Everolimus as maintenance therapy in advanced neuroendocrine neoplasms: results from the MAVERIC phase II trial
Lorenzo Antonuzzo, Daniele Lavacchi, Francesca Spada, Riccardo Marconcini, Fabio Gelsomino, Vito Amoroso, Federica Cosso, Elisa Pellegrini, Federico Scolari, Clotilde Sparano, Giulia Massaro, Elisa Giommoni, Luca Messerini, Daniele Rossini, Marco Brugia, Francesco Di Costanzo

TL;DR
The MAVERIC trial found that everolimus, as maintenance therapy, significantly improved progression-free survival in patients with advanced neuroendocrine tumors after chemotherapy.
Contribution
The study provides new evidence for the effectiveness of everolimus in metastatic neuroendocrine neoplasms with specific Ki-67 indices.
Findings
Everolimus treatment resulted in a median progression-free survival of 11.8 months compared to 1.8 months in the control group.
Toxicity was consistent with the known safety profile of everolimus, with common adverse events including mucositis and dyslipidemia.
The treatment was particularly effective in GEP-NEN patients, showing a median progression-free survival of 19.9 months.
Abstract
Neuroendocrine neoplasms (NEN) are a heterogeneous disease and chemotherapy (CT) represents the standard first-line treatment for those with a Ki-67 index >20%. MAVERIC is a randomized, multicenter, non-comparative phase II study including patients with metastatic gastroenteropancreatic (GEP-NEN) or large-cell neuroendocrine carcinoma (LCNEC) (Ki-67 20%-55%) according to the 2010 WHO grading system and at least stable disease after first-line CT. Patients were randomized (2:1) to everolimus 10 mg/day or observation until progression or treatment intolerance. The primary endpoint was progression-free survival (PFS); secondary endpoints included overall survival (OS) and