Research progress on the correlation between blood pressure variability and hypertensive microvascular disease
Shifeng Chen, Hongyu Kuang, Jie Zhu, Jia Wei, Pei Pan, Xinyu Hu, Ke Yang, Xiaoshu Yi, Huaan Du

TL;DR
This paper reviews how blood pressure variability contributes to microvascular damage in hypertension, independent of average blood pressure.
Contribution
The paper systematically explores BPV's role as an independent risk factor for hypertensive microvascular disease.
Findings
BPV is an independent risk factor for endothelial injury and target organ damage.
Neurohumoral regulation, behavioral factors, and comorbidities influence BPV.
BPV is closely linked to microvascular complications in diabetic and obese populations.
Abstract
The hypertensive microvascular disorder is a significant complication that can lead to substantial target organ damages, including cognitive impairments, visual impairments, and deterioration in renal function. Recent studies have indicated that blood pressure variability (BPV) is an independent risk factor for the progression of this pathology. The present paper aims to systematically elucidate the concept, classification, and clinical significance of BPV, focusing on how it acts as a pathogenic mechanism independent of mean blood pressure to exacerbate endothelial injury and cause target organ damage. This review was conducted to evaluate the influences of multiple factors on BPV, including neurohumoral regulation, the behavioural environment and comorbidities. It also emphasises the intrinsic link between BPV and microvascular complication risk in specific populations, such as those…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
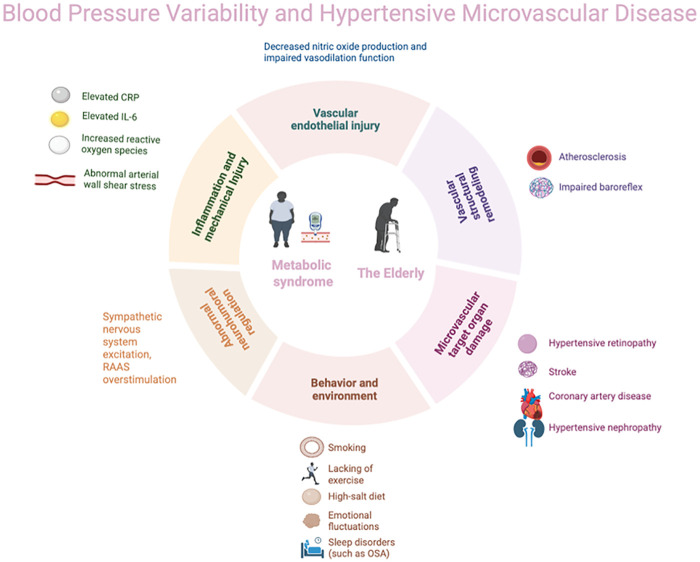 Figure 1
Figure 1| Type of BPV | time scale | Monitoring methodology | Representative indicators | Physiological/pathological significance | Clinical association | Advantages/limitations |
|---|---|---|---|---|---|---|
| Ultra-short-term BPV | beat to beat | Invasive intra-arterial monitoring, Non-invasive photoplethysmography, pulse transit time, tonometry | Linear: SD, CV, ARV, VIM, RSD, SV | Reflects instantaneous changes in the cardiovascular autonomic nervous system and is highly correlated with baroreflex sensitivity | Characteristic analysis in hypertensive populations; predicts white matter lesions, recurrent stroke, cardiovascular events; perioperative risk assessment for cardiac surgery; evaluation of volume responsiveness in critically ill patients | Advantage: Captures real-time autonomic nervous system information, reflecting early pathological changes. Limitation: Subject to equipment and environmental constraints; operation is complex; not yet widely adopted in clinical practice |
| Nonlinear: measure of entropy, DFA | ||||||
| Short-term BPV | in 24 h/day/night | ABPM | 24-hour/daytime/nighttime SD, CV, ARV, VIM, nocturnal blood pressure drop, morning peak blood pressure, etc | Reflects the impact of circadian rhythm, behavioral activities, and sleep patterns on blood pressure, demonstrating short-term vascular regulatory capacity | Independently predicts risk of coronary heart disease, stroke, and cardiovascular mortality; used in evaluate antihypertensive treatment efficacy | Advantage: Relatively high degree of standardization; most widely used in clinical practice; evidence is relatively robust |
| Limitation: Only reflects single-day blood pressure variation; heavily influenced by sleep and physical activity | ||||||
| Medium-term BPV | day to day | OBPM/HBPM | SD, CV, ARV, VIM, etc | Reflects blood pressure stability over longer periods, influenced by treatment adherence and lifestyle fluctuations | Predict cardiovascular mortality risk | Advantage: Data easily obtained (based on routine follow-up), low cost. Limitation: Susceptible to “white-coat effect” and inconsistent measurement conditions |
| Long-term BPV | visit to visit | Office, home, or ABPM data from long-term follow-up | SD, CV, ARV, VIM, etc | Reflects long-term trends and chronic instability of blood pressure, associated with progressive vascular remodeling and target organ damage | Predicts stroke, cognitive impairment, renal progression; predict mortality risk in CVD patients; assesses adherence, aids medication decisions | Advantage: Capable of capturing blood pressure fluctuation patterns most relevant to chronic damage |
| Limitation: Requires very long-term data; analysis is complex; many confounding factors |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Cardiovascular Health and Risk Factors · Sodium Intake and Health
Introduction
1
