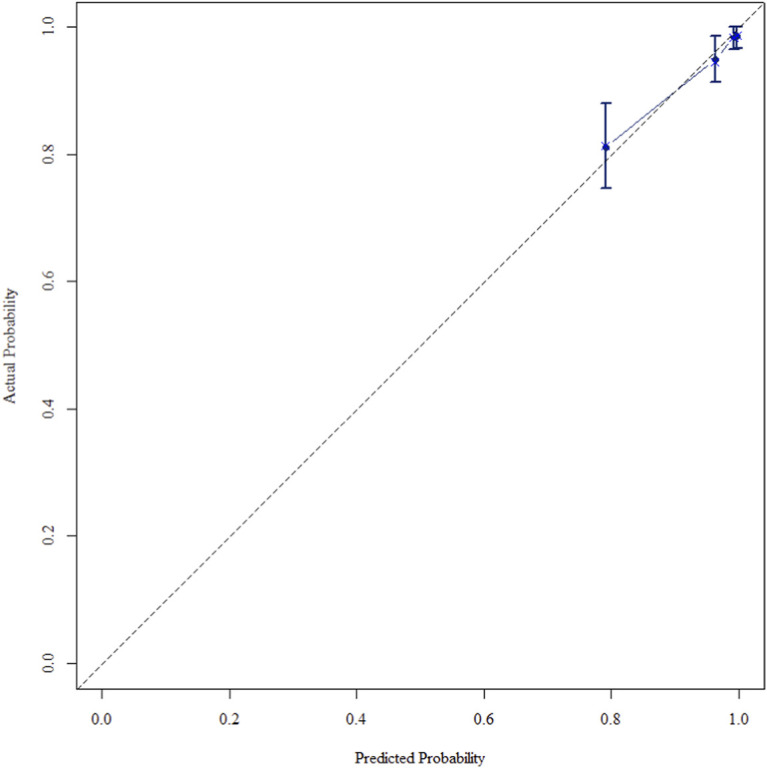 FIGURE 5
FIGURE 5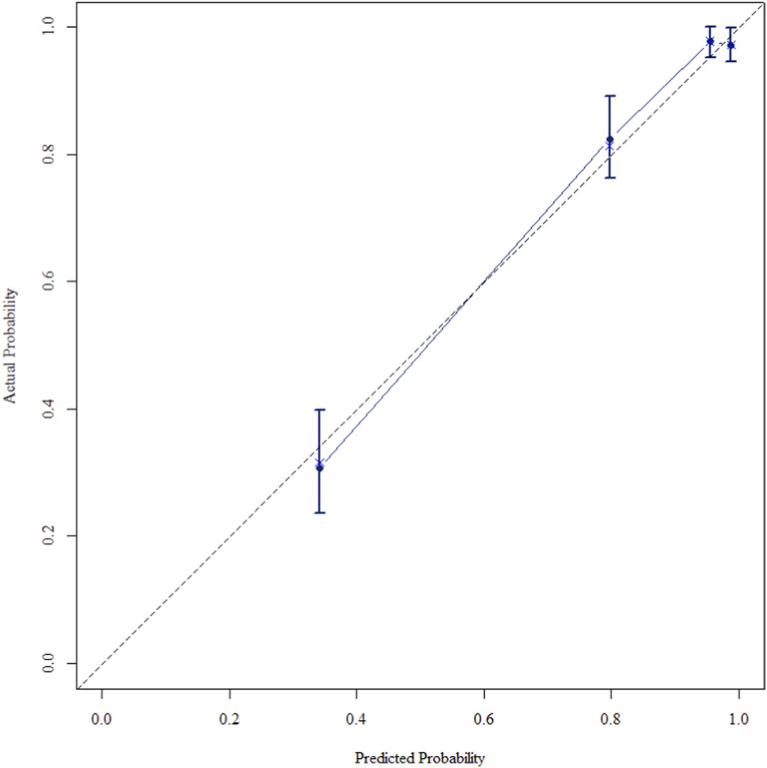 FIGURE 6
FIGURE 6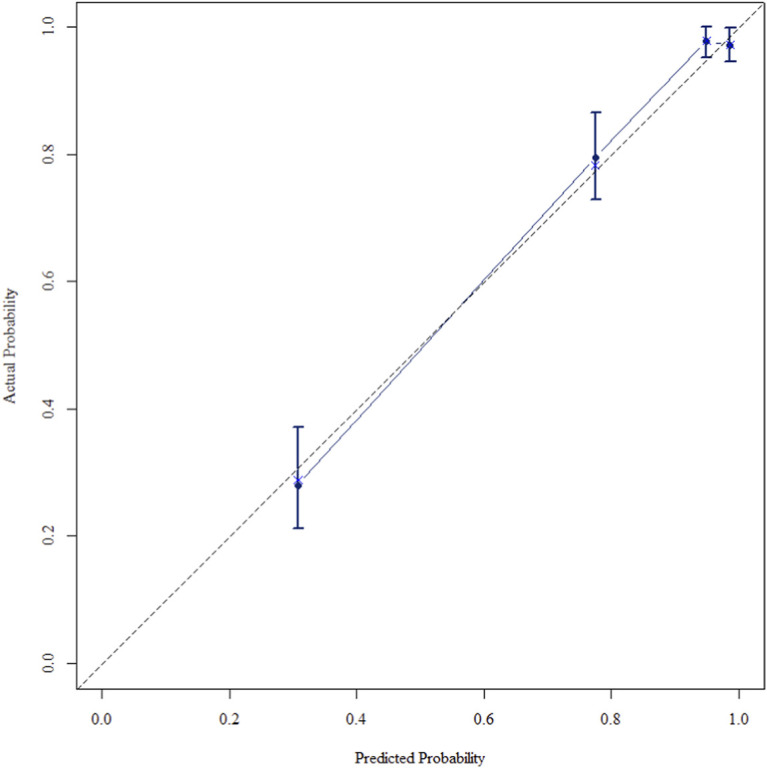 FIGURE 7
FIGURE 7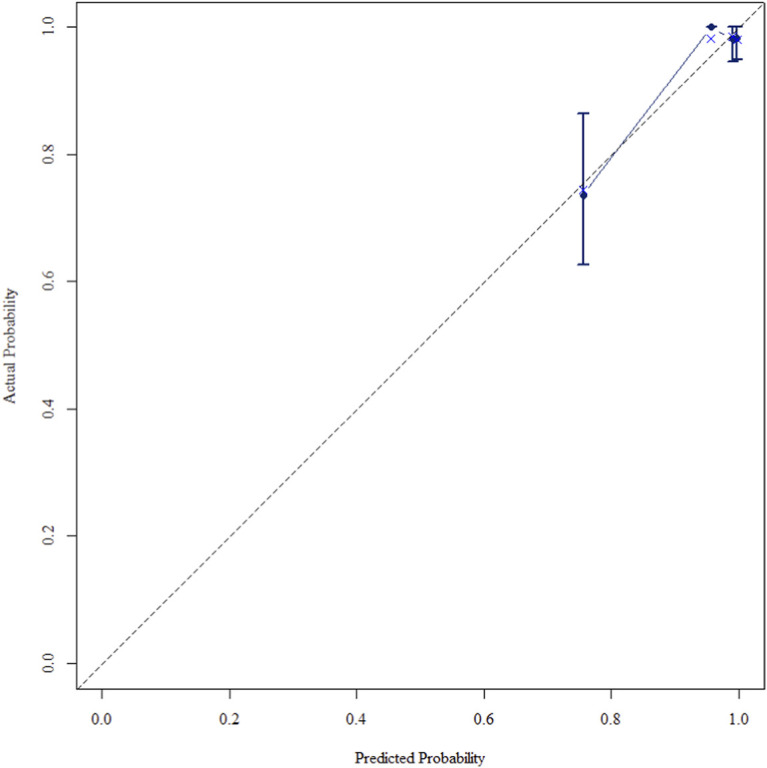 FIGURE 8
FIGURE 8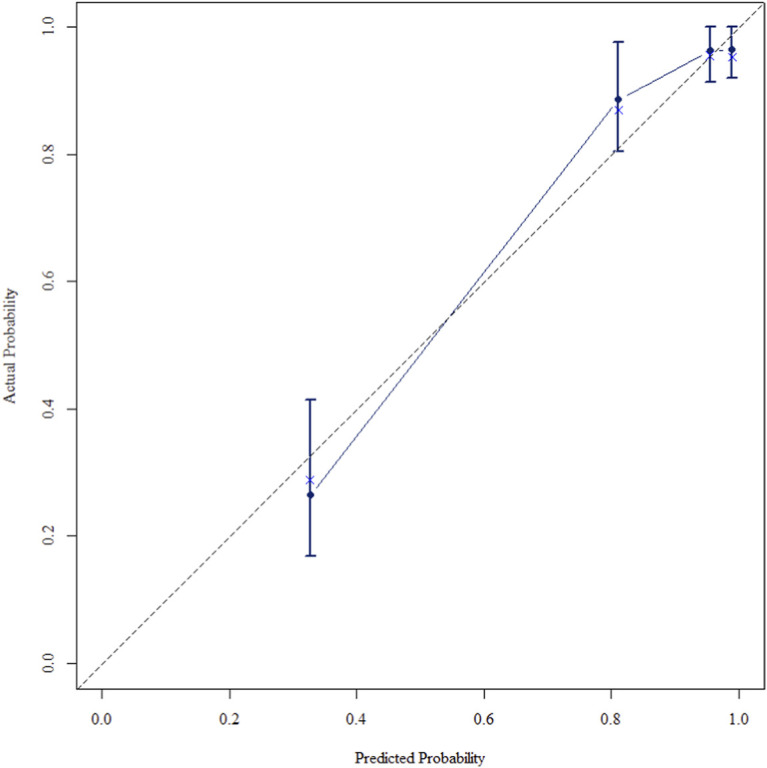 FIGURE 9
FIGURE 9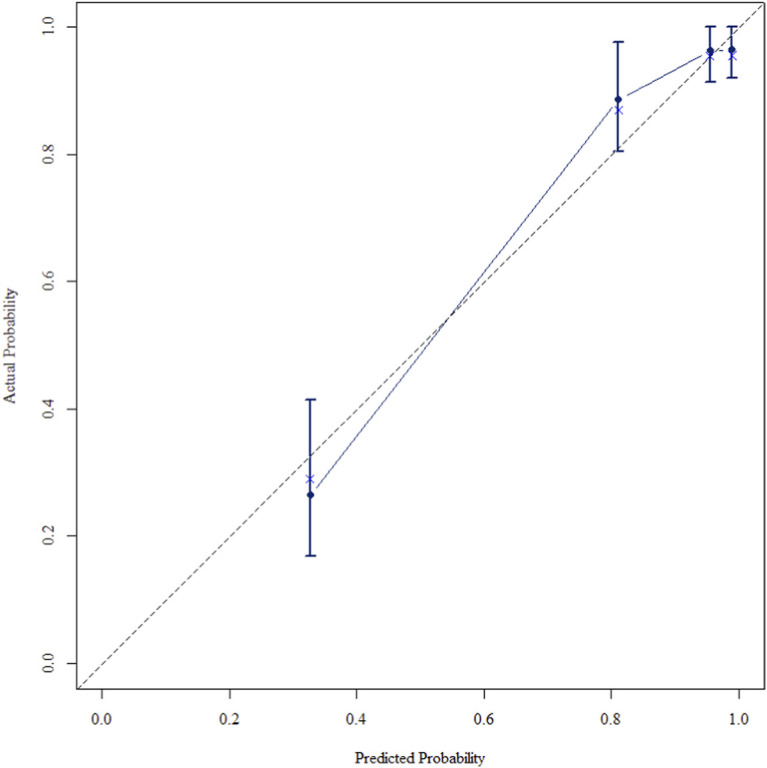 FIGURE 10
FIGURE 10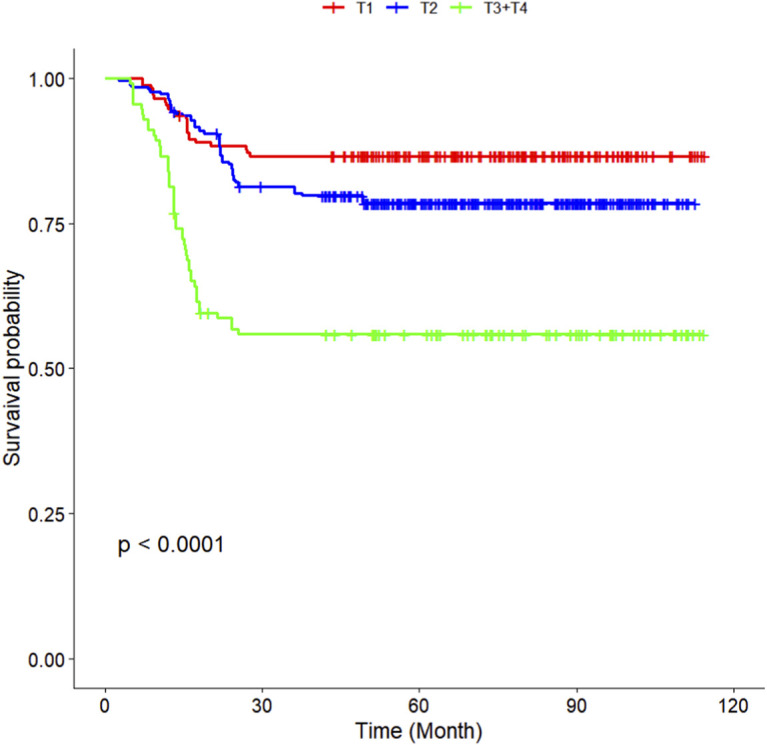 FIGURE 11
FIGURE 11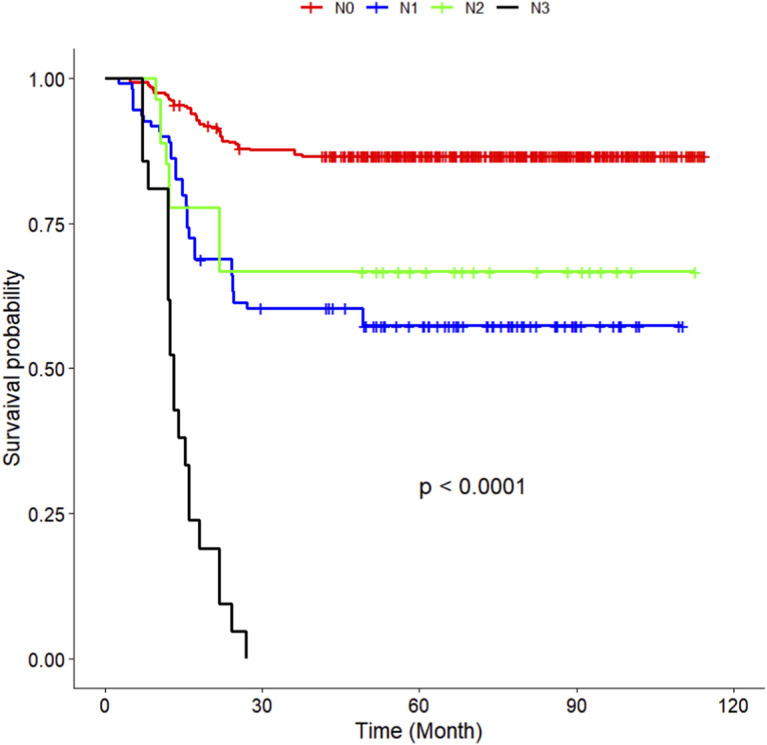 FIGURE 12
FIGURE 12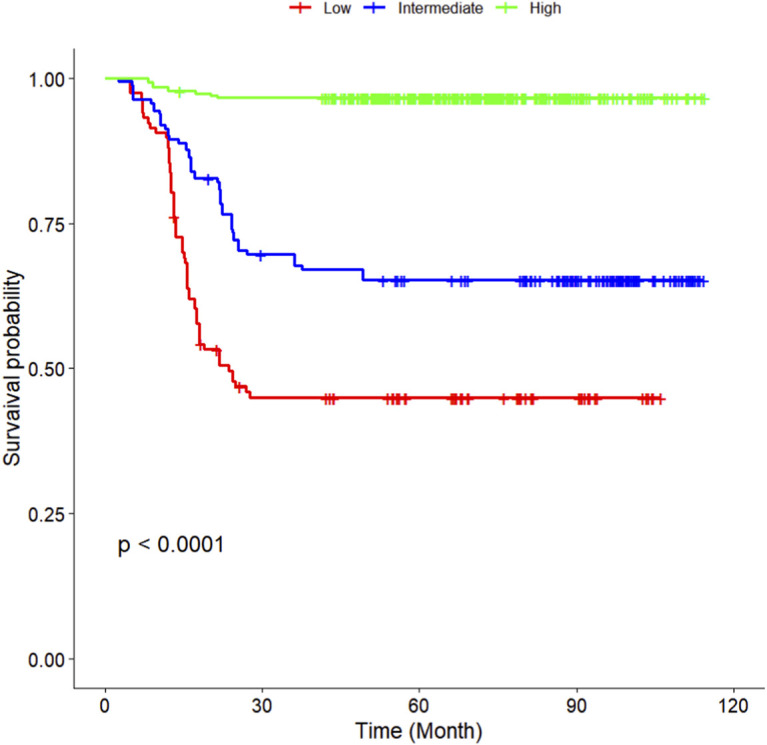 FIGURE 13
FIGURE 13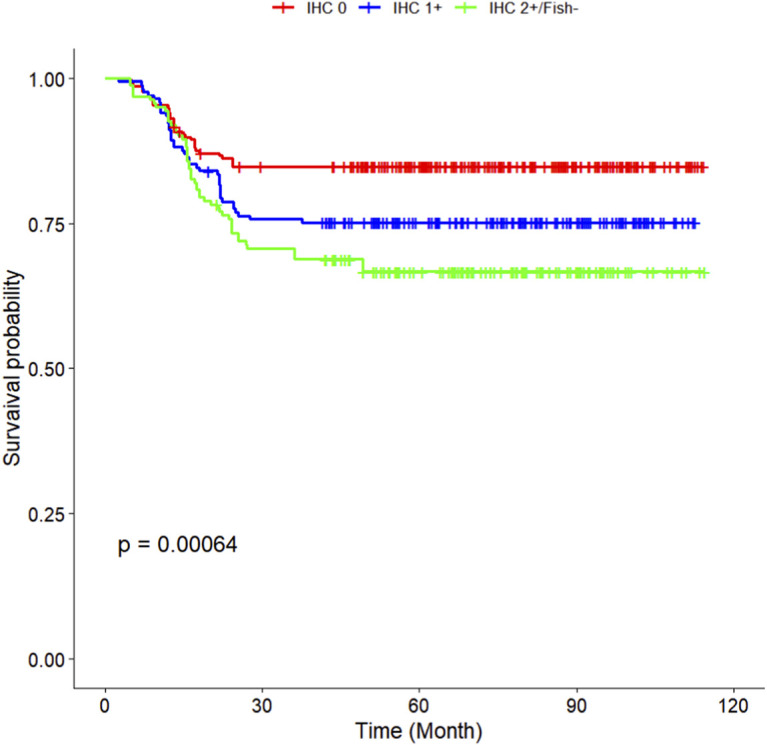 FIGURE 14
FIGURE 14| Variables | Training sets (n = 548) | Validation sets (n = 219) | P Value |
|---|---|---|---|
| Age at diagnosis | | | 0.531 |
| <50 years | 451 (82.30%) | 176 (80.37%) | |
| ≥50 years | 97 (17.70%) | 43 (19.63%) | |
| Family history | | | 0.020 |
| No | 469 (85.58%) | 201 (91.78%) | |
| Yes | 79 (14.42%) | 18 (8.22%) | |
| Surgical approach | | | 0.396 |
| Radical surgery | 412 (75.18%) | 171 (78.08%) | |
| Breast-conserving surgery | 136 (24.82%) | 48 (21.92%) | |
| Postoperative pathological T staging | | | <0.001 |
| T1 | 172 (31.39%) | 91 (41.55%) | |
| T2 | 264 (48.18%) | 65 (29.68%) | |
| T3+T4 | 112 (20.44%) | 63 (28.77%) | |
| Postoperative pathological N staging | | | 0.183 |
| N0 | 391 (71.35%) | 153 (69.86%) | |
| N1 | 109 (19.89%) | 47 (21.46%) | |
| N2 | 27 (4.93%) | 16 (7.31%) | |
| N3 | 21 (3.83%) | 3 (1.37%) | |
| Tumor grade | | | 0.170 |
