Fulminant Clostridioides difficile Infection During Repeated High-Dose Cytarabine Consolidation for Acute Myeloid Leukemia: A Fatal Case
Eisaku Iwanaga, Hirotomo Nakata, Rie Furuta, Kenji Tokunaga, Jun-Ichirou Yasunaga

TL;DR
A 69-year-old woman with leukemia died from a severe recurrence of Clostridioides difficile infection during chemotherapy, highlighting the risks of using metronidazole in high-risk patients.
Contribution
This case emphasizes the unpredictable severity of recurrent CDI and the importance of using guideline-recommended antibiotics like fidaxomicin or vancomycin in high-risk patients.
Findings
The patient's first CDI episode was mild and resolved with oral metronidazole.
The second CDI episode rapidly progressed to septic shock and death despite intravenous metronidazole and vancomycin.
Autopsy confirmed pseudomembranous colitis, and the CDI strain was not hypervirulent.
Abstract
Fulminant Clostridioides difficile infection (CDI) is a life-threatening complication during intensive chemotherapy. We report a 69-year-old woman with acute myeloid leukemia who had two CDI episodes of different severity following sequential high-dose cytarabine consolidation cycles. The initial episode was mild diarrhea during myelosuppression and was managed by oral metronidazole. Her diarrhea resolved by day 20, and she was discharged on day 24. She started her second cycle of consolidation 41 days after the first cycle with the same antibiotic prophylaxis. On day 17, she developed watery diarrhea and abdominal pain. Oral metronidazole was started for suspected recurrence. However, she rapidly developed severe metabolic acidosis and septic shock, requiring mechanical ventilation, vasopressors, and continuous hemodiafiltration. Computed tomography showed thickened colonic walls and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
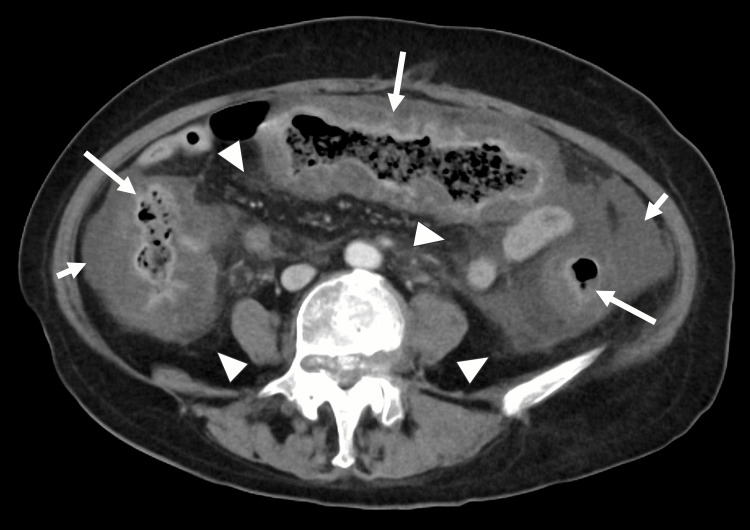 Figure 1
Figure 1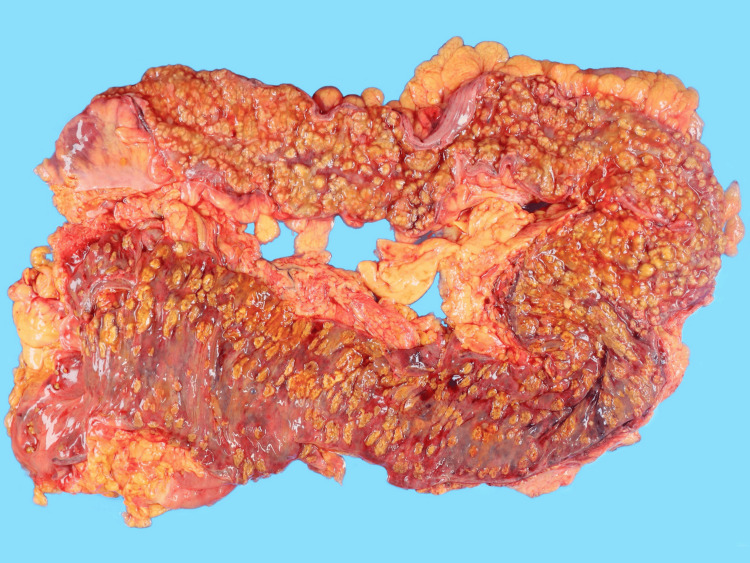 Figure 2
Figure 2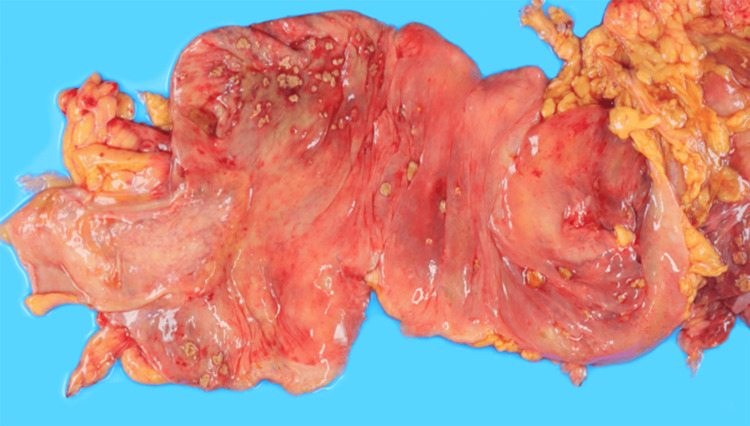 Figure 3