Hypertension is one of the most prevalent chronic cardiovascular diseases globally. An epidemiological research suggests that approximately 1.4 billion adults worldwide will be living with hypertension by 2024. However, it is estimated that less than one-fifth of these individuals will achieve adequate control of their condition. This phenomenon has been shown to result in a significant health and economic burden, particularly severe in developing countries (1). It is well established that persistent elevated arterial blood pressure can result in damage to multiple target organs, including but not limited to the heart, brain, and kidneys. This has a considerable impact on quality of life and increases healthcare costs, making effective blood pressure control crucial for mitigating target organ damage and improving prognosis. It is widely accepted that microvasculature represents a key target organ for damage caused by hypertension. This term refers to a number of different organs and arteries, including those located within the brain (intracranial arterioles), the eye (retinal arteries), the kidneys (glomerular arterioles), and the heart (coronary arteries). Early microvascular injury is characterised by its subtlety and difficulty in detection, with a progressive deterioration that accompanies disease progression. This contributes to a range of serious conditions, including stroke, cognitive impairment, visual impairment, coronary atherosclerotic heart disease, and renal insufficiency. At present, there is no universally accepted standard for the detection of microvascular lesions, thus highlighting the necessity for further exploration of innovative diagnostic approaches.
Blood pressure variability (BPV) is a term used to describe a series of indicators reflecting fluctuations in systolic or diastolic pressure. Notwithstanding mean blood pressure levels, BPV evinces a marked association with cardiovascular incidents (2). The key indicators for assessing BPV include standard deviation (SD), coefficient of variation (CV), average real variance (ARV), and variance independent of mean (VIM). Despite the differing calculation methods, elevated values across these metrics generally indicate increased blood pressure fluctuations. BPV is recognised as an independent risk factor for microvascular complications in hypertension and has a promoting effect on microvascular target organ damage (3–6). Maintaining BPV stability may therefore be crucial. To date, no study has systematically elucidated the role of BPV in microvascular complications across different hypertensive populations or its underlying mechanisms. The present review explores the correlation between BPV and microvascular complications, and investigates potential mechanisms.
An overview of BPV
2
The definition and classification of BPV
2.1
BPV is defined as the degree of blood pressure fluctuation exhibited by an individual over a specific time period. This fluctuation is indicative of the body's ability to regulate blood pressure in response to internal and external environmental changes, as well as the integrity of cardiovascular autonomic nervous system regulation. While healthy individuals also experience a certain range of blood pressure fluctuations during daily activities, the amplitude of these fluctuations is minimal and remains within a controllable range. However, in cases where the body is in a diseased state, such as hypertension, atherosclerosis, or diabetes, there is often an accompanying autonomic dysfunction and a decline in the function of vascular pressure receptors. This directly leads to a decline in the body's ability to regulate blood pressure both instantaneously and over the short term, resulting in an abnormal increase in BPV (7–9). Consequently, BPV abnormalities are fundamentally the combined result of autonomic nervous system dysfunction and impaired baroreceptor reflexes. Clinically, BPV can be categorized based on the time span of blood pressure monitoring into ultra-short-term BPV (beat to beat), short-term BPV (within 24 h), medium-term BPV (within several days), and long-term BPV (spanning weeks, seasons, or even years) (10). Short-term BPV refers to blood pressure fluctuations over 24 h, as assessed by ambulatory blood pressure monitoring (ABPM). This includes daytime BPV, nocturnal BPV and the morning blood pressure surge, which is the most clinically prevalent form (11). Medium- and long-term BPV reflect blood pressure changes over a period of days to years and are usually associated with BPV between follow-up visits. These exhibit independent predictive value for events such as myocardial infarction, stroke, and cardiovascular mortality (12–14). Ultra-short-term BPV (beat-to-beat) represents blood pressure fluctuations between consecutive heartbeats and can be obtained via invasive arterial monitoring or non-invasive devices (15, 16). It is recognised as an independent predictor of white matter lesions, recurrent stroke and cardiovascular events (17, 18), and is valuable in assessing fluid responsiveness in mechanically ventilated intensive care patients (19) (Table 1).