safety. Between November 2015 and June 2022, 30 patients were enrolled across 5 Italian centers, with 20 assigned to everolimus and 10 to observation. The analysis included 29 patients (52% GEP-NEN, 48% LCNEC). Median…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
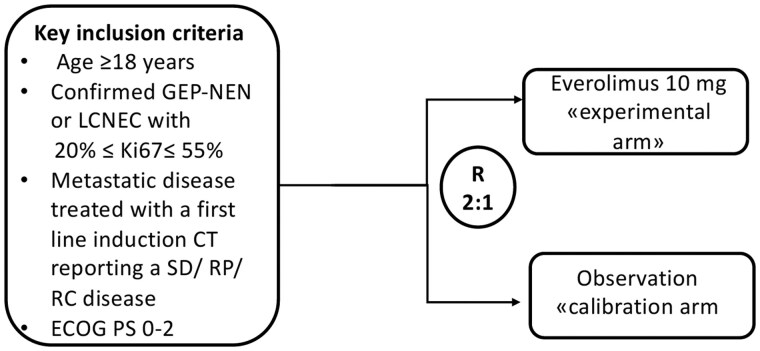 Figure 1
Figure 1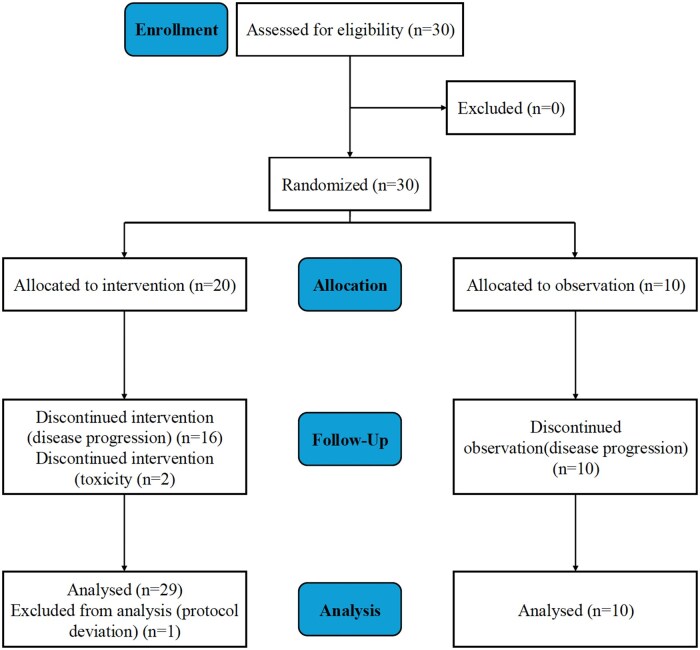 Figure 2
Figure 2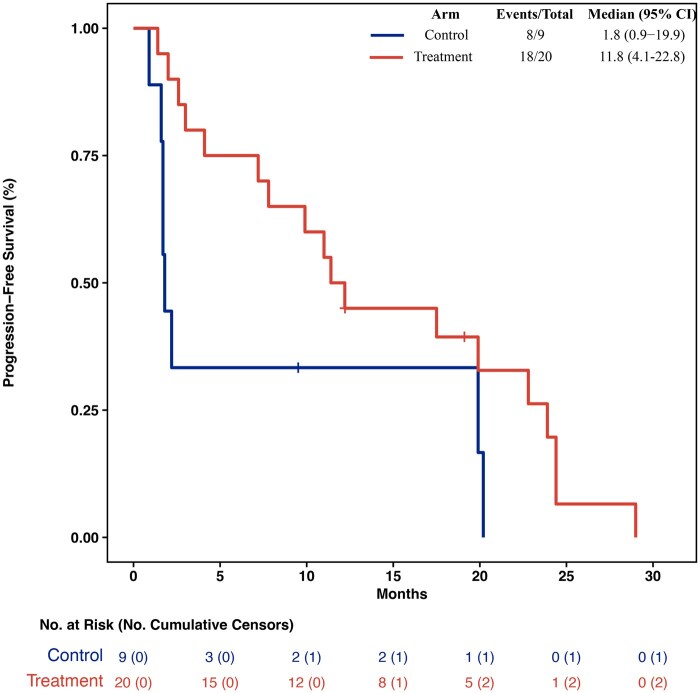 Figure 3
Figure 3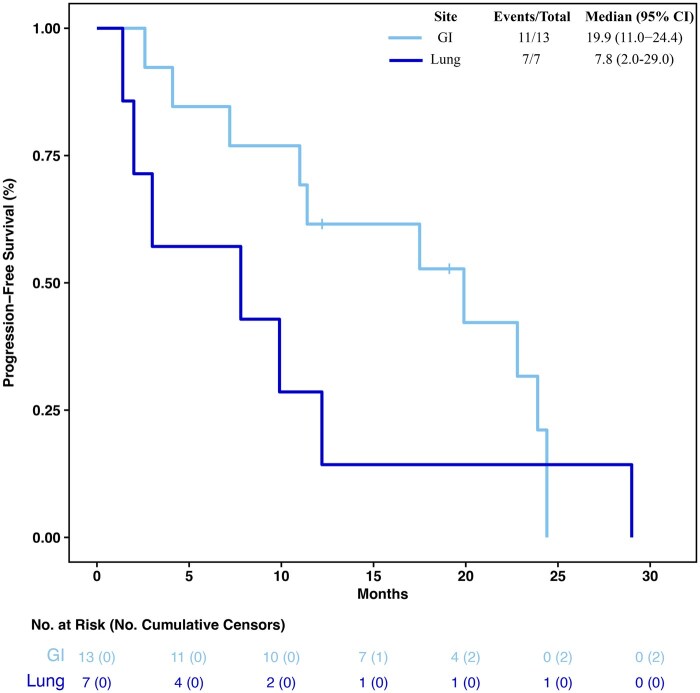 Figure 4
Figure 4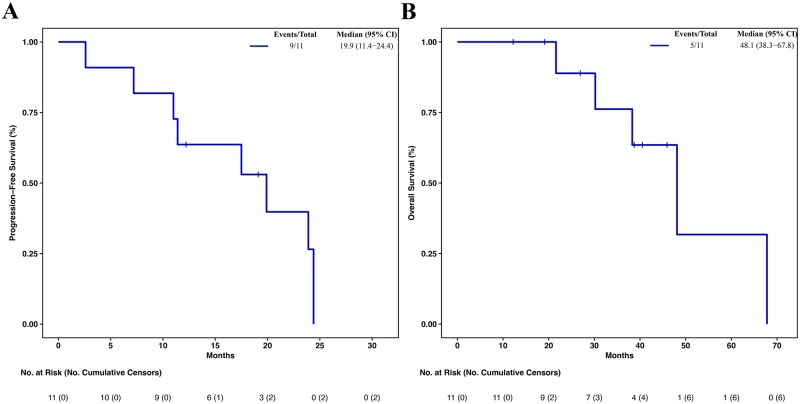 Figure 5
Figure 5| Trial information | ||
|---|---|---|
|
| Neuroendocrine neoplasm | |
|
| Metastatic/advanced | |
|
| 1 prior regimen achieving at least stable disease according to RECIST v1.1 criteria. | |
|
| Phase II | |
|
| Progression-free survival | |
|
| Overall survival and safety | |
|
| Tumoral tissue and blood samples were collected for further investigations exploring prognostic and predictive factors. | |
| Drug information | |
|---|---|
|
| Experimental |
|
| Everolimus |
|
| Novartis Pharmaceuticals Corporation |
|
| Protein kinase inhibitor |
|
| mTOR (mammalian target of rapamycin) kinase inhibitors |
|
| 10 mg |
|
| Oral |
|
| Once daily |
|
| |||
|---|---|---|---|
| Entire cohort ( | Treatment arm ( | Control arm ( | |
|
| |||
|
| 10 (35%) | 5 (25%) | 5 (55%) |
|
| 19 (65%) | 15 (75%) | 4 (45%) |
|
| 63 (38-84) | 64 (38-81) | 61 (52-84) |
|
| |||
|
| 28 (97%) | 20 (100%) | 8 (89%) |
|
| 1 (3%) | 0 (0%) | 1 (11%) |
|
| |||
|
| 8 (28%) | 6 (30%) | 2 (22%) |
|
| 21 (72%) | 14 (70%) | 7 (78%) |
|
| |||
|
| 14 (48%) | 7 (35%) | 7 (78%) |
|
| 15 (52%) | 13 (65%) | 2 (22%) |
|
| |||
|
| 22 (76%) | 17 (85%) | 5 (56%) |
|
| 13 (45%) | 11 (55%) | 2 (22%) |
|
| 9 (31%) | 6 (30%) | 3 (33%) |
|
| 7 (24%) | 3 (15%) | 4 (44%) |
|