Figure 3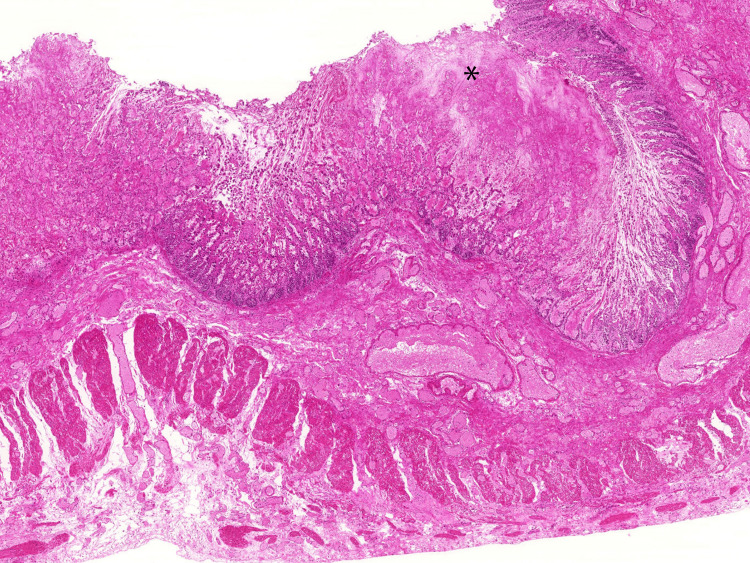 Figure 4
Figure 4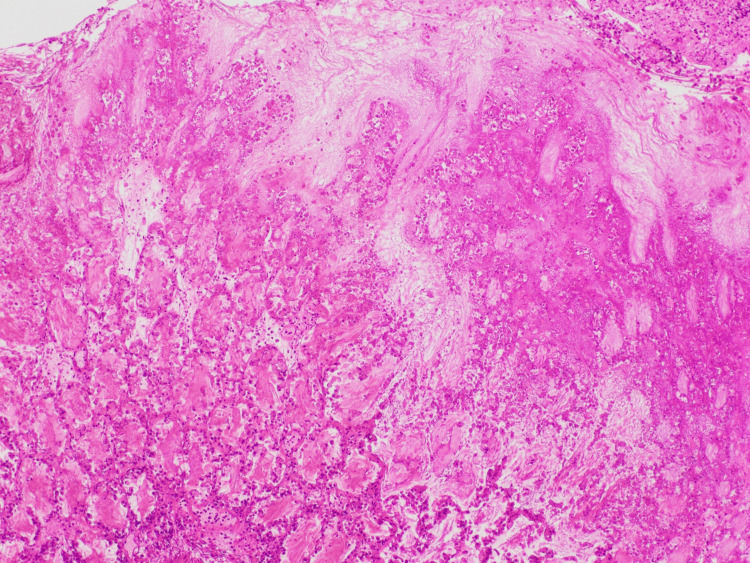 Figure 5
Figure 5| Parameter | Day -1 | Day 18 (8:30) | Day 18 (10:34) | Day 18 (16:17) | Unit | Reference range |
| WBC | 9400 | 100 | - | - | /µL | 3,300-8,600 |
| Neutrophils | 83 | 8 | - | - | % | 42.4-75.0 |
| Lymphocytes | 7 | 67 | - | - | % | 18.2-47.7 |
| Monocytes | 10 | 25 | - | - | % | 3.3-9.0 |
| Hb | 6.5 | 11.3 | - | - | g/dL | 11.6-14.8 |
| Plt | 18 × 104 | 2.8 × 104 | - | - | /µL | 15.8-34.8 × 104 |
| Alb | 3.2 | 2.1 | - | - | g/dL | 4.1-5.1 |
| T-Bil | 0.5 | 1.1 | - | - | mg/dL | 0.4-1.5 |
| Crea | 0.64 | 1.28 | - | - | mg/dL | 0.46-0.79 |
| CRP | 3.93 | 38.9 | - | - | mg/dL | 0.00-0.14 |
| PT | - | 60 | - | - | % | 80-120 |
| APTT | - | 42.5 | - | - | s | 24.0-39.0 |
| Fibrinogen | - | >700 | - | - | mg/dL | 200-400 |
| D-dimer | - | 5.5 | - | - | µg/mL | <1.0 |
| Venous pH | - | - | 7.432 | 7.255 | - | 7.33-7.43 |
| Venous pCO2 | - | - | 28.0 | 19.2 | mmHg | 40-50 |
| Venous HCO₃⁻ | - | - | 18.3 | 8.3 | mmol/L | 22-29 |
| Venous lactate | - | - | 2.82 | 11.5 | mmol/L | 0.5-2.2 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClostridium difficile and Clostridium perfringens research · Antibiotic Use and Resistance · Neutropenia and Cancer Infections
Introduction
Clostridioides difficile infection (CDI) is a common cause of antibiotic-associated colitis and is often observed among hospitalized and immunocompromised patients [1]. Despite the majority of the cases being responsive to proper antimicrobial treatment, fulminant CDI, which is associated with toxic megacolon, septic shock, and multiple organ failure, is still life-threatening [2,3]. Hematologic malignancy patients are also more susceptible to CDI due to intensive chemotherapy, prolonged neutropenia, and exposure to broad-spectrum antibiotics [4]. The prevention of the recurrence of CDI is a significant problem in the high-risk groups.