Multiple factors greatly influencing BPV
2.2
The current body of research indicates that BPV is primarily influenced by multiple factors, including the regulation of the autonomic and humoral systems is of particular interest in this study. The autonomic nervous system plays a dominant role in maintaining blood pressure stability, with the dynamic balance between sympathetic and parasympathetic activity determining BPV levels (20). Dysfunction of this system, such as cardiovascular autonomic neuropathy associated with diabetes, has been demonstrated to significantly reduce baroreflex sensitivity and lead to elevated blood pressure (21). Furthermore, the circadian secretion patterns of endocrine hormones such as aldosterone, cortisol, and thyroid hormones have been identified as significant contributors to abnormal BPV (22). Secondly, the behavioural and environmental factors must be considered. Numerous elements of daily life have been demonstrated to exert an influence on BPV, including emotional fluctuations, sleep quality, seasonal changes, dietary patterns, and exercise habits (23–28). Thirdly, consideration must be given to the combined effects of medications and other diseases. The types and combinations of antihypertensive medications are significant factors influencing BPV (29). Furthermore, the omorbid conditions of patients are also significant contributors to BPV fluctuations, particularly in the diabetic population, where obesity, kidney disease, and sleep-disordered breathing often coexist (30–32). The presence of these comorbid states has been demonstrated to exacerbate BPV abnormalities.
Pathophysiological mechanisms of BPV-induced endothelial dysfunction and microvascular injury
2.3
Research indicates that BPV contributes to vascular endothelial injury and microvascular lesions via multiple pathophysiological mechanisms. These include: 1. Abnormal blood flow shear stress. Increased BPV causes abrupt and recurrent changes in blood flow velocity and direction, generating turbulent and oscillatory shear stress. This directly damages vascular endothelial cells, leading to reduced nitric oxide (NO) bioavailability and promoting reactive oxygen species (ROS) production. It also activates inflammatory pathways such as nuclear factor kappaB (NF-κB) (33, 34). 2. Vascular remodelling: Persistent abnormal mechanical stress stimulates the proliferation, migration of vascular smooth muscle cells and extracellular matrix deposition. This leads to arterial wall thickening and luminal narrowing (35). 3. Promotion of thrombogenesis: Under conditions of high shear stress, endothelial injury exposes subendothelial collagen, which triggers von Willebrand factor (vWF)-mediated platelet activation and promotes microthrombus formation (36).
BPV also acting as an independent risk factor for hypertensive microvascular complications
3
Hypertensive retinopathy
3.1
Hypertensive retinopathy (HR) is a prevalent microvascular complication of hypertension, manifesting as lesions in various locations, including the retina, choroid, and optic nerve. A multicentre cross-sectional study involving 696 adult hypertensive patients revealed an overall prevalence of HR reaching 57.47% (95% CI: 53.75–61.10) (37). Conventionally, the progression of hypertension has been closely associated with the extent of blood pressure elevation. In the early stages of elevated blood pressure, functional compensatory adjustments occur in retinal arterioles, leading to diffuse stenosis. This progresses structurally over time, manifesting as retinal arteriolar wall thickening and hyalinization, ultimately compromising the blood-retinal barrier and precipitating HR (38). In recent years, the role of BPV in HR development has garnered increasing attention from the academic community, though current research conclusions remain inconclusive. A substantial body of research has indicated a positive correlation between BPV and HR. Previous studies also evaluated the association between BPV metrics and retinal microvascular structural degeneration in hypertensive patients (39). These findings demonstrated a negative correlation between SD of 24-hour diastolic blood pressure and retinal nerve fibre layer thickness (β = −0.707, p = 0.002). In addition, it was found that systolic blood