| G1+G2 | 347 (63.32%) | 127 (57.99%) | |
| G3 | 201 (36.68%) | 92 (42.01%) | |
| Lymph-vascular invasion | | | 0.088 |
| No | 283 (51.64%) | 128 (58.45%) | |
| Yes | 265 (48.36%) | 91 (41.55%) | |
| sTIL expression levels | | | 0.427 |
| Low | 117 (21.35%) | 38 (17.35%) | |
| Intermediate | 162 (29.56%) | 71 (32.42%) | |
| High | 269 (49.09%) | 110 (50.23%) | |
| Her2 expression levels | | | 0.522 |
| IHC 0 | 218 (39.78%) | 95 (43.38%) | |
| IHC 1+ | 169 (30.84%) | 59 (26.94%) | |
| IHC 2+/Fish- | 161 (29.38%) | 65 (29.68%) | |
| Ki67 | | | 0.005 |
| Ki67 ≤ 20 | 22 (4.01%) | 20 (9.13%) | |
| Ki67 > 20 | 526 (95.99%) | 199 (90.87%) | |
| CK5/6 | | | 0.995 |
| Negative | 115 (20.99%) | 46 (21.00%) | |
| Positive | 433 (79.01%) | 173 (79.00%) | |
| EGFR | | | 0.031 |
| Negative | 91 (16.61%) | 51 (23.29%) | |
| Positive | 457 (83.39%) | 168 (76.71%) | |
| Radiation therapy status | | | 0.731 |
| No | 442 (80.66%) | 179 (81.74%) | |
| Yes | 106 (19.34%) | 40 (18.26%) | |
| Variables | Univariate analyses | Multivariate analyses | ||||
|---|---|---|---|---|---|---|
| HR | 95%CI | P | HR | 95%CI | P | |
| Age at diagnosis | ||||||
| <50 years | 1 | | | 1 | | |
| ≥50 years | 0.445 | 0.246–0.807 | 0.008 | 0.605 | 0.326–1.124 | 0.112 |
| Family history | ||||||
| No | 1 | | | — | — | — |
| Yes | 0.586 | 0.323–1.062 | 0.078 | — | — | — |
| Surgical approach | ||||||
| Radical surgery | 1 | | | — | — | — |
