Community health assets and refugee wellbeing: Qualitative evidence across mental health, disability inclusion, end-of-life care, and women’s health – A global scoping review
Sileshi Demelash Sasie, Melkamu Asrat Alava, Lensa Fekadu, Hailemichael Wasye Misganaw, Tigist Ali Gebeyehu, Neima Zeynu Ali, Sisay Temesgen Dema, Melkamu Abte Afele, Zenebech Mamo Argaw, Jasmin Lilian Diab, Jasmin Lilian Diab, Jasmin Lilian Diab

TL;DR
This review explores how community health assets support refugee wellbeing in mental health, disability inclusion, women's health, and end-of-life care.
Contribution
It synthesizes fragmented qualitative evidence across four domains to identify common barriers and effective strategies for refugee health interventions.
Findings
Common barriers include stigma, gender-based violence, and limited access to specialized services.
Effective strategies include peer-led support and culturally concordant providers.
Trust and culturally safe engagement are central to successful interventions.
Abstract
Refugee populations face heightened and intersecting vulnerabilities across mental health, disability inclusion, women’s health, and end-of-life and palliative care, shaped by displacement, trauma, legal precarity, and systemic marginalization. Although community-centered approaches are increasingly recognized as critical for addressing these challenges, qualitative evidence on how community health assets support refugee wellbeing remains fragmented across domains. This scoping review aimed to map and synthesize qualitative evidence on community-based health interventions for refugee populations across four thematic areas: mental health, disability inclusion, women’s health, and end-of-life and palliative care. The review followed Joanna Briggs Institute methodology and was conducted in accordance with PRISMA-ScR guidance. A comprehensive search of PubMed, Scopus, and Web of Science…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
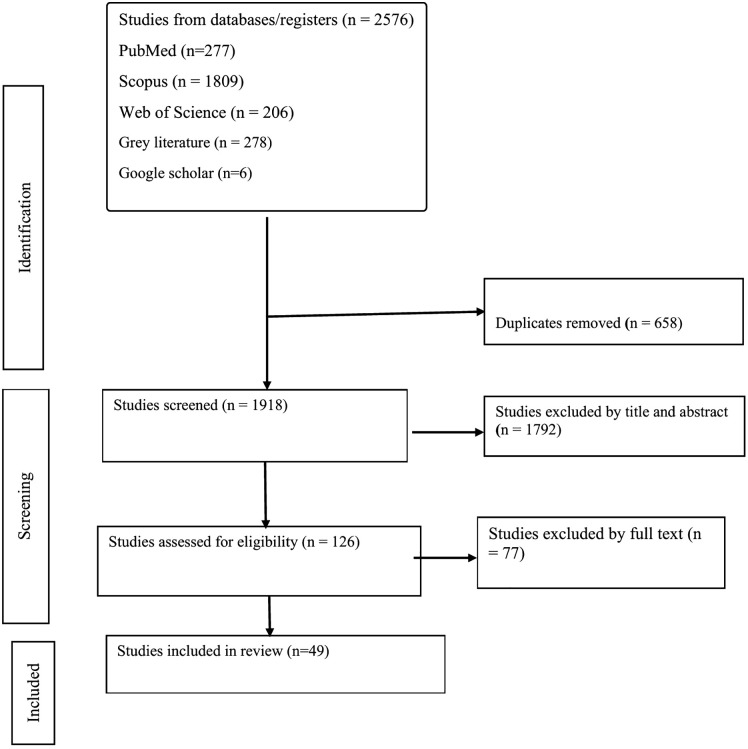 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigration, Health and Trauma · Palliative Care and End-of-Life Issues · Homelessness and Social Issues
1. Background
Globally, millions of forcibly displaced individuals are exposed to profound and largely preventable health risks [1,2]. Refugees, asylum seekers, and internally displaced persons (IDPs) represent legally distinct groups, yet they share a common reality of disrupted lives and fragile health. Refugees are individuals who have crossed an international border because of a well-founded fear of persecution and have been granted protection under the 1951 Refugee Convention and related instruments [3,4]. Asylum seekers are people who have sought this protection but whose claims remain pending, often leaving them in prolonged legal uncertainty and with limited access to essential services [3,5,6]. Internally displaced persons, by contrast, flee similar threats of conflict, violence, or disaster but remain within their country’s borders, where protection and assistance depend largely on domestic systems and the non-binding Guiding Principles on Internal Displacement [4,7,8].
Behind these legal categories are millions of individuals facing profound and preventable health risks. Across settings, forcibly displaced populations experience higher burdens of physical illness, psychological distress, and unmet healthcare needs than surrounding host communities [5–9]. IDPs, in particular, often endure even worse outcomes than refugees, reflecting sudden loss of livelihoods, separation from family networks, and severely constrained access to services [5]. Common barriers to care include administrative exclusion, fear of deportation, lack of documentation, language and cultural obstacles, discrimination, and unaffordable costs [9–12]. These challenges restrict access to primary care, mental health services, sexual and reproductive healthcare, and preventive programs, and are further intensified by overcrowded living conditions, poor water and sanitation, and insecure work [9–11,13].
The scale of this crisis is unprecedented. By 2024, more than 110 million people worldwide were forcibly displaced, with the majority hosted in low- and middle-income countries (LMICs) whose health systems are often overstretched and under-resourced [14,15]. Women and girls nearly half of the global refugee population face additional layers of vulnerability, including gender-based violence, limited reproductive health services, and intersecting social and economic inequalities [16–18]. Across all groups, experiences of violence, loss, and uncertainty accumulate over time, contributing to high levels of depression, anxiety, post-traumatic stress disorder, and other mental health conditions [3–5,13,19]. Recent global shocks, such as the COVID-19 pandemic, have further deepened these inequities by disrupting services, eroding livelihoods, and widening information gaps among displaced communities [10,20].
In response to these challenges, important initiatives have emerged. Asset-Based Community Development (ABCD) approaches in countries such as the United Kingdom and Australia have demonstrated the value of building on community strengths, social networks, and local leadership to support refugee wellbeing [21–23]. Culturally adapted mental health programs, early psychosocial screening, inclusive maternal health services, and digital health tools have shown promise in diverse contexts [14,24,25]. Participatory models such as co-designed services, peer-led networks, and community needs assessments are increasingly recognized as essential for ensuring that interventions are relevant, trusted, and sustainable [23,26,27]. Intersectoral frameworks, including the National Health Service (NHS) Inclusion Health model, illustrate how coordinated action across health, social services, and community organizations can help reduce structural barriers to care [22,28].