pressure average real variability(ARV) was negatively correlated with vessel density (VD) (β = −0.259, p = 0.001) and perfusion density (PD) (β = −0.006, p = 0.001). Then, Lou et al. (40) demonstrated in a diabetic cohort that elevated systolic BPV and systolic BP > 130 mmHg were both independent risk factors for retinopathy. In a large-scale study enrolling patients with type 1 diabetes, Fatulla et al. (41) identified inter-visit systolic blood pressure variability (SBPV) as an independent predictor of retinopathy. Meanwhile, the highest quartile of inter-visit SBP variability was significantly demonstrated to be associated with a 17% increased risk of new-onset retinopathy (OR = 1.171, 95% CI: 1.129–1.214, p < 0.001) (42). However, a number of well-designed, large-scale studies have failed to replicate these findings, and in some cases have even reported clear negative results. Foo et al. (43) found in an Asian type 2 diabetic cohort that factors associated with moderate retinopathy included mean glycated hemoglobin (HbA1c) levels and mean systolic blood pressure, but not BPV. Cardoso et al. (44) proposed that BPV is a predictor of major adverse cardiovascular events; however, they also found that it is unrelated to various microvascular outcomes, including retinopathy. This discrepancy may be attributable to two factors. Firstly, the underlying disease types of the study populations. Positive results predominantly emerged in primary hypertension cohorts, while negative findings were common in type 2 diabetes populations due to strong interference from multiple metabolic factors, such as hyperglycaemia. Secondly, a considerable degree of heterogeneity exists among the studies in terms of the assessment metrics for BPV, temporal scales, and diagnostic criteria for retinopathy, which complicates the direct comparison of results. In summary, the current evidence remains insufficient to establish a universally applicable causal relationship between BPV and retinopathy. In order to achieve further validation, it is necessary to conduct future large-scale prospective studies employing standardised assessment systems across stratified populations.
Coronary heart disease
3.2
Coronary heart disease (CHD) has been identified as the primary cause of cardiac death among hypertensive patients. Concurrently, BPV is considered a potential independent risk factor for the onset and progression of CHD (12, 45, 46). D. Clark et al. (12) established a correlation between long-term systolic blood pressure (SBP) and the progression of coronary atherosclerotic plaques (OR = 1.09, 95% CI: 1.02–1.17, p = 0.02). Moreover, the relationship between BPV and mortality was analyzed, indicating that patients in the highest quintile of BPV over a one-year period exhibited a significantly elevated long-term mortality risk in comparison to those with the lowest BPV (45). It remained consistent across different methods of measuring systolic BPV, with the strongest association observed when expressed as ARV (aHR = 1.18, 95% CI: 1.08–1.30). As demonstrated by Sun PF et al. (46), a U-shaped relationship between short-term 24-hour systolic BPV and one-year mortality in CHD patients (p = 0.001), while diastolic BPV showed a positive correlation (HR = 1.03, 95% CI: 1.00–1.06). Consequently, elevated BPV—whether short-term or long-term—is associated with adverse outcomes in CHD patients, with systolic BP demonstrating a stronger correlation. Furthermore, data from the ACSOT-BPLA trial indicate that antihypertensive regimens including amlodipine may improve BPV and potentially reduce the risk of stroke, coronary events, and cardiovascular mortality (29, 47). The potential benefits of this phenomenon may be attributable to drug-induced peripheral vasodilation, altered arterial compliance, and reduced circulatory load. It is evident that coronary plaque rupture and thrombosis are significant contributors to the progression of CHD. Therefore, the reduction of BPV in hypertensive patients has the potential to decrease vascular shear stress and suppress inflammatory mediators, such as C-reactive protein. This, in turn, has been demonstrated to reduce subendothelial lipid deposition, thereby slowing atherosclerosis progression and decreasing adverse cardiovascular events (4).