| Breast-conserving surgery | 0.964 | 0.644–1.445 | 0.86 | — | — | — |
| Postoperative pathological T staging | ||||||
| T1 | 1 | | | 1 | | |
| T2 | 1.6 | 0.985–2.600 | 0.058 | 1.623 | 0.969–2.719 | 0.066 |
| T3+T4 | 4.264 | 2.596–7.004 | <0.001 | 3.434 | 1.975–5.97 | <0.001 |
| Postoperative pathological N staging | ||||||
| N0 | 1 | | | 1 | | |
| N1 | 3.882 | 2.609–5.776 | <0.001 | 3.204 | 2.101–4.885 | <0.001 |
| N2 | 2.967 | 1.462–6.021 | 0.003 | 5.284 | 2.507–11.139 | <0.001 |
| N3 | 19.799 | 11.683–33.554 | <0.001 | 7.587 | 4.381–13.14 | <0.001 |
| Tumor grade | ||||||
| G1+G2 | 1 | | | 1 | | |
| G3 | 2.242 | 1.583–3.176 | <0.001 | 1.341 | 0.923–1.948 | 0.123 |
| Lymph-vascular invasion | ||||||
| No | 1 | | | — | — | — |
| Yes | 1 | 0.707–1.414 | 1 | — | — | — |
| sTIL expression levels | ||||||
| Low | 1 | | | 1 | | |
| Intermediate | 0.494 | 0.344–0.710 | <0.001 | 0.408 | 0.275–0.604 | <0.001 |
| High | 0.041 | 0.021–0.083 | <0.001 | 0.044 | 0.021–0.091 | <0.001 |
| Her2 expression levels | ||||||
| IHC 0 | 1 | | | 1 | | |
| IHC 1+ | 1.695 | 1.074–2.674 | 0.023 | 1.177 | 0.734–1.887 | 0.499 |
| IHC 2+/Fish- | 2.298 | 1.488–3.549 | <0.001 | 2.392 | 1.513–3.782 | <0.001 |
| Ki67 | ||||||
| Ki67 ≤ 20 | 1 | | | 1 | | |
| Ki67 > 20 | 0.326 | 0.184–0.579 | <0.001 | 0.759 | 0.384–1.498 | 0.426 |
| CK5/6 | ||||||
| Negative | 1 | | | — | — | — |
| Positive | 0.813 | 0.543–1.219 | 0.317 | — | — | — |
| EGFR | ||||||
| Negative | 1 | | | — | — | — |