Yet progress remains fragmented and uneven. Much of the available research and program experience is concentrated in high-income countries, limiting its applicability to LMICs where most displaced people live [23,29,30]. Studies frequently address single issues in isolation, with little attention to the ways mental health, disability, gender, and age intersect in real lives. Groups with some of the greatest needs people with disabilities, older adults, those requiring palliative care, and adolescent girls are often underrepresented [29–32]. Important areas such as maternal mental health, disability-inclusive services, and end-of-life care remain insufficiently explored. Moreover, many interventions lack grounding in implementation science frameworks and rarely assess long-term outcomes or system-level enablers [33]. A persistent absence of meaningful refugee participation in research and program design further limits cultural appropriateness and practical impact [9,34–36].
Qualitative evidence is uniquely positioned to address these shortcomings. By capturing lived experiences, community perspectives, and the everyday realities of service delivery, qualitative studies illuminate dimensions of access, trust, and dignity that quantitative indicators alone cannot reveal [37,38]. However, this evidence remains scattered across separate thematic silos, with few efforts to synthesize insights across domains.
This scoping review seeks to close that gap. For the first time, it brings together qualitative evidence across four critical areas of refugee health mental health, disability inclusion, women’s health, and end-of-life and palliative care. By integrating findings from diverse settings and perspectives, the review identifies shared barriers, practical facilitators, and cross-cutting lessons for implementation. In alignment with World Health Organization (WHO) and United Nations High Commissioner for Refugees (UNHCR) priorities for equity-oriented and culturally responsive care [39], the review aims to generate practical and actionable insights to inform inclusive, participatory, and context-sensitive interventions for displaced populations worldwide.
2. Methods
2.1 Ethics statement
This study is a scoping review of peer-reviewed, publicly available literature and did not involve the collection of primary data or direct engagement with human participants. In accordance with international ethical guidelines for secondary research, institutional ethical approval and informed consent were not required.
2.2 Study design and conceptual framework
This review focused exclusively on qualitative studies to capture context-sensitive evidence on refugee experiences, perceptions, and priorities that are not readily addressed through quantitative designs [37,40]. Qualitative research is particularly valuable for understanding the cultural, social, and systemic factors that shape access to care, service acceptability, and implementation of health interventions in complex displacement settings.
The review was conducted in accordance with the Joanna Briggs Institute (JBI) methodology for scoping reviews, which provides a structured and transparent approach for mapping the breadth and depth of existing research [41]. Methodological guidance from Arksey and O’Malley [42] and Levac et al. [43] was applied to strengthen rigor in study selection, data extraction, and synthesis processes. Reporting of the review followed the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) guideline [44].
The synthesis was further informed by established implementation science frameworks. The Consolidated Framework for Implementation Research (CFIR) and Proctor’s implementation outcomes were used to guide interpretation of findings and to identify determinants of intervention feasibility, acceptability, and sustainability [29,37,38].
2.3 Objectives and research questions
The objective of this scoping review was to systematically map and synthesize qualitative evidence on implementation experiences, challenges, and outcomes of health interventions for refugee and forcibly displaced populations across four priority domains: mental health, disability inclusion, women’s health, and end-of-life/palliative care.
The CFIR and Proctor’s Implementation Outcomes Framework guided the identification of implementation determinants, strategies, and reported outcomes. Research questions were developed in alignment with the Population–Concept–Context (PCC) framework, with the Population (P) fixed as refugee and forcibly displaced populations. The Concept and Context elements varied across questions, as shown in Table 1.
Table 1: Research Questions Aligned with the PCC Framework.
2.4 Eligibility criteria
The scope of eligible studies was structured using the Population–Concept–Context (PCC) framework recommended for scoping reviews. This framework guided the formulation of inclusion and exclusion criteria and ensured alignment between the review objectives and study selection processes. The PCC parameters defining the scope of this review are summarized in Table 2.
Table 2: PCC Framework Defining the Scope of the Scoping Review.
Inclusion criteria.
Study design: Qualitative studies (e.g., interviews, focus groups, ethnography, phenomenology, participatory co-design) reporting primary data.Population: Human participants who are refugees, asylum seekers, or internally displaced persons (IDPs).Focus: Addresses at least one of the four focal domains mental health, disability inclusion, end-of-life/palliative care, or women’s health.Child and adolescent populations: Studies involving children and adolescents were eligible when they addressed issues directly relevant to one of the four focal domains (for example, mental health of refugee youth or disability-related services for children). Broader pediatric health topics not linked to these domains were considered outside the scope of this review. Publication type:
- ◦ Peer-reviewed journal articles published between January 2010 and December 2025, in English.
- ◦ Grey literature outputs (e.g., reports, policy documents, program evaluations, and guidelines from international organizations, NGOs, and government bodies) that present primary qualitative data. Accessibility: Full-text documents available at the time of screening
Exclusion criteria.
Quantitative or mixed-methods studies without disaggregated qualitative findings.Studies not centered on forcibly displaced populations.Grey literature without methodological transparency (e.g., blogs, opinion pieces, media reports) and non-peer-reviewed conference abstracts.
2.5 Information sources and search strategy
A comprehensive search strategy was developed to identify both peer-reviewed and grey literature relevant to the review objectives. For the peer-reviewed component, three bibliographic databases PubMed, Web of Science, and Scopus were systematically searched. Search strategies combined controlled vocabulary (e.g., MeSH in PubMed) with free-text terms reflecting four core concepts: displaced populations, focal health domains, qualitative methods, and implementation. Boolean operators (AND/OR) were applied, and search fields were adapted for each database, including TITLE-ABS-KEY in Scopus and TS = Topic in Web of Science.
To complement the academic search, targeted strategies were applied to global repositories and organizational portals in order to capture relevant grey literature. Sources included the WHO Institutional Repository for Information Sharing (IRIS), the World Bank Documents Portal, UNHCR publications, and International Organization for Migration (IOM) resources. Focused Google site searches were also conducted for humanitarian organizations such as United Nations Children’s Fund (UNICEF), Médecins Sans Frontières (MSF), and Save the Children. These searches incorporated refinements such as document-type keywords (e.g., report, framework, guideline, policy) and file-type filters (filetype:pdf) to maximize relevance and precision.
