Intercostal Cryoneurolysis for Chest Wall Pain in Patients With Vertebral Osteomyelitis
Renato Abu Hana, Ruben G Ortiz Cordero, Oswaldo A Guevara Tirado, Vinicius Adami Vayego Fornazari, Grit A Adler

TL;DR
This paper presents a case where intercostal cryoneurolysis was used to treat chest wall pain caused by vertebral osteomyelitis.
Contribution
The paper introduces the use of intercostal cryoneurolysis for infection-related chest wall pain, which is rarely discussed.
Findings
A 53-year-old patient with vertebral osteomyelitis experienced chronic chest wall pain.
The patient underwent ultrasound-guided nerve block and CT-guided cryoneurolysis as an alternative to long-term medication.
The case highlights procedural techniques and potential complications of cryoneurolysis for this condition.
Abstract
Intercostal cryoneurolysis (IC) is an image-guided technique that provides prolonged analgesia through targeted cold-induced axonal degeneration. While it is most commonly used for post-traumatic, postoperative, and malignancy-related chest wall pain, its role in infection-associated pain syndromes remains poorly described. We report the case of a 53-year-old man with a history of vertebral osteomyelitis complicated by abscess formation who developed chronic right-sided dermatomal chest wall pain and sought an alternative to long-term pharmacologic therapy. The patient initially underwent an ultrasound-guided diagnostic intercostal nerve block, followed by computed tomography-guided IC. This report discusses patient selection, procedural technique, and potential complications associated with IC for intractable chest wall pain.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
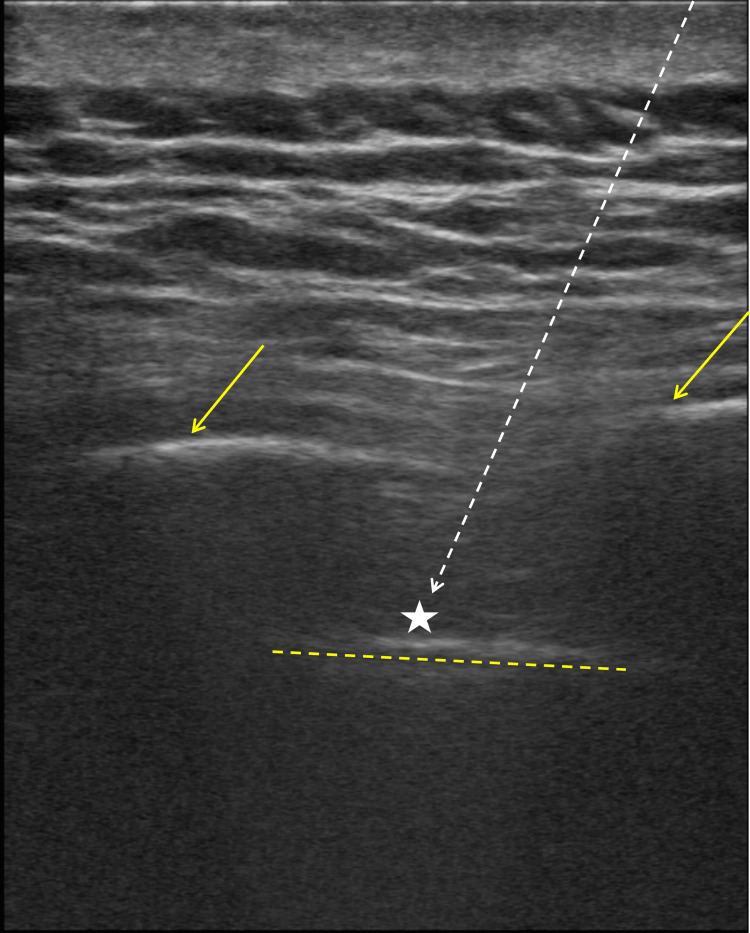 Figure 1
Figure 1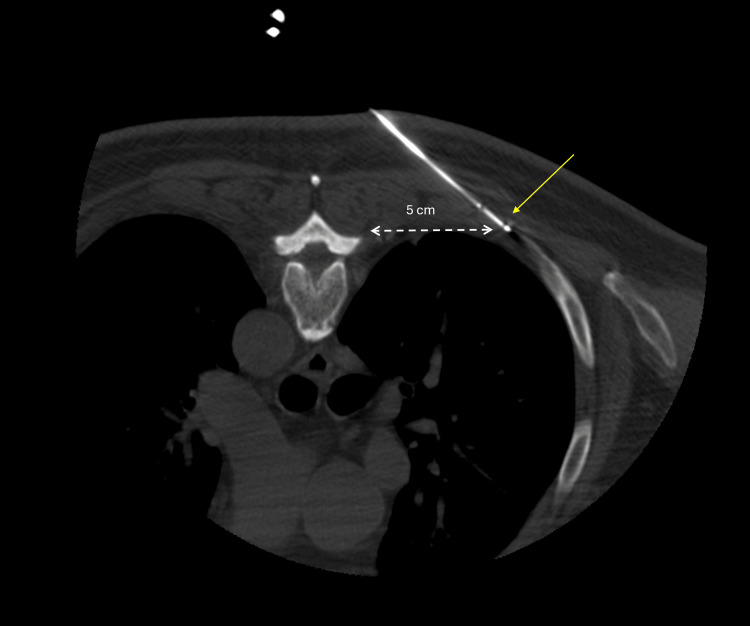 Figure 2
Figure 2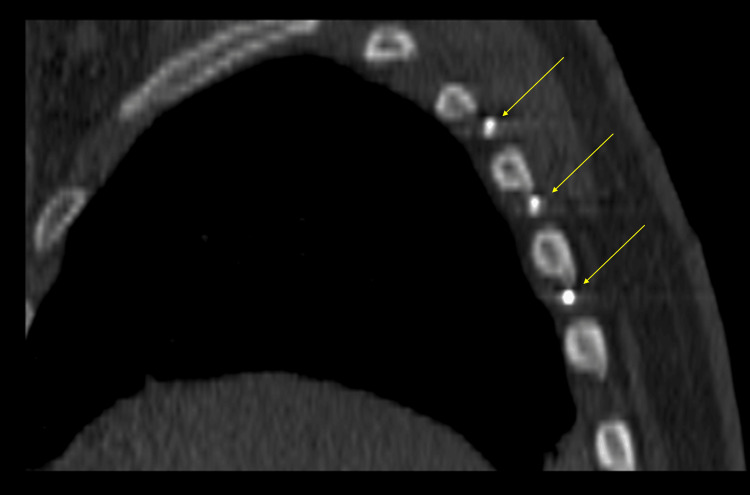 Figure 3