| Positive | 1.088 | 0.675–1.754 | 0.729 | — | — | — |
| Radiation therapy status | ||||||
| No | 1 | | | — | — | — |
| Yes | 1.004 | 0.648–1.554 | 0.987 | — | — | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · HER2/EGFR in Cancer Research · Advanced Breast Cancer Therapies
Introduction
1
Breast cancer remains the most commonly diagnosed malignancy and the leading cause of cancer-related mortality among women worldwide (Bray et al., 2024). Triple-negative breast cancer (TNBC), characterized by the absence of estrogen receptor, progesterone receptor, and HER2 amplification, represents a particularly aggressive subtype with limited therapeutic options and a heightened propensity for early recurrence (Bianchini et al., 2016; Foulkes et al., 2010). Within this heterogeneous disease, premenopausal patients often exhibit distinct clinicopathological and molecular features, including enriched immunogenic signatures and homologous recombination deficiency, which may influence both tumour behaviour and therapeutic response (Azim et al., 2012; Bareche et al., 2018).
Anthracycline and taxane-based chemotherapy remains the cornerstone of adjuvant treatment for early-stage TNBC (Liedtke et al., 2008). However, intrinsic and acquired chemoresistance significantly undermines its efficacy, leading to disparate clinical outcomes (Gonzalez-Angulo et al., 2011; Wahba and El-Hadaad, 2015). The mechanisms underlying chemoresistance