Additional measures were undertaken to ensure completeness and reduce the risk of missing eligible studies. Google Scholar was searched systematically using the same conceptual terms, and records were screened sequentially until thematic saturation was reached, which corresponded to approximately the first 200 results. Citation tracking was also employed: backward citation tracking involved screening the reference lists of included studies, while forward citation tracking used the Google Scholar “Cited by” function to identify more recent relevant works. The complete search strategies for all databases and repositories, including Boolean strings, refinements, and applied filters, are provided in S1 Table.
2.6 Study selection
All identified records were imported into EndNote, where duplicates were removed prior to screening. The selection process was carried out in two phases: an initial title and abstract screening followed by full-text review. Two reviewers (SDS and FMA) independently assessed all records against the predefined eligibility criteria. To ensure consistency, a calibration exercise was conducted on a random sample of ten records at the title and abstract stage. Reviewers agreed on nine of the ten records (90% raw agreement), and Cohen’s kappa [45] was calculated at 0.82, indicating substantial agreement according to the benchmarks established by Landis and Koch [46].
Following calibration, the full screening process proceeded independently. Any discrepancies between reviewers were resolved through discussion, and unresolved cases were adjudicated by a third reviewer (HWM). The selection process, including reasons for exclusion at each stage, is detailed in the PRISMA-ScR flow diagram (Fig 1).
PRISMA flow diagram of the study selection process.
2.7 Data extraction
Data extraction was conducted using a structured and pre-defined framework developed specifically for this scoping review. The framework was designed to capture key methodological characteristics, contextual information, and implementation-relevant evidence in a consistent and reproducible manner across all eligible studies.
For each included study, data were systematically extracted using the following fields: reference (authors and year of publication), country or setting, thematic domain, primary population, age group, gender composition, pertinent findings, study-reported limitations, and authors’ recommendations. These variables were selected to support transparent description of study characteristics and to enable consistent synthesis across the four thematic domains of the review.
Primary population was coded according to the target group described in each study, including refugees, asylum seekers, internally displaced persons, or mixed populations. Age was categorized based on the descriptors used by study authors (e.g., children, adolescents, adults, older adults, or mixed-age groups). Gender composition was recorded as women-only, men-only, mixed-gender, or not reported. Geographic setting was captured at the country or regional level as specified in the original publication.
Data extraction was performed independently by two reviewers (SDS and FMA) using a standardized extraction template. Discrepancies between reviewers were resolved through discussion, and when consensus could not be reached, a third reviewer (HWM) adjudicated the final decision. All extracted data were entered into a centralized database to ensure uniformity and to support subsequent synthesis.
For each included study, data were systematically extracted using a standardized set of variables designed to capture study characteristics and relevant qualitative information. The complete list of extraction variables is provided in S2 Table.
2.8 Data synthesis
Data synthesis was conducted using a structured thematic synthesis approach consistent with the method described by Thomas and Harden [47]. The process combined inductive coding of qualitative data with deductive organization using established implementation science frameworks. All information extracted in the “pertinent findings” field was first reviewed in its original qualitative form and coded inductively to capture key concepts, processes, and contextual factors described in each study.
Following inductive coding, the resulting codes were organized deductively using the Consolidated Framework for Implementation Research (CFIR) domains [48] to classify implementation determinants and Proctor’s implementation outcomes [49] taxonomy to categorize reported outcomes. This dual-framework approach provided a consistent analytic structure for organizing evidence on intervention characteristics, contextual influences, and implementation processes across diverse study settings.
Synthesis was undertaken in two sequential stages. In the first stage, coded data were organized and analyzed within each predefined thematic domain to generate domain-specific themes. In the second stage, a cross-domain synthesis was conducted to integrate evidence across domains and to identify commonalities and differences in implementation experiences.
Studies addressing more than one thematic domain were coded under all applicable domains during data extraction. For within-domain analyses, findings from these studies were included in each relevant domain. However, during cross-domain synthesis and any aggregate summaries, each study was treated as a single analytic unit and counted only once, regardless of the number of domains to which it contributed.
Demographic variables specified for inclusion in the synthesis were age group, gender composition, and geographic setting. Procedures were established to record these variables exactly as reported in the primary studies, using the categories and descriptors provided by the original authors. Where any demographic information was absent from a publication, it was to be coded as “not reported” rather than inferred. These rules were applied consistently to maintain methodological transparency.
Synthesized data were organized using narrative summaries and structured analytic matrices to enable systematic comparison across studies and thematic domains. These matrices were used to collate coded information, map implementation determinants and outcomes, and facilitate consistent integration of qualitative evidence.
2.9 Quality appraisal
To assess methodological rigor, all included studies were appraised using the Critical Appraisal Skills Programme (CASP) Qualitative Studies Checklist [50]. This checklist evaluates ten domains, including clarity of the research aim, appropriateness of qualitative methods, justification of research design, recruitment strategies, alignment between data collection and study objectives, researcher reflexivity, ethical considerations, rigor of data analysis, clarity of findings, and overall research value.
Although formal quality assessment is not a mandatory component of scoping reviews, the inclusion of CASP provided a structured appraisal of methodological strengths and limitations across studies. In accordance with established scoping review methodology, quality appraisal was conducted to describe the methodological characteristics of the evidence base rather than to exclude studies on the basis of quality [47,51].
3. Results
3.1 Study selection summary
The study selection process is presented in Fig 1 (PRISMA-ScR flow diagram). The initial database search identified 277 records from PubMed, 1,809 from Scopus, and 206 from Web of Science, yielding a total of 2,292 records. An additional 278 records were retrieved from grey literature sources and 6 from Google Scholar, resulting in 2,576 records overall. After removal of 658 duplicates, 1,918 unique records remained for title and abstract screening. Of these, 1,793 were excluded, leaving 126 articles for full-text review. Following detailed assessment, 77 articles were excluded, resulting in 49 studies that met the inclusion criteria and were retained for the final scoping review (Fig 1).
3.2 Study characteristics
The 49 included studies provided a broad but unevenly distributed body of qualitative evidence across the four domains of mental health, disability inclusion, women’s health, and end-of-life and palliative care. Collectively, the studies spanned diverse contexts, including high-income resettlement countries, low-resource humanitarian settings, and transnational migration environments. Geographically, Europe (n = 14) and North America (n = 13) contributed the largest share of studies, with representation across all four domains. Africa (n = 6) and the Middle East (n = 6) offered moderate coverage, each encompassing at least three domains. Oceania (n = 6) was represented primarily in women’s health and end-of-life research, with no studies addressing disability inclusion. Asia (n = 3) contributed exclusively to the end-of-life domain, while South America (n = 1) was represented by a single study focused on disability inclusion.
