Biomechanical and physiological effects of a passive upper-body exoskeleton during stair ascent and descent
Gabriela Garcia, Milena Espoz, Camilo Albuja, Rafaella Yañez, Paul G. Arauz, Bernard J. Martin

TL;DR
This study examines how a passive upper-body exoskeleton affects physical strain and comfort during stair climbing and descending with a load.
Contribution
The study provides empirical evidence of a passive exoskeleton's biomechanical and physiological effects during stair negotiation with a load.
Findings
The exoskeleton reduced heart rate and muscle activity in the biceps brachii and erector spinae during stair ascent and descent.
Participants reported lower perceived discomfort when using the exoskeleton, especially males.
The exoskeleton caused reduced joint range of motion in males but increased range of motion in some lower-body joints for females.
Abstract
The market has seen the emergence of various passive exoskeletons designed to assist with carrying tasks; however, evidence of their effects during stair negotiation remains limited. In this study fifteen female and fifteen male participants carried a 12-kg load with and without an upper-body passive exoskeleton (CarrySuitⓇ) while ascending and descending stairs. The impact of the CarrySuitⓇ was evaluated through measurements of heart rate, muscle activity, and joint range of motion during both stair ascent and descent. The results indicated that heart rate and muscle activity in the biceps brachii and erector spinae were reduced during both ascent and descent when wearing the exoskeleton, except in females during descent, where muscle activity remained comparable between conditions. An increase in upper-leg muscle activity was observed only in males during ascent, while lower-leg…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
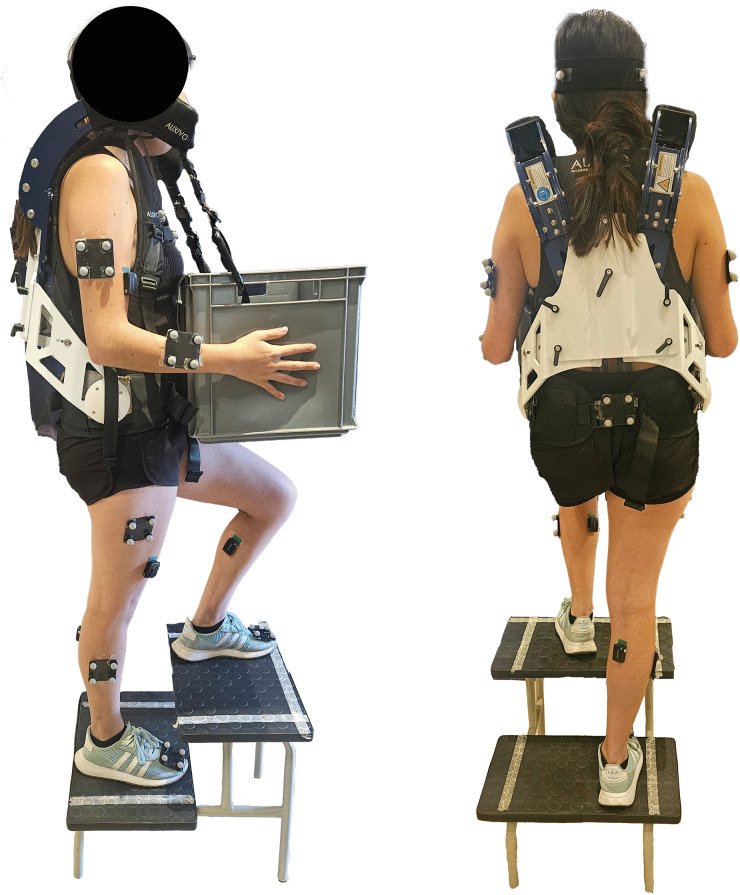 Fig 1
Fig 1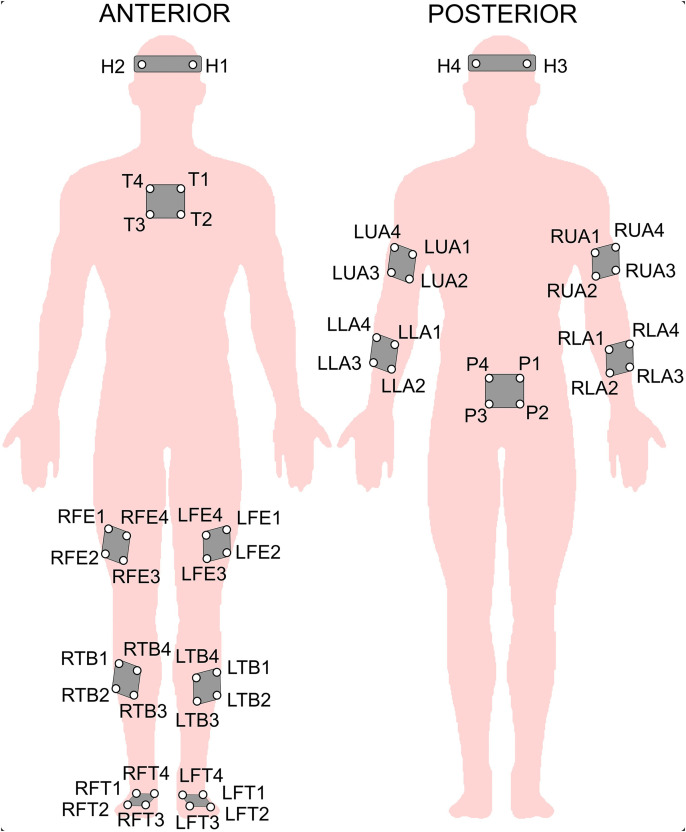 Fig 2
Fig 2- —http://dx.doi.org/10.13039/501100010654Universidad San Francisco de Quito
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProsthetics and Rehabilitation Robotics · Stroke Rehabilitation and Recovery · Balance, Gait, and Falls Prevention
Introduction
Manual material handling remains a core component of many industrial and labor-intensive sectors, despite growing trends in automation and mechanization. International reports indicate that over 30% of workers regularly carry and transport heavy loads as part of their daily tasks [1]. These physically demanding activities are closely associated with the development of musculoskeletal disorders (MSDs), particularly in the lower back, lower extremities, and upper limbs [2–5]. Work-related MSDs are among the leading causes of occupational disability, negatively impacting productivity, worker well-being, and overall economic outcomes [6–8].