| 2 (7%) | 2 (10%) | 0 (0%) |
|
| 5 (17%) | 1 (5%) | 4 (44%) |
|
| |||
|
| 15 (52%) | 13 (65%) | 2 (22%) |
|
| 14 (48%) | 7 (35%) | 7 (78%) |
|
| |||
|
| 13 (45%) | 11 (55%) | 2 (22%) |
|
| 2 (7%) | 2 (10%) | 0 (0%) |
|
| 14 (48%) | 7 (35%) | 7 (78%) |
|
| |||
|
| 12 (41%) | 9 (45%) | 3 (33%) |
|
| 17 (59%) | 11 (55%) | 6 (67%) |
|
| |||
|
| 7 (24%) | 7 (35%) | 0 (0%) |
|
| 22 (76%) | 13 (65%) | 9 (100%) |
|
| |||
|
| 13 (45%) | 8 (40%) | 5 (56%) |
|
| 16 (55%) | 12 (60%) | 4 (44%) |
|
| |||
|
| 16 (55%) | 13 (65%) | 3 (33%) |
|
| 13 (45%) | 7 (35%) | 6 (67%) |
|
| |||
|
| 2 (10%) | 1 (7%) | 1 (17%) |
|
| 13 (65%) | 9 (64%) | 4 (66%) |
|
| 5 (25%) | 4 (29%) | 1 (17%) |
|
| 9 | 6 | 3 |
|
| |||
|
| 14 (88%) | 7 (78%) | 7 (100%) |
|
| 2 (12%) | 2 (22%) | 0 (0%) |
|
| 13 | 11 | 2 |
|
| |||
|
| 8 (28%) | 7 (35%) | 1 (11%) |
|
| 21 (72%) | 13 (65%) | 8 (89%) |
| Primary assessment method | |
|---|---|
|
| Disease control (median progression-free survival). |
|
| 30 |
|
| 20 |
|
| 19 |
|
| 19 |
|
| Objective tumor assessments evaluated by imaging every 12 weeks of the initial randomized period according to RECIST v1.1 criteria. |
|
| Kaplan–Meier graph is provided in |
| Drug-related adverse events in at least 10% of patients | ||
|---|---|---|
| Adverse event | Grade 1 or 2 no. of patients (%) | Grade 3 no. of patients (%) |
|
| 12 (60) | 4 (20) |
|
| 9 (45) | 2 (10) |
|
| 8 (40) | 1 (5) |
|
| 7 (35) | 1 (5) |
|
| 6 (30) | 1 (5) |
|
| 6 (30) | 0 (0) |
|
| 5 (25) | 2 (10) |
|
| 5 (25) | 1 (5) |
|
| 5 (25) | 0 (0) |
|
| 4 (20) | 0 (0) |
|
| 3 (15) | 1 (5) |
|
| 3 (15) | 0 (0) |
|
| 3 (15) | 0 (0) |
|
| 3 (15) | 0 (0) |
|
| 3 (15) | 0 (0) |
|
| 3 (15) | 0 (0) |
|
| 3 (15) | 0 (0) |
|
| 2 (10) | 1 (5) |
|
| 2 (10) | 0 (0) |
|
| 2 (10) | 0 (0) |
| Serious adverse events | ||
|---|---|---|