Study population characteristics varied across the included literature. Demographic reporting was inconsistent, with most studies focusing on adult populations and a smaller subset addressing children, youth, or older adults. Thirteen studies examined women-only samples, particularly within the women’s health and gender-sensitive mental health domains, while others included mixed-gender populations or did not clearly specify gender composition. The evidence base reflects diverse geographic regions, including Europe, North America, Africa, the Middle East, Asia, and Australia.
Mental health studies (n = 12) frequently examined culturally adapted psychosocial interventions, stigma reduction strategies, faith-based supports, and digital tools intended to improve service accessibility and acceptability. Disability inclusion research (n = 11) often focused on enhancing accessibility for refugees with disabilities, with particular emphasis on inclusive program design, early developmental screening, and intersectional approaches addressing both gender- and disability-related needs. Women’s health studies (n = 9) highlighted culturally tailored maternal and perinatal care, peer-led health promotion initiatives, faith-integrated mental health interventions, and community-led service models aimed at improving engagement and trust in healthcare systems. End-of-life and palliative care studies (n = 17) explored dignity-preserving models of care, the role of family and community engagement, integration with primary healthcare, and context-specific approaches to service delivery in both camp-based and urban host settings.
Across all four domains, studies reported recurring patterns related to cultural competence, community engagement, and participatory approaches. Frequently reported constraints included language and communication challenges, stigma, discriminatory practices, restrictive policy environments, and fragmented service delivery systems. Many studies also documented practical recommendations to address these challenges, including expansion of peer support networks, cross-sectoral collaboration, culturally and linguistically appropriate provider training, and alignment of services with the social and cultural contexts of refugee populations. A detailed synthesis of individual study characteristics, demographic information, key findings, limitations, and recommendations is presented in S3 Table.
3.3 Quality appraisal of included studies
All 49 qualitative studies included in the review were appraised using the CASP Qualitative Studies Checklist, in line with scoping review methodology, which emphasizes mapping the evidence base rather than excluding studies on the basis of quality. Overall, most studies demonstrated clearly articulated aims, appropriate use of qualitative methodology, and data collection methods that were consistent with their objectives.
However, variability was observed across several critical domains. Recruitment strategies were frequently insufficiently described [52–54], limiting transparency around sampling processes and the potential for bias. Ethical considerations were also underreported in many cases; several studies failed to specify informed consent procedures or safeguards for vulnerable populations, particularly displaced women, persons with disabilities, and survivors of trauma [55,56].
A recurring limitation across the dataset was the lack of reflexivity. More than half of the studies provided minimal or no discussion of researcher positionality or the dynamics between researchers and participants, despite the importance of such considerations in refugee health research [57–59]. In addition, analytic rigor varied considerably. Some older and even more recent studies [60,61] presented only surface-level descriptions of data analysis, with limited detail on coding strategies, triangulation, or validation processes.
Nevertheless, the majority of studies offered clear statements of findings and contributed valuable insights, with several [58,62–64] demonstrating consistently high methodological quality across appraisal domains. Collectively, these results highlight both the strengths of the existing evidence and the key areas requiring improvement in future qualitative research particularly enhanced transparency in ethical reporting, stronger reflexivity, and more robust descriptions of analytic processes. A summary of quality appraisal findings is provided in S4 Table.
3.4 Domain-level findings: refugee health interventions across four contexts
Evidence on refugee health interventions clustered around four prominent domains: mental health, disability inclusion, women’s health, and end-of-life/palliative care. These domains capture intersecting determinants of health and align with global priorities for displaced populations. Across domains, mapping interventions onto CFIR constructs and Proctor’s outcomes revealed consistent challenges, including structural exclusion within the Outer Setting, organizational and infrastructural gaps within the Inner Setting, and the persistent need for participatory processes to ensure that interventions are contextually adapted to refugee realities. The synthesis below presents domain-specific findings while identifying recurrent patterns across interventions that directly address the guiding questions of this review.
3.4.1 Mental health.
Twelve studies examined refugee mental health interventions, with most focusing on psychosocial support, trauma recovery, stigma reduction, and community-based care [52–55,65–71]. Intervention models encompassed culturally congruent psychosocial programs, faith-integrated supports, stigma-sensitive digital tools, and trauma-informed approaches [53–55,66]. Collectively, the evidence highlights that intervention effectiveness was contingent on the alignment between program design and the broader socio-political and organizational contexts in which refugees were situated.
Across CFIR domains, the Outer Setting exerted the strongest influence. Legal precarity, asylum process stress, unstable housing, and stigma systematically undermined service continuity [52,57]. These constraints help explain why even well-adapted psychosocial interventions often struggled in the absence of broader protections. At the Inner Setting level, dependence on NGO-based services, weak referral networks, and under-resourced health facilities limited integration into host-country systems [65,70]. Programs that incorporated cultural competency training for general practitioners and frontline providers reported greater feasibility and adoption [70,71], underscoring how organizational readiness interacts with provider competence to shape implementation outcomes.
Characteristics of individuals were also critical. Distrust, shame, and cultural taboos around mental illness discouraged service uptake [53–55], while resilience and faith-based coping facilitated engagement [54,68]. Provider cultural competence emerged as a key mediator: interventions faltered where providers lacked cross-cultural awareness but flourished when training and collaboration helped bridge cultural divides [70].
Process strategies such as participatory co-design, peer-led delivery, and community involvement consistently enhanced intervention acceptability and contextual fit [67,71]. Digital interventions revealed a nuanced pattern: stigma-aware, human-centered approaches increased reach and engagement [55], but digital divides stemming from limited internet access, literacy barriers, and trust concerns restricted feasibility in many settings.
When mapped to Proctor’s outcomes, interventions were consistently rated acceptable and appropriate when culturally and linguistically tailored [66,68]. Feasibility and adoption improved when programs employed community facilitators and culturally competent staff [67,70], while fidelity was reinforced by embedding cultural sensitivity into implementation protocols. However, penetration and sustainability were rarely achieved, as these outcomes were contingent on integration with broader supports such as housing, legal aid, and policy reforms [57,65].