are multifactorial, encompassing tumour-intrinsic factors such as apoptotic evasion, enhanced DNA damage repair, and cancer stem cell persistence, as well as microenvironmental influences including immune contexture and stromal composition (Holohan et al., 2013; Shibue and Weinberg, 2017; Gottesman, 2002).
Emerging evidence underscores the prognostic significance of stromal tumour-infiltrating lymphocytes (sTILs) in TNBC, where higher densities correlate with improved pathological complete response and survival following chemotherapy (M Geurts et al., 2024; Salgado et al., 2015). Concurrently, The biological and clinical significance of HER2-low breast cancer, defined as immunohistochemistry (IHC) 1+ or IHC 2+ with negative in situ hybridization (FISH), has recently come into focus. Supported by evidence from clinical trials of novel anti-HER2 antibody–drug conjugates, this subset has emerged as a therapeutically actionable entity (Saura et al., 2025; Modi et al., 2025). Growing preliminary evidence further suggests that HER2-low tumours may represent a distinct biological subtype with unique therapeutic vulnerabilities (Tarantino et al., 2020; Agostinetto et al., 2021). Recent studies, including those by Tarantino P and Schettini F et al., have begun to delineate the underlying biology of HER2-low breast cancer across subtypes, including triple-negative breast cancer (Tarantino et al., 2023; Schettini et al., 2025).