Stroke
3.3
A substantial body of epidemiological research has indicated that as many as 73.91% of stroke patients also have hypertension (48). Stroke represents the primary cause of cognitive impairment, disability, or death among hypertensive patients. Furthermore, BPV has been found to be closely associated with the occurrence and progression of stroke, as well as with white matter ischemic damage and cognitive impairment (49). Research findings indicate a robust pathophysiological association between BPV and cerebral microvascular injury. Abnormal BPV has been demonstrated to induce significant fluctuations in blood pressure, directly contributing to the occurrence of arterial ruptures or occlusions, and consequently leading to the manifestation of stroke (5). Conversely, elevated BPV has been shown to augment shear stress on vascular walls, a process that may result in microvascular dysregulation and arterial remodelling through the infliction of direct damage to endothelial cells (50). Concurrently, abnormal vascular wall shear stress has been demonstrated to further expose subendothelial collagen and trigger vWF-mediated platelet activation, thereby promoting thrombosis (36). Research indicates that short-term BPV elevation is a potent stroke trigger, such as morning blood pressure surge (MBPS), which has been associated with stroke risk in patients with Big Dipper hypertension (aHR = 1.14, 95% CI: 1.00–1.30) (51). Heshmatollah et al. (13) conducted a prospective analysis of 9,958 stroke-free subjects, revealing that long-term BPV is closely associated with stroke occurrence, with systolic BPV showing the strongest correlation with haemorrhagic stroke (HR = 1.27, 95% CI: 1.05–1.54). Furthermore, persistent BPV abnormalities have been found to correlate with white matter ischemic lesions, cognitive decline, and widespread structural alterations in cerebral white matter (52, 53). Consequently, BPV has been demonstrated to play a pivotal role in both chronic cerebrovascular injury and acute stroke events. It is evident that substantial fluctuations in blood pressure have the capacity to induce arterial rupture in a direct manner. Moreover, heightened vascular wall shear stress has been observed to result in endothelial injury and the promotion of thrombosis. Improving BPV in hypertensive patients may therefore hold clinical value for preventing microvascular brain injury.
Hypertensive renal disease
3.4
Hypertensive renal disease (HRD) is a prevalent form of chronic kidney disease (CKD) and a principal cause of end-stage renal disease (ESRD) (54). The demographic shift towards an ageing population, coupled with the escalating prevalence of hypertension, portends a relentless rise in the incidence and mortality rates of HRD. This augurs well for the challenges that kidney disease prevention and management face. Patients with HRD frequently exhibit elevated blood pressure levels, and the onset and progression of this condition is often attributed to inadequate blood pressure control. Nevertheless, this standpoint has been contested by the principles of evidence-based medicine. The Systolic Blood Pressure Intervention Trial (SPRINT) demonstrated that while intensive blood pressure lowering reduced cardiovascular events, it did not yield equivalent improvements in renal outcomes (55). This paradox suggests that blood pressure levels may not be the primary determinant of renal prognosis. In recent years, the scientific community has increasingly recognised the critical role played by BPV. It is important to note that the current research focus has shifted from static BPV at a single time point to its dynamic evolution over several years, which is essential for assessing long-term risk. Cheng et al. (56) provided the first systematic demonstration that increased systolic BPV during follow-up is an independent risk factor for new-onset chronic kidney disease and renal function deterioration (aHR = 1.33, 95% CI: 1.15–1.52). This indicates a strong association between BPV and renal disease prognosis. The mechanisms by which BPV promotes HRD may involve multiple pathways, including abnormal shear stress fluctuations, vascular remodeling, endothelial dysfunction, and activation of the renin-angiotensin-aldosterone system (57). The urine albumin-to-creatinine ratio (UACR) and estimated glomerular filtration rate (eGFR) are pivotal indicators of renal function, closely associated with cardiovascular disease and CKD prognosis. As demonstrated by Wang et al. (58), there is a strong association between BPV and new-onset CKD and albuminuria in hypertensive patients, with systolic BPV demonstrating a more pronounced relationship. In comparison with the lowest quartile, the highest quartile of systolic BPV was associated with a 90% increased risk of CKD (aHR = 1.90, 95% CI: 1.13–3.19), while the risk of albuminuria events increased by 67% (aHR = 1.67, 95% CI: 1.14–2.45). A prospective study (59) also indicated that long-term increased BPV correlates with albuminuria and declining eGFR. The evidence presented herein indicates that elevated and worsening BPV trends constitute independent risk factors for HRD onset and progression. The pressing question that must be addressed is: The present study seeks to investigate whether treatment strategies that specifically target BPV reduction, in addition to standard antihypertensive therapy, can further improve outcomes in patients with HRD. This finding may indicate a promising avenue for future prospective randomised controlled trials.
BPV promoting microvascular damages in different populations
4
Metabolic syndrome population
4.1
Metabolism is currently recognised as a key factor influencing microvascular disease. Consequently, patients exhibiting diverse metabolic profiles (e.g., diabetes, obesity) demonstrate varying sensitivities and stability to BPV (30, 60–66). The identification of BPV differences across distinct disease states facilitates precise assessment of microvascular disease risk and improves prognosis.