Reported outcomes included reductions in psychological distress and trauma symptoms [66], strengthened coping and resilience [54,68], improved help-seeking and social connectedness [52,67], enhanced cultural competence among providers [70,71], and symptom reduction through tailored digital programs [55]. Despite these promising findings, few studies evaluated long-term continuity, highlighting a critical evidence gap regarding sustainability and systemic integration (Table 3).
Table 3: Summary of qualitative evidence on mental health interventions for refugee populations mapped to CFIR constructs, Proctor’s implementation outcomes, barriers, facilitators, and reported outcomes.
3.4.2 Disability inclusion.
Eleven studies explored disability-inclusive interventions for refugees with physical, sensory, or cognitive impairments, often intersecting with age, gender, and trauma histories. Interventions included accessibility audits, inclusive health outreach, community-based rehabilitation, and peer-led advocacy. While these programs addressed multiple CFIR domains and Proctor outcomes, the synthesis shows that most operated as corrective measures within systems marked by structural neglect, highlighting persistent gaps in disability recognition, resource allocation, and policy integration.
Outer Setting determinants were particularly pronounced. Policy gaps, unsafe migration conditions, entrenched stigma, and systemic neglect of disability needs consistently undermined implementation [56,72,73]. These external barriers disproportionately affected refugee women with disabilities, who frequently faced intersectional discrimination [56]. Nonetheless, promising adaptations emerged: coordinated disability service models along migration routes [73] and tailored -prevention programs for persons with communication disabilities [74] demonstrated how context-specific approaches, when aligned with humanitarian or policy frameworks, could mitigate risks.
At the Inner Setting level, constraints reflected inadequate provider training, inaccessible infrastructure, and weak intersectoral coordination [62,75]. Interventions struggled where organizations lacked adaptive facilities or case management systems. By contrast, inclusive classroom models in Germany illustrated how organizational culture, teacher preparedness, and peer inclusion could significantly enhance adoption [63]. These variations underscore that organizational readiness is not merely a supportive factor but a determinant of feasibility and sustainability.
Individual characteristics and process strategies also shaped outcomes. Provider competence, cultural sensitivity, and advocacy skills were critical for engagement, while refugees’ resilience and agency contributed to uptake [76,77]. Programs incorporating participatory design, caregiver engagement, and partnerships with disability organizations achieved stronger contextual fit and legitimacy [63,77]. Peer networks and leadership initiatives particularly those led by women with disabilities were transformative, enhancing both acceptability and social participation [72].
Mapped to Proctor’s outcomes, interventions demonstrated high appropriateness when grounded in inclusive communication and intersectional design [74,77]. Acceptability improved through peer support and culturally adapted screening [76]. Feasibility was frequently undermined by inaccessible facilities and fragmented services [62,75], though community navigation and teacher training enhanced adoption [63,76]. Fidelity was best maintained when inclusion principles were embedded into program protocols, while penetration and sustainability remained limited, dependent on systemic integration and stable funding. Reported impacts included earlier developmental screening [76], improved caregiver coping [78], increased reporting of gender-based-violence (GBV) [74], and enhanced educational and social participation [63,72].
Barriers were consistently systemic and multi-level, including inaccessible infrastructure, lack of assistive devices, transportation challenges, siloed disability services, migration hazards, and institutional gatekeeping [62,73,75]. Facilitators included interpreter provision, inclusive communication, awareness campaigns, and advocacy-led program design [74,77]. Cross-sector collaboration particularly between humanitarian and medical actors and empowerment initiatives further supported uptake and sustainability [63,72].
Taken together, these findings suggest that while disability-inclusive interventions generate meaningful gains across health, education, and protection sectors, they remain structurally fragile. Success depended less on the specific features of individual programs than on their ability to challenge systemic neglect and foster sustained cross-sector collaboration. The evidence underscores a persistent gap between short-term adaptation and long-term institutional reform, pointing to the need for systemic accountability and durable inclusion mechanisms within both humanitarian and host-country systems (Table 4).
Table 4: Summary of qualitative evidence on disability inclusion interventions for refugee populations mapped to CFIR constructs, Proctor’s implementation outcomes, barriers, facilitators, and reported outcomes.
3.4.3 Women’s health.
Nine studies addressed women’s health interventions among refugee populations, focusing on maternal health, reproductive autonomy, perinatal care, and GBV prevention. Intervention designs included culturally tailored maternal health models, integrated antenatal services, peer-led health promotion, and faith-based approaches.
Outer Setting determinants reported across studies included socio-economic hardship, restrictive policies, gendered stigma, and fragmented maternal health services [80,81]. These factors were associated with reduced continuity of care and lower service utilization, particularly among undocumented women and those in transit. Some studies reported that programs linking health services with social supports, such as housing assistance and NGO partnerships, improved access [80].
At the Inner Setting level, organizational capacity and provider preparedness varied. Facilities lacking gender-sensitive infrastructure or staff trained in culturally responsive care were associated with disengagement [81,82]. In contrast, programs employing female providers, peer navigators, and community health workers were reported as demonstrating higher feasibility and adoption [83,84]. Most initiatives were described as pilot projects and were not integrated into national maternal health frameworks.
Individual characteristics and process strategies influenced implementation. Several studies described refugee women’s resilience and leadership as facilitating program uptake, particularly in peer-led and co-leadership models [58,81]. In contrast, mistrust, fear, and digital exclusion limited engagement [58]. Participatory co-design and community leadership were reported as enhancing contextual fit, while digital interventions produced mixed results due to connectivity and literacy challenges [58].
Across Proctor’s outcomes, acceptability and appropriateness were reported as higher when services were linguistically and culturally tailored [82,83]. Feasibility and adoption improved with peer involvement and continuity of care [83,84]. Penetration and sustainability were less frequently reported; stand-alone pilots often ended once external support was withdrawn, whereas integration with policy frameworks and partnerships was associated with greater continuity [80,81].
Overall, the nine studies reported outcomes such as increased service uptake, improved engagement with providers, enhanced trust through peer-led initiatives, and context-specific adaptations to maternal and reproductive health services (Table 5).
Table 5: Summary of qualitative evidence on women’s health interventions for refugee populations mapped to CFIR constructs, Proctor’s implementation outcomes, barriers, facilitators, and reported outcomes.
3.4.4 End-of-life and palliative care.
Seventeen studies examined end-of-life (EOL) and palliative care interventions for refugee and displaced populations, focusing on advanced illness, symptom management, and culturally appropriate spiritual support [60,61,64,87–100].