Despite these advances, validated biomarkers for stratifying chemosensitivity in premenopausal TNBC remain scarce. Most existing prognostic tools neither account for the unique biology of this demographic nor integrate readily accessible biomarkers reflective of tumour-immune interplay (Sparano et al., 2018; Parker et al., 2009). Therefore, we aimed to develop and validate a clinically applicable nomogram that incorporates key clinicopathological and microenvironmental variables-specifically sTIL density and HER2-low status-to predict disease-free survival (DFS) in premenopausal women with TNBC treated with anthracycline-taxane chemotherapy.
Methods
2
Study design and patient cohort
2.1
This retrospective, multicentre cohort study consecutively enrolled 767 female patients with TNBC from Peking Union Medical College Hospital and Lishui People’s Hospital of Zhejiang Province between 1 Jan 2016, and 31 Dec 2021 (Figure 1).
Patient selection flowchart for this study.
Inclusion Criteria: (1) Histopathologically confirmed invasive breast carcinoma; (2) Negative for estrogen receptor, progesterone receptor, and HER2 (defined as ER/PR <1% positive cells, HER2 IHC 0 or 1+, or 2+ with negative FISH); (3) Premenopausal status at diagnosis; (4) Underwent curative-intent surgery (modified radical mastectomy or breast-conserving surgery) at initial diagnosis; (5) Received adjuvant chemotherapy based on anthracyclines and taxanes (sequential or combination regimens) postoperatively; (6) Had complete clinical, pathological, and follow-up data.
Exclusion Criteria: (1) Bilateral breast cancer or concurrent other malignancies; (2) History of neoadjuvant chemotherapy; (3) Presence of distant metastasis at diagnosis; (4) Incomplete follow-up data.
Variable definition and data collection
2.2
Collected variables included: age at diagnosis, family history of breast cancer, surgical approach, postoperative pathological T staging, postoperative pathological N staging, tumor grade, lymph-vascular invasion, sTIL expression levels, Her2 expression levels, Ki-67 index, CK5/6 expression, EGFR expression, and receipt of radiotherapy.
HER2 Status Assessment: HER2 protein expression was evaluated by IHC, and equivocal cases (IHC 2+) were reflexively tested by FISH according to the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines (Wolff et al., 2023). To ensure consistency and mitigate inter-institutional variability-a known challenge in HER2-low scoring—all IHC and FISH results underwent a centralized review by two experienced breast pathologists who were blinded to patient outcomes. HER2-low status was defined according to the standard definition as IHC 1+ or IHC 2+/FISH-negative. For primary and sensitivity analyses, patients were categorized into three groups: HER2 IHC 0, HER2 IHC 1+, and HER2 IHC 2+/FISH-negative.
sTIL Assessment: sTILs were evaluated by two experienced pathologists blinded to clinical outcomes, according to international guidelines. sTILs were defined as the percentage of tumour stroma area occupied by mononuclear inflammatory cells (lymphocytes and plasma cells). sTIL density was categorised into three groups: low (≤10%), intermediate (10%–40%), and high (>40%).
Follow-up strategy
2.3
Follow-up started from the date of initial breast cancer diagnosis and ended on 1 June 2025. Follow-up methods included outpatient visits and telephone interviews. Data collected encompassed: local or regional recurrence, distant metastasis, time to first recurrence or metastasis, site of first recurrence or metastasis, and vital status at the last follow-up.
Disease-free survival (DFS) was defined as the time from surgery date to the first occurrence of any of the following events: local recurrence, regional recurrence, distant metastasis, contralateral breast cancer, or death from any cause.
Statistical analysis
2.4
Analyses were performed using R software (version 4.3.1). The patient cohort was randomly split into a training set (70%) and an internal validation set (30%). Categorical variables are presented as numbers (percentages) and compared using the χ^2^ test or Fisher’s exact test. Continuous variables are presented as mean ± standard deviation or median (interquartile range) based on their distribution and compared using the t-test or Mann-Whitney U test.
In the training set, univariable Cox regression analysis (P < 0.05) was used to screen prognostic factors associated with DFS. Significant variables were subsequently included in a multivariable Cox proportional hazards regression model to identify independent prognostic factors. Results are presented as hazard ratios (HRs) with 95% confidence intervals (CIs).
Based on the final independent prognostic factors, a nomogram for predicting 1-year, 3-year, and 5-year DFS probabilities was constructed using the rms package. The model’s discrimination was assessed using the C-index and time-dependent AUC analysis. Calibration curves were plotted to evaluate the agreement between predicted probabilities and observed outcomes (assessed by the Kaplan-Meier method). For key prognostic variables, Kaplan-Meier survival curves were generated, and differences between groups were compared using the log-rank test.
All tests were two-sided, and a P value <0.05 was considered statistically significant.
Results
3
Patient characteristics and follow-up
3.1
The final cohort comprised 767 premenopausal TNBC patients with a median follow-up of 76.0 months. The median age was 49.0 years. The cohort was randomly divided into training (n = 548) and internal validation (n = 219) sets. Baseline clinicopathological characteristics were largely balanced between the training and validation sets, except for family history, postoperative pathological T staging, Ki-67 index, and EGFR status (all P < 0.05, Table 1). All other variables showed no significant differences (all P > 0.05, Table 1). In the training set, 420 DFS events and 128 deaths were recorded over a median follow-up of 73.7 months; the validation set experienced 170 DFS events and 49 deaths over 75.4 months.