Prolonged hyperglycaemia and blood glucose fluctuations experienced by diabetic patients have been demonstrated to result in oxidative stress, chronic inflammation, and the accumulation of advanced glycation end-products (AGEs). These phenomena have been shown to ultimately lead to endothelial injury and microvascular thrombosis (67). Consequently, diabetic patients are considered to be a high-risk group with regard to microvascular complications. Research has indicated that persistent fluctuations in blood pressure can promote inflammatory responses and exacerbate endothelial damage, thus establishing them as a pivotal factor in the development of diabetic target organ damage (68). A prospective study by Chen et al. (69) further indicated that baseline systolic BPV independently predicts the risk of developing diabetes (HR = 1.973, 95% CI: 1.333–2.920). A large meta-analysis confirmed that in type 2 diabetes patients, each one-standard-deviation increase in long-term systolic BPV significantly elevated the risk of microvascular complications (pooled HR = 1.12, 95% CI: 1.01–1.24) (61). This finding lends further support to the hypothesis that BPV may act as a crucial catalyst for the onset and progression of diabetes. Concurrently, recent studies indicate that SGLT-2 inhibitors effectively improve abnormal nocturnal blood pressure rhythms in diabetic patients by reducing BPV, maintaining blood pressure stability, and lowering the risk of adverse cardiovascular events (70). Furthermore, a prospective study indicated that intensive statin therapy (target LDL-C < 70 mg/dL) has been demonstrated to have significant cardiovascular protective effects, but only in diabetic patients with high BPV (63). This underscores the considerable potential of stratified treatment based on BPV levels for cardiovascular protection in diabetic patients.
Obesity has been identified as an independent risk factor for cardiovascular disease (71). The epidemiological evidence indicates that approximately 8% of hypertensive patients also have obesity (72), with this subgroup exhibiting more pronounced blood pressure fluctuations (73). Concurrently, studies indicate that obese patients face markedly increased risks of microvascular target organ damage, including retinopathy, coronary heart disease, and renal insufficiency (74, 75). Emerging evidence suggests that obesity may exacerbate microvascular target organ damage by increasing blood pressure instability through elevated BPV. Specifically, on one hand, the nocturnal obstructive sleep apnoea that is commonly associated with obesity can lead to excessive sympathetic nervous system activation. Conversely, as articulated by Koenen et al. (65), aberrant proliferation and remodelling of visceral adipose tissue precipitate heightened immune cell infiltration and secretion of multiple vasoconstrictive mediators, concomitant with diminished secretion of salutary vasodilatory factors such as adiponectin. The combined effect of these mechanisms is the disruption of the body's physiological regulation of blood pressure. A domestic cross-sectional study provides more direct epidemiological evidence: compared with individuals of normal weight, overweight individuals had a 10% increased risk of developing sustained systolic blood pressure (SBP) (HR = 1.10, 95% CI: 1.04–1.15), while this risk further escalated to 23% in obese individuals (HR = 1.23, 95% CI: 1.15–1.32) (30). It is noteworthy that recent scholarly contributions propose adipocyte dysfunction as a pivotal contributor to hypertension and abnormal BPV (66). Consequently, obese patients may exhibit higher BPV, and meticulous monitoring and control of blood pressure stability in obese patients can effectively reduce the risk of cardiovascular disease.