|
|
|
|
|
| Mucositis G3 | Possible |
|
| Sepsis G3 | Not related |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeuroendocrine Tumor Research Advances · Lung Cancer Research Studies · Tuberous Sclerosis Complex Research
Background
Emerging evidence has progressively challenged the concept of high-grade neuroendocrine neoplasm (NENs), and in responsive patients after first-line chemotherapy (CT) a standard approach has not been defined yet.1^,^2
Everolimus, an oral inhibitor of mammalian target of rapamycin (mTOR), could have a potential role in this setting although limited data are available.3
Trial information
MAVERIC was a multicenter, randomized, open-label, non-comparative, phase II clinical trial performed at 5 Italian institutions. The main inclusion criteria were an age of 18 years or older; histologically or cytologically confirmed, advanced, non-functioning, gastroenteropancreatic (GEP)-NEN) or large-cell neuroendocrine carcinoma (LCNEC) of lung origin with Ki-67 index ranging from 20% and 55% in accordance with the 2010 World Health Organization (WHO) classification4 (Figure 1); measurable target lesions according to the Response Evaluation Criteria in Solid Tumors (RECIST) guideline5; evidence of stable disease (SD), partial response (PR) or complete response after first-line CT according to clinical practice; Eastern Cooperative Oncology Group (ECOG) performance status ≤ 2; adequate organ function. The main exclusion criteria were well differentiated (WD) NEN with Ki67 < 20% or neuroendocrine carcinoma with Ki-67 > 55%; functional disease; concurrent mutually exclusive drugs with everolimus; presence of brain metastases. Histology performed before 2017 has been revised and classified according to the latest WHO classification by each reference center.