Intervention characteristics most frequently included home-based palliative care, dignity-preserving approaches, integration of cultural and religious rituals, and cross-cultural provider training [88,95,98]. Some studies reported models linking palliative care with primary health or HIV services, which broadened access [60,87,100]. Flexible outreach and mobile teams were also described as enhancing feasibility for mobile or marginalized populations [99].
Outer Setting determinants reported as barriers included the absence of palliative care in humanitarian policy, shortages of essential medicines (particularly opioids), and legal or regulatory exclusions limiting refugee access [91,93,97]. Camp resource scarcity, unstable housing, and systemic inequities were also identified as obstacles to continuity of care [91,99]. Inner Setting constraints included limited provider preparedness, inadequate awareness of palliative approaches, and fragmented coordination between humanitarian and health actors [89,90]. Where specialist palliative units, NGO–health system partnerships, or multidisciplinary outreach teams were present, adoption and integration were stronger [61,87,90].
Characteristics of individuals influenced delivery and engagement. Provider-level skills in communication and cultural awareness were reported as shaping quality of care. Refugee patients and families frequently relied on religious rituals, faith-based coping, and cultural understandings of dignity in illness and death [88,98]. Process strategies emphasized family involvement in care planning, engagement of faith and community leaders, inclusive spatial design, and cross-sector coordination [87,89,98].
Across Proctor’s outcomes, interventions were reported as acceptable and appropriate when incorporating cultural and religious practices, family structures, and inclusive rituals [87,88]. Feasibility was reported as higher in integrated primary–palliative care models, community-based services, and flexible outreach [87,99]. Adoption was supported through NGO partnerships, community leadership, and faith-based mediation [89,98]. Fidelity was strongest when dignity-care protocols and family-inclusive planning were consistently applied. Penetration and sustainability were limited overall, though studies noted improvements when services were integrated into host-country primary care systems and supported with policy or dedicated resources [60,87].
Reported barriers included language and communication gaps, stigma, cultural misunderstandings, mistrust of formal services, shortages of trained providers, restricted opioid access, policy exclusions, and disruptions associated with displacement and legal precarity [91,93,95,97,99]. Reported facilitators included family engagement, safe and inclusive clinical environments, interpreter and mediator provision, involvement of religious leaders, and NGO–health system collaboration [87,89,98]. Reported outcomes included reductions in symptom distress and unnecessary hospitalizations [60,64,93]. Patient- and family-level outcomes included preservation of dignity, improved trust in providers, strengthened caregiver–staff relationships, and reduced emotional distress [88,93,98]. Both pediatric and adult studies reported that culturally respectful, community-integrated approaches were associated with improved comfort and increased utilization of palliative services [61,95] (Table 6).
Table 6: Summary of qualitative evidence on end-of-life and palliative care interventions for refugee populations mapped to CFIR constructs, Proctor’s implementation outcomes, barriers, facilitators, and reported outcomes.
3.5 Integrated CFIR–proctor synthesis of refugee health interventions
This review undertook an integrated analysis of implementation determinants, outcomes, barriers, and facilitators across the four domains of refugee health interventions. Across domains, cultural adaptation, participatory design, and intervention flexibility were consistently reported as central features shaping acceptability, appropriateness, and fidelity. For instance, stigma-sensitive and community-anchored approaches were described in mental health interventions [52,66,67], rights-based and intersectional strategies in disability inclusion [56,73,74], peer-led and co-designed delivery in women’s health [54,82,83], and dignity-preserving integration into primary health systems in palliative care [60,87,88].
When mapped to Proctor’s outcomes, findings followed a common gradient across the literature. Acceptability, appropriateness, and feasibility were the most frequently documented and were typically achieved in the early phases of implementation. By contrast, adoption, fidelity, penetration, and sustainability were reported less often and were more closely associated with interventions that demonstrated stronger systemic integration. For example, disability-inclusive education programs maintained adoption when linked to school readiness and teacher training [63], while palliative care interventions demonstrated continuity when embedded within host-country primary care structures [60, 87].
Barriers cutting across all domains were predominantly structural. Policy exclusions, regulatory gaps, stigma, discrimination, and resource scarcity including shortages of essential medicines, assistive devices, and trained personnel were widely reported as limiting penetration and scale [57,62,91,97]. These systemic constraints were compounded by logistical challenges such as unstable housing, transport difficulties, and digital divides, all of which undermined continuity and equity in service delivery [55,58,73].
Alongside these constraints, studies identified a range of facilitators that supported implementation. Participatory design processes, community and peer engagement, interpreter and cultural mediation services, cross-sector partnerships, and organizational readiness were frequently described as enabling mechanisms across domains [67,70,77,98]. Where these facilitators were present, interventions achieved stronger contextual fit and greater engagement.
The outcomes reported across domains reflected these patterns of barriers and facilitators. Documented results included improved service uptake in maternal health and preventive screening [82,84]; reductions in psychological distress, stigma, and trauma symptoms in mental health interventions [66,68]; enhanced social participation and empowerment for persons with disabilities [63,72]; and strengthened dignity, trust, and continuity of care in end-of-life and palliative interventions [88,95] (Table 7).
Table 7: Cross-Domain Determinants, Outcomes, Barriers, and Facilitators for Refugee Health Interventions.
3.6 Comparative Findings by Income Setting
Of the 49 included studies, 32 were conducted primarily in high-income countries (HICs), 15 in low- and middle-income countries (LMICs), and 2 in multi-country or cross-regional settings. Mental health and disability inclusion studies were more frequently located in HIC resettlement contexts, while end-of-life and palliative care studies were more commonly situated in LMIC humanitarian settings. Women’s health studies were distributed across both income settings, though numerically fewer than studies in other domains.
Across domains, studies conducted in HICs predominantly described interventions delivered through formal health systems, including structured clinical services, interpreter-supported programs, and institutionally based models of care. Studies conducted in LMICs more often reported community-based, NGO-supported, and informal service models delivered in resource-constrained environments. A domain-specific summary of these observed differences is presented in Table 8.
Table 8: Evidence patterns and assets by income setting across four domains (n = 49).