Prognostic nomogram for disease-free survival
3.2
The multivariate Cox regression revealed that postoperative pathological T staging (T3+T4,HR = 3.434,95%CI:1.975-5.97,P < 0.001), postoperative pathological N staging (N1,HR = 3.204,95%CI:2.101-4.885,P < 0.001; N2,HR = 5.284,95%CI:2.507-11.139,P < 0.001; N3,HR = 7.587,95%CI:4.381-13.14,P < 0.001),sTIL expression levels (sTIL intermediate expression, HR = 0.408, 95% CI: 0.275-0.604,P < 0.001; sTIL high expression, HR = 0.044, 95% CI: 0.021-0.091,P < 0.001), and Her2 expression levels (IHC 2+/Fish-, HR = 2.392, 95% CI: 1.513-3.782,P < 0.001) were independent predictive factors for DFS in premenopausal TNBC patients (Table 2). A nomogram integrating these variables was constructed to estimate 1-, 3-, and 5-year DFS probabilities (Figure 2). The model exhibited excellent discrimination, with C-indices of 0.862 (training) and 0.861 (validation). Time-dependent receiver operating characteristic (ROC) analysis further confirmed its robust predictive accuracy, with area under the curve (AUC) values for 3-year DFS of 0.907 and 0.908 in the training and validation sets, respectively (Figures 3, 4). Calibration curves demonstrated close alignment between predicted and observed outcomes across all time points (Figures 5–10). Kaplan-Meier analyses visually affirmed the prognostic stratification afforded by each variable (Figures 11–14).
Prognostic nomogram for predicting disease-free survival time of premenopausal TNBC patients.
Roc curve of the training set.
Roc curve of the validation set.
Calibration curve of the training set at 1 Year.
Calibration curve of the training set at 3 Years.
Calibration curve of the training set at 5 Years.
Calibration curve of the validation set at 1 Years.
Calibration curve of the validation set at 3 Years.
Calibration curve of the validation set at 5 Years.
KM curves stratified by T staging in the Training Set.
KM curves stratified by N staging in the Training Set.
KM curves stratified by sTIL expression levels in the Training Set.
KM curves stratified by Her2 expression levels in the Training Set.
Discussion
4
In this large, multicentre retrospective study, we developed and validated a prognostic nomogram specifically tailored for premenopausal women with TNBC receiving anthracycline–taxane chemotherapy. The model-incorporating T stage, N stage, sTIL density, and HER2 immunohistochemistry (IHC) status-demonstrated high predictive accuracy and clinical utility, addressing a critical unmet need in this high-risk population.
Our findings confirm the prognostic relevance of the tumour immune microenvironment in this cohort. Low sTIL density was independently associated with worse disease-free survival, corroborating previous studies that have consistently linked lower sTIL levels with inferior outcomes in patients treated with DNA-damaging chemotherapies (M Geurts et al., 2024; Denkert et al., 2018; Adams et al., 2019). Clinically, these results align with the concept that tumours with low sTILs frequently exhibit an immunologically “cold” phenotype, which may inform future therapeutic strategies aimed at enhancing antitumour immunity in such patients (Sharma et al., 2017; Emens and Middleton, 2015).
We also observed that HER2 IHC 2+/fluorescence in situ hybridization (FISH)-negative status—but not IHC 1+—independently predicted poorer disease-free survival, challenging several earlier reports that associated HER2-zero expression with inferior outcomes in TNBC (Miglietta et al., 2025; Won and Spruck, 2020). This discrepancy may reflect variations in patient selection, treatment setting, or HER2 scoring methodology. Multivariable analysis under the standard HER2-low definition (IHC 1+ or IHC 2+/FISH-negative) indicated that the prognostic risk was predominantly driven by the IHC 2+/FISH-negative subgroup. This suggests that HER2-low TNBC may not represent a homogeneous entity and that IHC 2+/FISH-negative tumours could harbour distinct biological properties—a hypothesis that warrants further validation.
Growing preclinical and clinical evidence indicates that HER2-low breast cancers exhibit altered receptor trafficking, activation of compensatory signalling pathways (e.g., PI3K/AKT, MAPK), and specific tumour–stroma interactions, which may collectively compromise chemotherapy efficacy (Tarantino et al., 2020; Schettini et al., 2021; Modi et al., 2022). Translationaly, the recent efficacy of novel antibody–drug conjugates such as trastuzumab deruxtecan in HER2-low metastatic breast cancer underscores the clinical relevance of this subset and highlights its potential susceptibility to targeted approaches (Banerji et al., 2019; Gennari et al., 2021). Our data suggest that premenopausal patients with HER2-low TNBC—particularly those with IHC 2+/FISH-negative disease—represent a candidate population for adjuvant antibody–drug conjugate trials. Such a strategy could eventually shift the therapeutic paradigm from empirical chemotherapy toward biomarker-guided targeted treatment.
Moreover, TNBC is a molecularly heterogeneous disease, encompassing distinct subtypes such as those described by Lehmann BD et al. (basal-like, immunomodulatory, mesenchymal, etc.) (Lehmann et al., 2011). The prognostic role of sTILs and HER2-low status may vary across these subtypes, a nuance not captured in our retrospective analysis. Future prospective studies integrating transcriptomic subtyping with tumour microenvironment features are warranted to refine personalised prognostic models.