Flow chart of MAVERIC trial. Patients with metastatic GEP-NEN or LCNEC (Ki-67 20%-55%) according to the 2010 WHO classification achieving at least SD after first-line CT that were randomized (2:1) to everolimus 10 mg/day or observation. GEP-NEN, gastroenteropancreatic neuroendocrine neoplasm; LCNEC, lung large cell neuroendocrine carcinoma; SD, stable disease; RP, partial response; RC, complete response; R, randomization.
The study was done in accordance with Good Clinical Practice guidelines, the ethical principles of the Declaration of Helsinki, and local regulatory requirements. (EudraCT registration number is 2014-003951-72). All patients provided written informed consent before enrolment.
The primary endpoint was radiology-assessed progression-free survival (PFS), defined as the time between randomization and the first evidence of progressive disease (PD) or death, whichever occurred first. Documentation of PD was defined as per RECIST version 1.1 criteria5 based on investigator-reported evaluation. Overall survival (OS), defined as the time from randomization to the date of death due to any cause, and safety were the main secondary endpoints (Table 1).
Adverse events (AE) were assessed as per National Cancer Institute Common Terminology Criteria for AE (CTCAE) version 4.03.
Drug information
Patients were randomly assigned with a 2:1 ratio to maintenance therapy with everolimus 10 mg per day (experimental arm) or to observation (control arm) until progression or toxicity (Table 2).
Randomization was done using a centralized web-based system and allocation sequence was masked and generated at the Clinical Trials Coordinating Center, Oncology Unit, Careggi University Hospital (Florence, Italy).
The time between the last cycle of CT and randomization must not exceed 28 days.
All patients who underwent randomization were assessed for efficacy by radiological imaging every 12 weeks. Visits and study drug dispensation occurred in cycles, with each cycle equaling 28 days. Dose reductions and treatment interruption were allowed for patients who did not tolerate therapy or to manage adverse events that were judged to be related to study treatment. Two dose reductions were allowed: from 10 mg to 5 mg per day and, subsequently, to 5 mg every other day.
Palliative radiotherapy was allowed.
Statistical analysis
This is an open-label phase II study not powered for statistical comparison between experimental and observation arm. A control arm was included to provide contextual and calibration data due to lack of historical data for comparison in this subgroup of patients.
Survival analyses were descriptive. Kaplan–Meier methods were used to estimate median (m)PFS and OS with corresponding 95% CIs. No formal hypothesis testing between groups was performed. All statistical analyses were conducted using the R software v4.3.0 and the packages survival v3.5-5, survminer v0.4.9, and dplyr v1.1.2, and SAS (version 9.4).
Patient characteristics
From November 2015 to June 2022, 30 patients with metastatic, non-functioning, NEN from GEP or lung primary sites and Ki-67 index 20%-55% were enrolled and randomly assigned to everolimus (20 patients) or observation (10 patients) (Figure 2). One patient was not included in the analysis for protocol deviation having a Ki-67 > 55%. Patients’ baseline characteristics are reported in Table 3. The primary site was GEP in 52%, mostly pancreatic, while 48% of lung origin that resulted equally distributed in the 2 arms. WD neuroendocrine tumors (NETs) were more common in the experimental arm (85% of patients) than in the control arm (55%). Prior first-line CT was platinum-based in 13 patients and non-platinum-based in 16 patients, with 4 median number of CT cycles in both arms. A PR was achieved in 67% of patients in the control arm, with an equal distribution among platinum and non-platinum-based CT and in 35% of patients in the experimental arm, 60% with non-platinum-based CT.
Consort flow diagram.
Primary assessment method
After a median follow-up of 80 months, mPFS was 11.8 months (95% CI 4.1-22.8) in the experimental and 1.8 months (95% CI 0.9-19.9) in the control arm (Figure 3 and Table 4). MOS were 38.3 months (95% CI 14.9-59.6) and 38.2 months (95% CI 3.1-64.5), respectively.