CDI is usually manageable in patients with acute myeloid leukemia (AML), but sudden deterioration can be fatal. The causes of such a sudden decline remain poorly understood [4,5]. It is unclear why some patients experience dramatically different levels of disease severity despite identical chemotherapy protocols [5].
We report an autopsy-confirmed case of fulminant CDI that occurred during the second cycle of high-dose cytarabine consolidation for AML, while the first cycle produced only a mild, treatment-responsive episode. This case highlights the unpredictable nature of recurrent CDI during intensive chemotherapy and underscores the importance of appropriate antimicrobial selection.
Case presentation
A 69-year-old woman was diagnosed with AML harboring an NPM1 mutation and achieved complete remission after standard induction chemotherapy. She received her initial high-dose cytarabine consolidation with prophylaxis of levofloxacin, posaconazole, and a proton pump inhibitor. She had watery diarrhea during the myelosuppressive phase. CDI was diagnosed based on positive glutamate dehydrogenase (GDH) antigen and toxin A/B assays in stool. She was treated with oral metronidazole 500 mg every eight hours, showed prompt clinical improvement, and was discharged.
She received a second course of consolidation therapy using the same chemotherapy regimen and prophylaxis 41 days after the first cycle (18 days after discharge). Baseline laboratory values before her second consolidation cycle showed moderate inflammation (Table 1). On day 15, she developed febrile neutropenia, and cefepime was started. On day 16, she developed intermittent epigastric pain. On day 17, she developed frequent watery diarrhea. Given her history of CDI, recurrence was suspected. A rapid enzyme immunoassay detected GDH antigen and toxins A/B (approximately five to six weeks after the initial positive toxin assay, consistent with the commonly used two-to-eight-week window for recurrent CDI). Therefore, oral metronidazole was started. However, her fever persisted, intravenous teicoplanin was added, and cefepime was escalated to meropenem.