Figure 3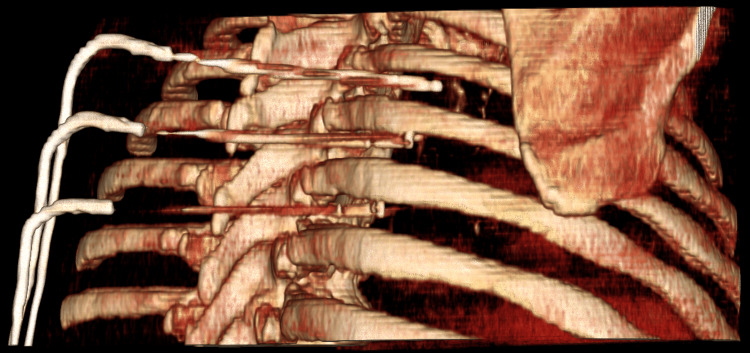 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Osteomyelitis and Bone Disorders Research · Orthopedic Infections and Treatments
Introduction
Chronic chest wall pain represents a heterogeneous clinical entity, with etiologies ranging from musculoskeletal disorders to neuropathic and visceral causes [1,2]. In rare cases, spinal infections such as vertebral osteomyelitis or paraspinal abscesses may manifest as radicular or dermatomal chest wall pain, posing diagnostic and therapeutic challenges [3-5]. Pain associated with spinal infection is thought to result from inflammatory changes and compression of adjacent nerve roots [3,4]. Case reports have described an association between inflammatory masses or osseous destruction and band-like, nonpleuritic chest pain [4]. Additionally, epidural infections may present with radicular pain corresponding to the dermatomal distribution of the affected vertebral level [3].
Because the intercostal nerves arise from the anterior rami of T1-T12 and innervate the thoracic wall and parietal pleura, thoracic spine pathology can produce band-like, dermatomal chest wall pain [1]. Standard management strategies often rely on pharmacologic therapies, including opioids and neuromodulatory agents, which may be poorly tolerated or undesirable for long-term use due to concerns regarding dependence [2].
Intercostal cryoneurolysis (IC) is a minimally invasive, image-guided technique that induces reversible axonal injury through cold application, resulting in prolonged analgesia while preserving nerve integrity [1]. It has been described in the management of post-thoracotomy pain, rib fractures, chest wall malignancies, and intercostal neuralgia [1,6,7]. Additionally, Cha et al. demonstrated that IC may reduce inpatient opioid use and hospital length of stay in selected chest wall pain populations [6]. However, its use in infection-associated neuropathic chest wall pain remains poorly described in the literature.