Kaplan–Meier curves and risk table of progression-free survival (PFS) in the control and treatment arm. NA, not reached.
In the 13 GEP-NEN patients treated with everolimus, the mPFS was 19.9 months (95% CI 11.0-24.4) and the mOS 48.1 months (95% CI 34.5-NA). Among the 7 patients with LCNEC, mPFS was 7.8 months (95% CI 2.0-29.0) (Figure 4) and mOS 14.6 months (95% CI 3.8-59.6).
Kaplan–Meier curves and risk table of progression-free survival (PFS) in the GI and lung subgroups of the treatment arm. GI, gastrointestinal; NA, not reached.
GEP-NENs specimens were reviewed by an expert pathologist in accordance with the 2017 WHO classification and 86% were reclassified as NET G3. The subgroup of 11 patients with GEP NET G3 treated with everolimus showed an mPFS of 19.9 months (95% CI 11.4-24.4) and mOS of 48.1 months (95% CI 38.3-67.8) (Figure 5).
Kaplan–Meier curves and risk tables of progression-free survival (PFS) (A) and overall survival (OS) (B) in the GI NET G3 population of the treatment arm. GI, gastrointestinal; NET, neuroendocrine tumors; NA, not reached.
General toxicity profile
Drug-related AEs in the experimental arm were in line with the known safety profile of everolimus and were mostly grade (G) 1 or 2 (Table 5). The most common AEs reported in patients receiving everolimus were mucositis, dyslipidemia, fatigue, pneumonitis and peripheral edema. Globally, 14 patients (70%) experienced a G3 AE and 2 of them were classified as serious AE with consequent discontinuation of treatment (Table 6). In 65% of patients, at least one dose reduction was needed. No G4 AEs occurred.
Discussion
The MAVERIC trial focused on a particular subgroup of high-grade NENs, with Ki-67 between 20% and 55%, including both well and poorly differentiated NENs defined according to the WHO 2010 classification criteria.
Current guidelines indicate CT as first-line treatment in high-grade NENs although evidence remains limited to specific schedule or duration, particularly for advanced GEP NET G3.6 Similarly, clinical data on everolimus in this setting are also limited. The association of TEM and everolimus was assessed as upfront therapy in GEP-NET G3 and GEP-NEC reporting an mPFS of 12.6 months and 3.4 months, respectively, which are consistently in line with MAVERIC efficacy outcomes, with a comparable toxicity profile.7
Notably, unlike Morken’s study, MAVERIC trial evaluated everolimus as a maintenance treatment following first-line CT, which, to our knowledge, represents the first in this distinct patient population. Everolimus prolonged PFS suggesting that a biological therapy could replace CT to keep a longer tumor response.
The apparent lack of OS benefit with everolimus in our study (ie, 38.3 vs 38.2 months) may reflect the high percentage of patients receiving second-line therapy in the control arm at the time of progression (7/9 patients, 78%). Considering the high-grade lung NEN, the further rarity of this subtype implies even more uncertainties. In our trial, 7 patients in the everolimus arm had LCNEC with an mPFS of 7.8 months and mOS of 14.6 months, confirming the worse outcome of this population. Recently, a retrospective series of carcinoids with Ki-67 > 20% has reported a favorable response to both temozolomide (n = 12, PFS 6.8 months) and everolimus (n = 8, PFS 12.1 months) regimes, indirectly supporting our findings.8
Considering the OS in high-grade NEN, the present cohort shows a prolonged mOS which results almost doubled compared to literature data.9^,^10 This survival gap could be affected by several factors, such as the good baseline prognostic characteristics, the restricted inclusion criteria, and the use of different treatment lines after disease progression.