By restricting our analysis to premenopausal women, we minimised confounding from age-related biological differences, such as the higher prevalence of PIK3CA mutations in older patients (Ciriello et al., 2015; Cancer Genome Atlas Network, 2012). This enhances the biological coherence and clinical applicability of our model for this specific demographic. The nomogram’s performance (C-index >0.86) surpasses that of many conventional prognostic tools and genomic assays (Paik et al., 2004; Cardoso et al., 2019), supporting its utility in routine practice for risk-adapted therapeutic decision-making.
From a translational perspective, our model provides a rationale for personalised adjuvant strategies. High-risk patients-those with low sTILs and HER2-low tumours-may benefit from treatment intensification, including capecitabine maintenance (Wang et al., 2021; Masuda et al., 2017) or PARP inhibition in BRCA-mutated cases (J Tutt et al., 2021; Robson et al., 2017). Conversely, low-risk patients could be spared unnecessary toxicity. Furthermore, this tool may facilitate refined patient selection for clinical trials evaluating immunomodulatory agents or novel antibody–drug conjugates in the early-stage setting.
Limitations
5
Several limitations of our study warrant consideration. First, its retrospective design introduces potential selection bias, despite multicentre enrolment. Second, all participants were of Chinese ancestry; external validation in diverse ethnic and geographic populations is essential to confirm generalisability (Eniu et al., 2008). Third, although patients were randomly assigned to training and validation sets, some baseline variables (e.g., family history, postoperative pathological T staging, Ki-67 index, and EGFR status) showed uneven distributions. While our model maintained high predictive performance across cohorts, such imbalances could theoretically introduce selection bias or affect generalizability. Future validation in larger, multi-ethnic cohorts is warranted to confirm the model’s stability. Fourth, although HER2 and sTIL assessments followed international guidelines and underwent central review, HER2 scoring reproducibility remains a challenge in TNBC, and sTIL evaluation is semi-quantitative. Future iterations could benefit from digital pathology, automated image analysis, or standardized immune-based assays to improve objectivity and reproducibility (Klauschen et al., 2018; Vanguri et al., 2022). Fifth, we did not incorporate germline BRCA status, a known determinant of TNBC prognosis and treatment response (Tutt et al., 2010; Tung et al., 2020). Integrating genomic and transcriptomic data in future prospective studies may further refine predictive accuracy and biological insight (Curtis et al., 2012; Pereira et al., 2016).
Conclusion
6
In conclusion, we have identified and validated low stromal TILs and HER2-low status as key biomarkers of intrinsic resistance to anthracycline-taxane chemotherapy in premenopausal TNBC. Beyond prognostication, these factors illuminate distinct biological pathways underlying treatment failure-an immunosuppressive microenvironment and the unique biology of HER2-low tumors. This mechanistic insight provides a compelling rationale for future pharmacological strategies: leveraging immunotherapy to inflame sTIL-low tumors and deploying novel ADCs to target HER2-low subtypes. Our findings thus offer a practical framework for patient stratification and pave the way for more personalized, mechanism-driven adjuvant therapy trials in this challenging disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adams S. Gatti-Mays M. E. Kalinsky K. Korde L. A. Sharon E. Amiri-Kordestani L. (2019). Current landscape of immunotherapy in breast cancer: a review. JAMA Oncol. 5 (8), 1205–1214. 10.1001/jamaoncol.2018.7147 30973611 PMC 8452050 · doi ↗ · pubmed ↗
- 2Agostinetto E. Rediti M. Fimereli D. Debien V. Piccart M. Aftimos P. (2021). HER 2-Low breast cancer: molecular characteristics and prognosis. Cancers (Basel) 13 (11), 2824. 10.3390/cancers 13112824 34198891 PMC 8201345 · doi ↗ · pubmed ↗
- 3Azim Jr H. A. Michiels S. Bedard P. L. Singhal S. K. Criscitiello C. Ignatiadis M. (2012). Elucidating prognosis and biology of breast cancer arising in young women using gene expression profiling. Clin. Cancer Res. 18 (5), 1341–1351. 10.1158/1078-0432.CCR-11-2599 22261811 · doi ↗ · pubmed ↗
- 4Banerji U. Van Herpen C. M. L. Saura C. Thistlethwaite F. Lord S. Moreno V. (2019). Trastuzumab duocarmazine in locally advanced and metastatic solid tumours and HER 2-expressing breast cancer: a phase 1 dose-escalation and dose-expansion study. Lancet Oncol. 20 (8), 1124–1135. 10.1016/S 1470-2045(19)30328-6 31257177 · doi ↗ · pubmed ↗
- 5Bareche Y. Venet D. Ignatiadis M. Aftimos P. Piccart M. Rothe F. (2018). Unravelling triple-negative breast cancer molecular heterogeneity using an integrative multiomic analysis. Ann. Oncol. 29 (4), 895–902. 10.1093/annonc/mdy 024 29365031 PMC 5913636 · doi ↗ · pubmed ↗
- 6Bianchini G. Balko J. M. Mayer I. A. Sanders M. E. Gianni L. (2016). Triple-negative breast cancer: challenges and opportunities of a heterogeneous disease. Nat. Rev. Clin. Oncol. 13 (11), 674–690. 10.1038/nrclinonc.2016.66 27184417 PMC 5461122 · doi ↗ · pubmed ↗
- 7Bray F. Laversanne M. Sung H. Ferlay J. Siegel R. L. Soerjomataram I. (2024). Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 74 (3), 229–263. 10.3322/caac.21834 38572751 · doi ↗ · pubmed ↗
- 8Cancer Genome Atlas Network (2012). Comprehensive molecular portraits of human breast tumours. Nature 490 (7418), 61–70. 10.1038/nature 11412 23000897 PMC 3465532 · doi ↗ · pubmed ↗