Case presentation
A 53-year-old man with multiple comorbidities, including insulin-dependent diabetes mellitus and paraplegia secondary to a prior deep T4-T8 paraspinal abscess with chronic osteomyelitis, was admitted for a urinary tract infection (UTI) and referred to interventional radiology for evaluation of a one-year history of chronic, intractable right-sided chest wall pain in the T4-T7 dermatomal distribution. The pain was described as burning and shock-like, associated with painful muscle spasms, and had been poorly controlled with medical therapy, requiring chronic opioid use. At the time of evaluation, there was no evidence of active thoracic osteomyelitis.
A structured pain assessment using the Douleur Neuropathique en 4 questions (DN4) questionnaire yielded a score of 6/10, consistent with a neuropathic pain component [8]. The DN4 is a validated 10-item screening tool that differentiates neuropathic from nonneuropathic pain based on symptom descriptors and bedside sensory testing, with scores ≥4/10 supporting a neuropathic pain diagnosis [8] (see the Appendix). At the time of evaluation, the patient reported partial symptom control with oral oxycodone (10 mg) and diazepam (10 mg) but expressed concern regarding long-term opioid use. After discussion of treatment options, informed consent was obtained to proceed with an ultrasound-guided right intercostal nerve block as a short-term therapeutic measure and diagnostic step to assess candidacy for a more durable intervention such as cryoneurolysis.
Laboratory studies obtained prior to the procedure demonstrated mild anemia (hemoglobin 10.9 g/dL), normal white blood cell count (6.09 10³/µL), and mildly elevated international normalized ratio (INR: 1.2). These findings were reviewed and were not deemed contraindications to the procedure.
For the ultrasound-guided right intercostal nerve block, the patient was positioned in the left lateral decubitus position. Under ultrasound guidance, a 25-gauge spinal needle was advanced into the plane between the innermost intercostal muscle and the pleura at the T5-T6 level, where 3 mL of 0.5% ropivacaine was injected (Figure 1), followed by additional injections of 3 mL at the adjacent T4-T5 and T6-T7 intercostal spaces, for a total volume of 9 mL of 0.5% ropivacaine. The patient tolerated the procedure without complications and subsequently reported complete resolution of symptoms, supporting the intercostal nerves as the primary pain generators and consistent with previously described diagnostic approaches for neuropathic chest wall pain [1,6].
Ultrasound-guided intercostal nerve block. A 25-gauge spinal needle (limited needle visualization; white dashed arrow) is advanced with a caudal to cranial angulation into the subcostal groove (star), positioned just superior to the pleura (yellow dashed line) and between adjacent ribs (solid yellow arrows)
Two weeks after the nerve block, the dermatomal pain and muscle spasms recurred while the patient was receiving extended antibiotic therapy for a multidrug-resistant UTI in the hospital’s rehabilitation unit. Interventional radiology was reconsulted, and the patient was scheduled for computed tomography (CT)-guided right IC. Laboratory studies at that time demonstrated persistent mild anemia (hemoglobin 10.7 g/dL), a normal white blood cell count (5.05 × 10³/µL), and a minimally elevated INR (1.4), which were again not considered contraindications to the procedure.
After informed consent was obtained, the procedure was performed with the patient in the prone position under moderate sedation using 3 mg of midazolam and 150 mcg of fentanyl, with standard pre- and postsedation assessment and continuous cardiorespiratory monitoring. Localizing CT images were obtained. The skin and subcutaneous tissue were anesthetized with 15 mL of 2% lidocaine.
Under CT guidance, three 17-gauge ICESEED™ 1.5 cryoablation probes (Boston Scientific, Boston, MA) were inserted 5 cm from the right neuroforamen into the T4-5, T5-6, and T6-7 intercostal spaces and 5 mm from the subcostal groove to avoid vascular injury with the probe (Figures 2-4). Once probes were placed, two alternating freeze-thaw cycles were performed, with the first cycle being an eight-minute ablation at 100%, followed by an active three-minute thaw, and the second cycle being a three-minute ablation at 100%, followed by a three-minute active thaw.
Intraprocedural axial computed tomographic image of the cryoablation probe placement (yellow arrow), at the level of the affected rib with ablation zone distancing 5 mm away from the subcostal groove and 5 cm away from the thoracic nerve roots
Intraprocedural sagittal computed tomographic image showing three cryoablation probes (arrows) within T4-T7 intercostal spaces
Multiplanar CT reconstruction demonstrating multiple cryoprobes from T4 to T7 intercostal levelsCT: computed tomography
Intermittent CT imaging after the initial eight-minute freeze demonstrated appropriate ice-ball formation. Postcryoneurolysis CT showed no acute complications, including pneumothorax, lung injury, or hematoma. The patient tolerated the procedure well and remained in the department for one hour for routine postprocedural monitoring.
On short-term inpatient follow-up evaluation, the patient reported significant improvement in his muscle spasms after several days. The patient was later discharged to the rehabilitation unit to continue his ongoing antibiotic treatment for his UTI.