In our study, several limitations should be recognized. Considering the rarity of these neoplasms, the enrollment lasted almost 7 years, and different primary sites were included; the WHO classification has been updated during the accrual period and consequentially most of LC-NECs (9/14) were retrospectively reclassified as WD. In WD lung or GI NETs, although limited to progressive disease, the activity of everolimus has been also reported in RADIANT-4, which is consistent with our results.3 Moreover, during study’s accrual, first-line 177Lu-DOTATATE data for high G2 and G3 SSTR+ GEP NETs was not available.11 Despite the reported limitations this study discloses several strengths: the therapeutic approach has shed light on a specific sequential treatment; although small, the population sample represents an authentic overview of advanced NEN, joining 2 different aggressive cohorts of high-grade lung and GEP-NEN, to explore the therapeutic benefits of the same treatment scheme.
In conclusion, the MAVERIC trial is a hypothesis generating study, showing that everolimus may be effective and safe in patients with advanced non-functional GEP-NEN and LCNEC with a Ki-67 index ranging from 20% and 55% as maintenance therapy after a first-line CT. This strategy was particularly effective for the GEP-NEN patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Milione M , Maisonneuve P, Spada F, et al. The clinicopathologic heterogeneity of grade 3 gastroenteropancreatic neuroendocrine neoplasms: morphological differentiation and proliferation identify different prognostic categories. Neuroendocrinology. 2017;104:85-93.26943788 10.1159/000445165 · doi ↗ · pubmed ↗
- 2Zatell MC , Guadagno E, Messina E, Lo Calzo F, Faggiano A, Colao A; NIKE Group. Open issues on G 3 neuroendocrine neoplasms: back to the future. Endocr Relat Cancer. 2018;25:R 375-R 384.29669844 10.1530/ERC-17-0507 · doi ↗ · pubmed ↗
- 3Yao JC , Fazio N, Singh S, et al.; RAD 001 in Advanced Neuroendocrine Tumours, Fourth Trial (RADIANT-4) Study Group. Everolimus for the treatment of advanced, non-functional neuroendocrine tumours of the lung or gastrointestinal tract (RADIANT-4): a randomised, placebo-controlled, phase 3 study. Lancet. 2016;387:968-977.26703889 10.1016/S 0140-6736(15)00817-XPMC 6063317 · doi ↗ · pubmed ↗
- 4Niederle MB , Hackl M, Kaserer K, Niederle B. Gastroenteropancreatic neuroendocrine tumours: the current incidence and staging based on the WHO and European Neuroendocrine Tumour Society classification: an analysis based on prospectively collected parameters. Endocr Relat Cancer. 2010;17:909-918. 10.1677/ERC-10-015220702725 · doi ↗ · pubmed ↗
- 5Ruchalski K , Braschi-Amirfarzan M, Douek M, et al. A primer on RECIST 1.1 for oncologic imaging in clinical drug trials. Radiol Imaging Cancer. 2021;3:e 210008.33988475 10.1148/rycan.2021210008 PMC 8183261 · doi ↗ · pubmed ↗
- 6Pavel M , Öberg K, Falconi M, et al.; ESMO Guidelines Committee. Gastroenteropancreatic neuroendocrine neoplasms: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2020;31:844-860.32272208 10.1016/j.annonc.2020.03.304 · doi ↗ · pubmed ↗
- 7Morken S , Langer SW, Sundlöv A, et al. Phase II study of everolimus and temozolomide as first-line treatment in metastatic high-grade gastroenteropancreatic neuroendocrine neoplasms. Br J Cancer. 2023;129:1930-1939.37872405 10.1038/s 41416-023-02462-0PMC 10703888 · doi ↗ · pubmed ↗
- 8Rubino M , Scoazec JY, Pisa E, et al. Lung carcinoids with high proliferative activity: further support for the identification of a new tumor category in the classification of lung neuroendocrine neoplasms. Lung Cancer. 2020;148:149-158.32916569 10.1016/j.lungcan.2020.08.001 · doi ↗ · pubmed ↗