4. Discussion
This review provides a cross-domain synthesis of refugee health interventions spanning mental health, disability inclusion, women’s health, and end-of-life/palliative care. Across these domains, three implementation outcomes acceptability, appropriateness, and feasibility were most consistently achieved, while adoption, fidelity, and sustainability were observed primarily in interventions that progressed beyond pilot stages. Shared determinants of success included cultural adaptation, community engagement, participatory design, and provider cultural competence, all of which were strongly associated with higher uptake and trust. Conversely, policy gaps, stigma, discrimination, service fragmentation, and resource scarcity emerged as recurrent barriers limiting penetration and sustainability. The synthesis also identified innovative facilitators such as faith-integrated mental health models, inclusive prevention strategies, peer-led women’s health education, and family-centred palliative care, which contributed to measurable improvements in help-seeking, maternal health access, disability inclusion, and dignified end-of-life experiences. By systematically mapping determinants to implementation outcomes through a CFIR–Proctor hybrid framework, this review moves beyond domain-specific analyses to highlight transferable strategies that can inform refugee health policy and practice globally.
Findings reaffirm well-documented barriers to refugee mental health service utilization, most notably language limitations, stigma, bureaucratic hurdles, and digital access constraints, which have been consistently reported across systematic reviews [23,30,101–103]. While previous reviews have emphasized the importance of culturally sensitive care and provider training [30,101,102], few examined the operational impact of faith-based or digital modalities. The present analysis advances the literature by demonstrating how culturally congruent psychosocial models and stigma-aware digital tools can improve engagement and acceptability, linking these directly to reported reductions in depression, anxiety, and post-traumatic stress disorder [104,105].
Disability inclusion remains comparatively underrepresented in refugee health research. This review makes a novel contribution by identifying inclusive prevention models, culturally adapted developmental screening, and intersectional gender–disability programming as effective strategies. Earlier reviews have noted fragmented services and entrenched stigma as persistent barriers; however, the present synthesis identifies tangible facilitators such as advocacy-led program design, peer support networks, and teacher training. Outcomes including early identification of developmental needs and improved caregiver coping capacities provide an additional dimension of evidence seldom reported previously [106–108]. Consistent with Rfat et al. (2022), findings highlight the influence of systemic discrimination, legal restrictions, and resource scarcity in limiting access to inclusive healthcare, education, and social participation [106]. The review also aligns with calls from Njelesani et al. (2022) and Malloy et al. (2023) for participatory, accessible research design that directly involves persons with disabilities and centres their lived experiences [107,109].
In women’s health, this review confirms established evidence of refugee women’s heightened vulnerability to adverse perinatal outcomes, and mental health challenges [110], as well as the importance of social support, health literacy, and culturally responsive care [111]. While prior reviews have specifically called for improved communication and navigation [112], the present findings identify operational models including peer-led health education, participatory co-leadership, female provider engagement, and multi-sectoral service integration that were associated with improved screening uptake, interpersonal trust, and maternal mental health outcomes.
Evidence on end-of-life and palliative care for refugees remains limited, with most earlier reviews emphasizing unmet needs for culturally sensitive, family-oriented approaches but offering few empirical evaluations [113,114]. This review addresses that gap by presenting findings on family-centred palliative models, dignity-preserving care, and the integration of primary and palliative services. Whereas earlier literature highlighted the absence of structured frameworks and the challenges of delivering care in resource-constrained or unstable settings [113,115], this synthesis documents operational strategies such as outreach and mobile service models that extended access to marginalized populations. Reported outcomes included reduced symptom distress, improved dignity, and strengthened patient–provider trust, providing empirical evidence of effectiveness. These results are consistent with global calls for integrating palliative care into primary health systems, including WHO guidance on essential palliative services in humanitarian crises [116]. At the same time, most interventions remain pilot-level, lack long-term sustainability evidence, and are rarely scaled within national health strategies.
The comparative findings by income setting underscore a well-established principle in global health implementation: the effectiveness of refugee health interventions is shaped primarily by the structural and service environments in which they are delivered. Evidence from high-income countries reflects greater reliance on formal health-system assets, including specialist services, interpreter-supported care, and structured clinical pathways features that have been shown to facilitate coordination, continuity, and quality of care for refugee populations [117,118]. In contrast, studies from low- and middle-income and humanitarian settings more often described interventions implemented through community networks, non-governmental organizations, and informal support platforms operating in resource-constrained contexts, a pattern consistently documented in humanitarian mental health and psychosocial support literature [119,120]. These differences align with broader implementation science evidence demonstrating that complex health interventions achieve greater feasibility and impact when they are adapted to local system capacities and social realities rather than transferred without contextual modification [121,122]. Across domains, the present review found that cultural adaptation, participatory design, and contextual flexibility were central to acceptability and feasibility an observation consistent with extensive evidence on culturally responsive care for migrant and refugee populations [123,124]. Global policy guidance further emphasizes that community engagement and locally grounded service models are essential components of effective refugee and migrant health programming [125,126]. The predominance of studies from high-income settings nevertheless highlights a persistent imbalance in the evidence base and reinforces longstanding calls for greater investment in implementation research within low-resource and displacement-affected contexts [51]. Together, these findings point to the need for implementation strategies that prioritize contextual fit and equity, and for a rebalancing of the research agenda to better reflect the realities of the settings in which most displaced populations reside.
Taken together, the cross-domain synthesis reveals shared barriers including policy gaps, stigma, and resource scarcity and common facilitators such as cultural adaptation, community engagement, and participatory design, in line with the broader literature [23,101,103,110,111]. The unique contribution of this review lies in systematically mapping these determinants to specific implementation outcomes (acceptability, feasibility, sustainability) and demonstrating that community-driven, context-specific approaches are consistently associated with higher impact. This integrative perspective contrasts with the compartmentalized treatment of refugee health domains in prior reviews, offering a more coherent understanding of transferable strategies for donors, policymakers, and practitioners.
Methodologically, the review aligns with established scoping review frameworks (Arksey and O’Malley; Levac et al.; PRISMA-ScR), ensuring transparency, replicability, and comprehensive coverage [23,127,128]. Core processes included multi-database systematic searches, explicit eligibility criteria, and dual independent screening and data extraction [23,29,129]. While quality appraisal is not typically required in scoping reviews, the use of the CASP Qualitative Checklist enhanced interpretive validity without influencing inclusion [30]. The review also extends methodological standards by mapping findings to the CFIR framework and Proctor’s taxonomy of implementation outcomes, enabling nuanced cross-domain analysis and enhancing transferability an aspect often missing from earlier reviews [23,127,128]. The systematic integration of participatory and community-based approaches in both analysis and interpretation further distinguishes this review as methodologically robust and innovative [128].