Elderly population
4.2
In addition to individuals with diabetes and obesity, the elderly are another high-risk group for developing microvascular complications. Aging itself increases the prevalence of hypertension in the elderly through multiple pathophysiological mechanisms, including atherosclerosis, decreased baroreflex sensitivity, altered renin-angiotensin-aldosterone system (RAAS) regulation and reduced renal sodium excretion (76). It also serves as a common basis for both short-term and long-term abnormal BPV elevation in this population. Elevated BPV places greater strain on microvascular beds that are already affected by vascular stiffening and impaired blood pressure self-regulation. This exacerbates endothelial injury, promotes inflammatory responses and vascular remodelling, and increases the risk of target organ damage independently of blood pressure levels. Recent studies indicate that elevated BPV is a strong predictor of cognitive impairment, dementia and cardiovascular events in older adults (77, 78). For example, the S.AGES prospective cohort study showed that inter-visit BPV is significantly correlated with an increased risk of cognitive impairment and dementia in people aged 65 years and over (aHR > 1.21, p < 0.029) (77). A post-hoc analysis of the ASPREE (Aspirin in Reducing Events in the Elderly) trial also confirmed that elevated blood pressure variability (BPV) during clinic visits was independently associated with an increased risk of ischaemic stroke (highest vs. lowest tertile: aHR = 1.56, 95% CI: 1.04–2.33) and cardiovascular disease (highest vs. lowest tertile: aHR = 1.36, 95% CI: 1.08–1.70) (78). It is noteworthy that the relationship between BPV and renal function varies by population. Further analysis of the ASPREE trial revealed that long-term BPV was unable to predict renal outcomes in the general elderly population (79), whereas markedly elevated BPV has been confirmed as an independent risk factor that accelerates renal deterioration in elderly patients with chronic kidney disease (80). Therefore, BPV should be considered as a target for antihypertensive treatment in elderly individuals with cardiovascular risk factors. The conflicting aspects of blood pressure management strategies in the elderly population must be recognised: sustained blood pressure reduction is necessary to minimise target organ damage, but excessive blood pressure lowering and inappropriate medication use may lead to cerebral hypoperfusion and orthostatic hypotension, increasing the risk of syncope, falls and cardiovascular events (81). Therefore, antihypertensive therapy for elderly patients should prioritise long-acting, stable antihypertensive agents (such as calcium channel blockers or renin–angiotensin system inhibitors) (82). Using home and ambulatory blood pressure monitoring to accurately assess circadian rhythms and amplitude of fluctuation is essential for reducing blood pressure variability in elderly patients and minimising microvascular target organ damage.
BPV-targeted interventions for microvascular protection
5
Blood pressure variability (BPV) is an independent predictor of cardiovascular events, distinct from mean blood pressure. It is strongly associated with microvascular damage and cardiovascular events. Therefore, it is essential to incorporate BPV into hypertension management strategies. An effective BPV intervention must combine individualised pharmacotherapy with systematic lifestyle modifications to stabilise haemodynamics through multiple pathways and to prevent microvascular injury.
Firstly, different antihypertensive drugs directly influence BPV. Studies indicate that treatment regimens incorporating long-acting dihydropyridine calcium channel blockers (such as amlodipine) or diuretics are more effective at reducing both short-term and long-term BPV (47, 83). De la Sierra et al. (47) concluded that amlodipine combined with diuretics is more effective than other major classes of antihypertensive drug at reducing short-term BPV in hypertensive patients, and this remains the case in combination therapy regimens. A post hoc analysis of the SPRINT trial further confirmed that sustained amlodipine therapy reduced systolic BPV by approximately 2.05 mmHg during follow-up (83), potentially due to its potent and sustained vasodilatory effects. Therefore, for patients with markedly elevated BPV, prioritising such agents in antihypertensive regimens may reduce residual cardiovascular risk.
Secondly, dietary intervention is a key strategy for stabilising BPV. It is crucial to restrict sodium intake and increase potassium consumption. Studies by Chang et al. (26) suggest that a lower urinary sodium-to-potassium ratio is associated with reduced short-term BPV. Specifically, the DASH diet alone has limited impact on reducing short-term BPV. However, combining the DASH diet with strict sodium restriction is a more effective way of lowering both blood pressure and short-term BPV. This highlights the importance of optimising dietary composition and strictly controlling sodium intake. Furthermore, increasing dietary nitrate intake can stabilise blood pressure by improving endothelial function and nitric oxide bioavailability. A randomised controlled trial confirmed that seven days of dietary nitrate supplementation significantly reduced blood pressure fluctuations and cerebral blood flow velocity in patients with transient ischaemic attacks (84). Therefore, incorporating evidence-based dietary modifications into hypertension management is a key strategy for controlling blood pressure and reducing BPV.
Finally, non-pharmacological approaches, such as regular exercise and weight management, can improve BPV. Meta-analyses indicate that regular exercise significantly improves both systolic and diastolic BPV, with aerobic exercise being particularly effective at reducing diastolic BPV (85). A randomised controlled trial demonstrated that a combination of aerobic exercise and resistance training is more effective than aerobic exercise alone in reducing short-term BPV (86). Additionally, proactive weight management is crucial for obese patients. A randomised controlled trial involving 100 obese, hypertensive patients demonstrated that adding bariatric surgery to baseline antihypertensive therapy reduced 24-hour BPV without altering the circadian rhythm of blood pressure (87). These findings further emphasise the importance of exercise and weight management for hypertensive patients with severe obesity in achieving target blood pressure levels.