Her abdominal pain deteriorated rapidly, despite treatment. On day 18 morning, she experienced severe, diffuse abdominal pain. Physical examination showed abdominal distension and diminished bowel sounds with sharp tenderness and rebound tenderness in the epigastrium and lower abdomen without guarding. Abdominal CT with contrast enhancement revealed significant edematous thickening of the walls of the entire colon without bowel necrosis, perforation, or abscess (Figure 1). She experienced shock in the evening of day 18 (blood pressure 87/33 mmHg, heart rate 101 bpm, respiratory rate 44 breaths per minute, temperature 36.4°C, SpO₂ 98% on room air) and reduced consciousness (Glasgow Coma Scale 14: E3V5M6). Venous lactate increased from 2.82 mmol/L at 10:34 to 11.5 mmol/L at 16:17, accompanied by worsening metabolic acidosis (Table 1). Norepinephrine was initiated, but adequate hemodynamic stabilization was not achieved. She was endotracheally intubated and transferred to the intensive care unit, where continuous hemodiafiltration was initiated. Vancomycin 500 mg every six hours was administered via nasogastric tube, and metronidazole was switched from oral to intravenous administration at 500 mg every eight hours. Subsequent stool testing showed Clostridioides difficile growth (10⁶ colony-forming units). Polymerase chain reaction detected toxin B but was negative for mutant tcdC and binary toxin genes.
Contrast-enhanced abdominal CT on day 18 revealed marked edematous wall thickening from the rectum to the ascending colon (long arrows), with pericolonic fat stranding (arrowheads) and ascites (short arrows). No perforation or abscess formation was identified. Mucosal enhancement was preservedCT: computed tomography
By day 19, neutrophil recovery was observed; however, systemic perfusion did not improve, and she progressed to multiple organ failure and died on day 21. Autopsy showed that there were diffuse yellow-green flat elevations and inflammatory exudates that extended through the colon to the rectum, and the ileum was spared (Figures 2-3). Histopathological examination showed characteristic pseudomembrane formation on the colonic mucosal surface with marked transmural edema consistent with fulminant pseudomembranous colitis (Figures 4-5).
Multiple yellow-green flat elevations with accompanying mucosal erythema were observed extending from the colon to the rectum
No pseudomembrane formation was observed in the ileum
Hematoxylin and eosin-stained section showing mucosa-limited inflammation with eruptive pseudomembrane formation on the surface (asterisk) and marked transmural edema involving the mucosa, submucosa, muscularis propria, and serosa
High-power view of the pseudomembrane indicated by the asterisk in Figure 4. The pseudomembrane was composed of mucus and fibrin, containing abundant neutrophils and necrotic debris. No pathogenic organisms suggestive of other infectious diseases were identified
Discussion
The case shows an extreme increase in the severity of CDI between two identical rounds of consolidation chemotherapy. There are several possible causes of the fulminant presentation in the second cycle: cumulative mucosal toxicity from two high-dose cytarabine cycles [6], the patient's age (69 years), hypoalbuminemia (3.2→2.1 g/dL), and neutropenia (100/μL). More importantly, the metronidazole selection in both episodes was not optimal. Recent Infectious Diseases Society of America (IDSA)/Society for Healthcare Epidemiology of America (SHEA) guidelines (2021) recommend fidaxomicin or vancomycin as first-line treatment, replacing metronidazole due to its lower efficacy and increased recurrence rates [7]. Fidaxomicin would have been a better choice in this high-risk patient undergoing intensive myelosuppressive chemotherapy to maximize the eradication of Clostridioides difficile. In cases where CDI recurred, the use of metronidazole (orally) rather than switching to vancomycin and fidaxomicin was a missed opportunity. This suboptimal antimicrobial selection may have contributed to incomplete clearance and recurrent infections of increasing severity.
An important finding is the absence of markers for hypervirulent strains. Binary toxin and mutant tcdC are used as surrogate markers of hypervirulence to characterize epidemic strains of RT027 and RT078 in Western countries. The PCR of our patient's stool was negative for both markers, indicating that this was not an epidemic hypervirulent strain. This is consistent with Japanese epidemiology: marker-positive strains are rare in Japan, with non-hypervirulent strains (RT018, RT014, RT002, RT369, RT017) comprising over three-quarters of isolates and capable of causing fulminant CDI [8]. Our case demonstrates that non-hypervirulent strains can lead to severe outcomes when combined with intensive chemotherapy and suboptimal antimicrobial therapy.