Discussion
Chest wall pain secondary to infection, such as vertebral osteomyelitis, is uncommon and may result from nerve root irritation or inflammatory extension into adjacent neural structures [3-5]. In such cases, accurate identification of a neuropathic pain component is essential to guide targeted interventions. The DN4 questionnaire is a validated and widely used screening tool for neuropathic pain and provides objective support for procedural decision-making in this case [8]. More specifically, a DN4 score of ≥4/10 has good diagnostic performance, with about 83% sensitivity and 90% specificity for neuropathic pain, and can correctly classify pain in approximately 86% of patients [8].
Analgesic strategies for chronic neuropathic chest wall pain can include multimodal pharmacotherapy with nonsteroidal anti-inflammatory drugs, opioids, and gabapentin [1,2]. However, long-term use of these medications can lead to dependence, tolerance, or side effects [1]. Regional nerve blocks can also be used for pain management, but their analgesic effect is often temporary [6,7]. While our patient’s dermatomal chest pain was being managed adequately by oral pain medications, his desire to find a longer lasting and nonaddictive solution in conjunction with the chronicity of his pain led to the consideration of an intercostal block followed by IC.
IC has demonstrated efficacy in managing various forms of neuropathic chest wall pain while reducing opioid consumption and improving quality of life [1,6,7]. Complications are low, and reported adverse events include chest wall hematomas, pneumothorax, chest wall laxity and numbness, neuroma or pseudohernia formation, and postoperative neuralgia [1,6,8]. If performed using appropriate technique and under imaging guidance, complications are minimized because IC does not damage important structures, such as the perineurium, epineurium, vessels, or bones [1,6,7].
In our patient, the use of CT guidance to position the probe within the subcostal groove while maintaining a safe distance from critical structures, together with real-time monitoring of ice-ball formation, allowed the procedure to be completed without any immediate or delayed complications. Furthermore, our case highlights that, when combined with structured neuropathic pain assessment and confirmatory diagnostic nerve blocks, IC was associated with symptomatic improvement [1,6].
Conclusions
IC is an image-guided, minimally invasive technique that has been used for the treatment of post-traumatic, postoperative, malignant, and idiopathic neuropathic chest wall pain. This report describes a rare case in which IC provided a nonpharmacological pain control alternative for chronic dermatomal chest wall pain presumed to be a sequela of prior vertebral osteomyelitis following appropriate neuropathic pain assessment and confirmatory diagnostic nerve block. Although limited to a single patient, this case suggests that IC may provide sustained analgesia in selected patients with infection-associated neuropathic chest wall pain. Further studies and long-term follow-up are needed to better characterize the durability of pain relief after IC in this population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intercostal cryoneurolysis Semin Intervent Radiol Huang J Delijani K El Khudari H Gunn AJ 1671713920223578199010.1055/s-0042-1745763 PMC 9246488 · doi ↗ · pubmed ↗
- 2Chronic pain: an update on burden, best practices, and new advances Lancet Cohen SP Vase L Hooten WM 2082209739720213406214310.1016/S 0140-6736(21)00393-7 · doi ↗ · pubmed ↗
- 3Paraspinal and extensive epidural abscess: the great masqueraders of abdominal pain Case Rep Neurol Med Chu A Aung TT Shankar U 103624201520152677084710.1155/2015/103624 PMC 4684844 · doi ↗ · pubmed ↗
- 4Chest pain? An unusual presentation of vertebral osteomyelitis Case Rep Med Landa C Giddings S Reddy P 416498201320132347666410.1155/2013/416498 PMC 3582057 · doi ↗ · pubmed ↗
- 5Vertebral osteomyelitis presenting with pleuritic chest pain and bilateral pleural effusions Thorax Sullivan PJ Currie D Collins JV Johnstone DJ Morgan A 395396471992160938610.1136/thx.47.5.395PMC 463766 · doi ↗ · pubmed ↗
- 6Efficacy of intercostal cryoneurolysis as an analgesic adjunct for chest wall pain after surgery or trauma: systematic review Trauma Surg Acute Care Open Cha PI Min JG Patil A Choi J Kothary NN Forrester JD 06202110.1136/tsaco-2021-000690 PMC 813715934079913 · doi ↗ · pubmed ↗
- 7Cryoneurolysis of intercostal nerve for rib trauma and intercostal neuralgia in the emergency department: a multidisciplinary approach J Emerg Med Hashemi M Mahmood SM Fernandez J Oswald J 3763816320223624147510.1016/j.jemermed.2022.06.009 · doi ↗ · pubmed ↗
- 8Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN 4)Pain Bouhassira D Attal N Alchaar H 293611420051573362810.1016/j.pain.2004.12.010 · doi ↗ · pubmed ↗