Conclusions
6
In conclusion, blood pressure variability (BPV) has been identified as an independent risk factor for microvascular complications arising from hypertension and cardiovascular events, thereby emphasising its critical importance in the management of blood pressure (Figure 1). This current review has demonstrated that BPV exacerbates target organ damage independently of mean blood pressure levels through mechanisms such as aggravated endothelial injury and abnormal vascular shear stress. This is particularly evident in elderly populations and those with hypertension complicated by diabetes and obesity, also known as metabolic syndrome. Actually, the intrinsic link between BPV and microvascular complication risk is more complex, offering new perspectives for precision risk management. In clinical practice, beyond strict control of mean blood pressure, long-term monitoring and intervention targeting BPV should be integrated into hypertension management strategies. Ambulatory blood pressure monitoring (ABPM) and home blood pressure monitoring (HBPM) have been shown to be effective tools for the assessment of BPV. It is recommended that these techniques be adopted more widely in clinical settings in order to optimise blood pressure management and improve patient outcomes. Despite substantial research supporting BPV as an independent risk factor for microvascular damage in hypertension, there are currently significant limitations in this field that hinder its clinical translation. On the one hand, existing studies exhibit high heterogeneity, which is manifested in the following ways: (1) inconsistent methodological standards, including monitoring techniques (e.g., office blood pressure, ambulatory blood pressure monitoring and continuous monitoring), analytical indicators (e.g., SD, CV and ARV) and calculation methods; (2) varied temporal scales of focus (e.g., beat to beat, 24-hour and inter-visit), each carrying distinct physiological and pathological implications; and (3) substantial variations in the characteristics of the study population (e.g., age and comorbidities), which limits the generalisability of the findings. On the other hand, the most critical issue is the current lack of large-scale, prospective, randomized controlled trials demonstrating whether interventions specifically targeting BPV reduction can independently reduce microvascular complications and clinical events beyond the effects of lowering mean blood pressure levels. Therefore, future research urgently requires standardised BPV assessment protocols and intervention studies targeting clinical endpoints in clearly defined high-risk subgroups (e.g., patients with diabetes, obesity or advanced age), in order to advance the transition of BPV from a risk marker to a clinical therapeutic target.
Blood pressure variability (BPV) and hypertensive microvascular disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Farrar J Frieden T. WHO Global report on hypertension 2025. Lancet. (2025) 406(10517):2318–9. 10.1016/S 0140-6736(25)02208-141241506 · doi ↗ · pubmed ↗
- 2De La Sierra A. Blood pressure variability as a risk factor for cardiovascular disease: which antihypertensive agents are more effective? J Clin Med. (2023) 12(19):6167. 10.3390/jcm 1219616737834811 PMC 10573370 · doi ↗ · pubmed ↗
- 3Wan EYF Yu EYT Chin WY Fong DYT Choi EPH Lam CLK. Association of visit-to-visit variability of systolic blood pressure with cardiovascular disease, chronic kidney disease and mortality in patients with hypertension. J Hypertens. (2020) 38(5):943–53. 10.1097/HJH.000000000000234731904623 · doi ↗ · pubmed ↗
- 4Liu Y Luo X Jia H Yu B. The effect of blood pressure variability on coronary atherosclerosis plaques. Front Cardiovasc Med. (2022) 9:803810. 10.3389/fcvm.2022.80381035369353 PMC 8965230 · doi ↗ · pubmed ↗
- 5Lattanzi S Słomka A Divani AA. Blood pressure variability and cerebrovascular reactivity. Am J Hypertens. (2023) 36(1):19–20. 10.1093/ajh/hpac 11436219582 · doi ↗ · pubmed ↗
- 6Karadag MF. A new potential risk factor for central serous chorioretinopathy: blood pressure variability. Eye. (2021) 35(8):2190–5. 10.1038/s 41433-020-01222-133077907 PMC 8302670 · doi ↗ · pubmed ↗
- 7Spallone V. Blood pressure variability and autonomic dysfunction. Curr Diab Rep. (2018) 18(12):137. 10.1007/s 11892-018-1108-z 30361834 · doi ↗ · pubmed ↗
- 8Zhang Y Agnoletti D Blacher J Safar ME. Blood pressure variability in relation to autonomic nervous system dysregulation: the X-CELLENT study. Hypertens Res. (2012) 35(4):399–403. 10.1038/hr.2011.20322129516 · doi ↗ · pubmed ↗