In general, the synthesis demonstrates that community-driven, culturally adapted, and participatory models were consistently associated with higher uptake and sustainability than fragmented or top-down approaches. Shared facilitators including cultural competence, trust-based delivery, and community engagement supported implementation across all domains, while policy gaps, stigma, and resource scarcity remained persistent barriers. By aligning with global priorities articulated in the Sustainable developmental goals and WHO’s Global Action Plan for Refugee and Migrant Health, this review provides an evidence base for the design of interventions that are both locally responsive and globally transferable.
Strengths and limitations
This review’s main strength lies in its methodological rigor and breadth. Guided by established scoping review frameworks, it used systematic multi-database searches, explicit eligibility criteria, and dual independent screening to ensure transparency and replicability. Mapping findings to CFIR and Proctor’s implementation outcomes enabled a structured cross-domain synthesis, while the inclusion of participatory and community-focused perspectives enhanced contextual relevance.
Several limitations should be acknowledged. Restricting inclusion to English-language, peer-reviewed qualitative studies may have excluded relevant non-English and grey literature, particularly from humanitarian settings. Geographic and income-level representation was uneven, with a predominance of studies from high-income resettlement contexts and comparatively limited evidence from low- and middle-income countries where most displaced populations reside. This imbalance may have led to greater documentation of formal health-system–based models and underrepresentation of community-driven approaches common in resource-constrained settings. In addition, as a scoping review, the study was not designed to assess effectiveness or establish causal relationships. Finally, findings reflect the literature available up to 2025 and may require updating as contexts and interventions evolve.
These limitations temper generalizability but do not diminish the review’s contribution in synthesizing qualitative evidence across four key domains and in identifying critical gaps and priorities for future refugee health research.
Recommendations
Based on the mapped evidence, several recommendations can be drawn to guide future policy, practice, and research on refugee health interventions.
For policymakers, the evidence highlights the importance of integrating culturally congruent and community-driven elements into refugee health strategies. Key considerations include embedding participatory design, accommodating faith and cultural practices, and ensuring family engagement, all supported by mechanisms for cross-sector coordination and sustained financing.
For health systems and practitioners, findings underscore the need to embed culturally competent, trauma-informed, and context-specific approaches into service delivery. These efforts should be reinforced by targeted workforce training and strong partnerships with refugee communities to ensure trust, accessibility, and continuity of care. For humanitarian actors and NGOs, greater alignment with national and local health systems is critical. Priority should be given to mobile and outreach-based models of service delivery to extend coverage to underserved and mobile refugee populations who are often excluded from formal systems of care.
For researchers, there remains a need to address underexplored domains such as disability inclusion and palliative care. Future studies should expand the evidence base through participatory methodologies and mixed-methods designs, with particular attention to underrepresented geographic contexts where the majority of refugees reside.
Conclusion
This scoping review synthesizes qualitative evidence on refugee health interventions across four priority domains mental health, disability inclusion, women’s health, and end-of-life care capturing both cross-cutting and domain-specific barriers, facilitators, and outcomes. By applying CFIR and Proctor’s frameworks, the review extends beyond descriptive mapping to identify implementation patterns that inform context-sensitive, culturally grounded, and system-integrated approaches. Although causal inferences cannot be established, the synthesis provides a robust foundation for policy development, program design, and future research. Across domains, the findings consistently emphasize the importance of community engagement, cultural adaptation, and cross-sector collaboration in improving the accessibility, quality, and sustainability of health services for displaced populations.
Supporting information
S1 TableSearch terms by database used in the scoping review.(DOCX)
S2 TableData extraction format for included studies.(DOCX)
S3 TableCharacteristics and evidence synthesis of included studies across four domains.(DOCX)
S4 TableCritical appraisal of included qualitative studies using the CASP checklist.(DOCX)
S1 ChecklistPRISMA Checklist.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abubakar I, Devakumar D, Madise N, Sammonds P, Groce N, Zimmerman C, et al. UCL-Lancet Commission on Migration and Health. Lancet. 2016;388(10050):1141–2. doi: 10.1016/S 0140-6736(16)31581-1 27650082 · doi ↗ · pubmed ↗
- 2Hargreaves S, Rustage K, Nellums LB, Mc Alpine A, Pocock N, Devakumar D, et al. Occupational health outcomes among international migrant workers: a systematic review and meta-analysis. Lancet Glob Health. 2019;7(7):e 872–82. doi: 10.1016/S 2214-109X(19)30204-9 31122905 PMC 6565984 · doi ↗ · pubmed ↗
- 3Lindert J, Carta MG, Schäfer I, Mollica RF. Refugees mental health-A public mental health challenge. Eur J Public Health. 2016;26(3):374–5. doi: 10.1093/eurpub/ckw 010 27053728 · doi ↗ · pubmed ↗
- 4Uphoff E, Robertson L, Cabieses B, Villalón FJ, Purgato M, Churchill R, et al. An overview of systematic reviews on mental health promotion, prevention, and treatment of common mental disorders for refugees, asylum seekers, and internally displaced persons. Cochrane Database Syst Rev. 2020;9(9):CD 013458. doi: 10.1002/14651858.CD 013458.pub 2 32885850 PMC 8572368 · doi ↗ · pubmed ↗
- 5Grasser LR. Addressing mental health concerns in refugees and displaced populations: is enough being done?. Risk Management and Healthcare Policy. 2022;:909–22.35573980 10.2147/RMHP.S 270233 PMC 9094640 · doi ↗ · pubmed ↗
- 6Asif Z, Kienzler H. Structural barriers to refugee, asylum seeker and undocumented migrant healthcare access. Perceptions of Doctors of the World caseworkers in the UK. SSM - Mental Health. 2022;2:100088. doi: 10.1016/j.ssmmh.2022.100088 · doi ↗
- 7Cantor D, Swartz J, Roberts B, Abbara A, Ager A, Bhutta ZA, et al. Understanding the health needs of internally displaced persons: A scoping review. J Migr Health. 2021;4:100071. doi: 10.1016/j.jmh.2021.100071 34820657 PMC 8600058 · doi ↗ · pubmed ↗
- 8Ní Ghráinne B. Internally Displaced Persons and Exclusion Clauses. International Journal of Refugee Law. 2025;37(2):219–34. doi: 10.1093/ijrl/eeaf 016 · doi ↗