Few similar cases have been reported. Yamamoto et al. reported fulminant CDI in an elderly patient with AML undergoing low-intensity therapy that responded to fidaxomicin [9]. Lee et al. described a young AML patient who was treated successfully with fecal microbiota transplantation (FMT) [10]. Carmeliet et al. reported a case of an AML patient who needed a colectomy [11]. In contrast, our patient had high-intensity consolidation, cumulative cytarabine-induced damage, severe neutropenia, advanced age, and suboptimal antimicrobial therapy, all contributing to the fatal outcome. Limitations in treatment were the unavailability of FMT under insurance coverage in Japan and surgical contraindication because of severe neutropenia. A CT scan and autopsy confirmed CDI as the leading cause, with no other source of infection.
For patients undergoing high-dose cytarabine consolidation, adherence to current guidelines is essential. Initial CDI should be treated with fidaxomicin (preferred) or vancomycin rather than metronidazole to achieve complete eradication and minimize the risk of recurrence [7]. Secondary prophylaxis with oral vancomycin 125 mg twice daily may be considered for patients with previous CDI receiving additional cycles of intensive chemotherapy [1]. In the case of fulminant CDI, a combination of vancomycin (orally or nasogastrically) with intravenous metronidazole is indicated [7]. FMT represents an important rescue option when available [12]. Clinicians should recognize that subsequent high-dose cytarabine cycles carry substantial risk and that alternative consolidation strategies may need to be considered, balancing the risk of infection against leukemia control.
Conclusions
This case demonstrates that CDI during repeated high-dose cytarabine consolidation may recur with unpredictably severe manifestations. The use of metronidazole rather than guideline-recommended fidaxomicin or vancomycin may have contributed to incomplete eradication and recurrence with a fatal outcome. In patients receiving intensive myelosuppressive chemotherapy, adherence to current IDSA/SHEA guidelines is important: fidaxomicin or vancomycin is recommended for initial CDI, and secondary prophylaxis may be considered for subsequent chemotherapy cycles. Clinicians must recognize that prior mild CDI does not predict the severity of recurrence, and treatment decisions should be guided by evidence-based recommendations rather than initial disease severity. Autopsy confirmation of diffuse pseudomembranous colitis without hypervirulent strain markers underscores that fulminant CDI can occur with typical strains when combined with intensive chemotherapy and suboptimal antimicrobial selection.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA)Clin Infect Dis Mc Donald LC Gerding DN Johnson S 1486620182946228010.1093/cid/cix 1085 PMC 6018983 · doi ↗ · pubmed ↗
- 2Fulminant Clostridium difficile colitis Curr Opin Crit Care Adams SD Mercer DW 4504551320071759901710.1097/MCC.0b 013e 3282638879 · doi ↗ · pubmed ↗
- 3Fulminant Clostridium difficile colitis: patterns of care and predictors of mortality Arch Surg Sailhamer EA Carson K Chang Y 43343914420091945148510.1001/archsurg.2009.51 · doi ↗ · pubmed ↗
- 4Outcomes of Clostridium difficile infection in hospitalized leukemia patients: a nationwide analysis Infect Control Hosp Epidemiol Luo R Greenberg A Stone CD 7948013620152580108510.1017/ice.2015.54 · doi ↗ · pubmed ↗
- 5Clostridium difficile--more difficult than ever N Engl J Med Kelly CP La Mont JT 1932194035920081897149410.1056/NEJ Mra 0707500 · doi ↗ · pubmed ↗
- 6Characteristics of Clostridium difficile infection in patients hospitalized with myelodysplastic syndrome or acute myelogenous leukemia World J Clin Oncol Shah K Curtin BF Chu C Hwang D Flasar MH von Rosenvinge E 398404820172906727610.5306/wjco.v 8.i 5.398PMC 5638715 · doi ↗ · pubmed ↗
- 7Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of Clostridioides difficile infection in adults Clin Infect Dis Johnson S Lavergne V Skinner AM Gonzales-Luna AJ Garey KW Kelly CP Wilcox MH 1029104473202110.1093/cid/ciab 71834492699 · doi ↗ · pubmed ↗
- 8Molecular epidemiology of endemic Clostridioides difficile infection in Japan Anaerobe Senoh M Kato H 1025107420223499081410.1016/j.anaerobe.2021.102510 · doi ↗ · pubmed ↗