Efforts to mitigate physical workload in occupational environments have led to the exploration of various ergonomic strategies. However, traditional solutions such as automation, material handling equipment, or workspace redesign are not always feasible, especially in complex or constrained environments such as stairwells, multi-story buildings, construction sites, and uneven outdoor terrain. In such settings, wearable assistive technologies, including exoskeletons, have gained attention as practical tools for alleviating physical strain and reducing the risk of injury. Passive exoskeletons, in particular, offer a promising balance of structural support and affordability by using energy-storing components or frame-based load distribution systems rather than powered actuators [9].
Although passive exoskeletons have been extensively studied for static tasks, overhead work, and lifting [10,11], only a limited number are specifically designed to support dynamic load carriage, and even fewer have been evaluated in conditions involving stair negotiation [12–14]. One such device is the CarrySuit^Ⓡ^, a commercially available passive upper-body exoskeleton designed by Auxivo AG (Schwerzenbach, Switzerland). The device redistributes load across the torso and hips, reducing strain during manual carrying tasks. Previous studies have demonstrated positive effects of the CarrySuit^Ⓡ^ during level and inclined walking, including reductions in muscle activation and heart rate [12–15]. However, its performance during stair ascent and descent remains largely unexamined.
Stair negotiation poses unique biomechanical and physiological challenges, making it a critical yet underexplored context for exoskeleton evaluation. Stair ascent and descent require substantial joint mobility, dynamic balance, and neuromuscular coordination [16,17]. When combined with the task of carrying a heavy load, these demands are significantly heightened. Unlike level or inclined walking, stair negotiation introduces alternating concentric and eccentric loading patterns in the lower limbs and alters movement strategies. Inefficient or asymmetrical load distribution in this context may result in compensatory motions and increased joint loading, potentially elevating injury risk [18,19]. Given these concerns, understanding how exoskeletons like the CarrySuit^Ⓡ^ influence movement quality, physiological strain, and symmetry during stair-based tasks is essential. Furthermore, sex-based differences in biomechanical responses and user perceptions have been documented in previous exoskeleton studies [13,14,20], underscoring the need for inclusive evaluations.
Accordingly, this study aimed to investigate the physiological and biomechanical effects of using the CarrySuit^Ⓡ^ during stair ascent and descent while carrying a 12 kg load, a condition that remains untested despite the exoskeletons’ growing adoption. This work addresses a critical gap in the literature: although the CarrySuit^Ⓡ^ has shown benefits on level and inclined surfaces, its impact on stair negotiation, a biomechanically demanding and common workplace scenario, has not been evaluated. To this end, we assessed muscle activity, sagittal plane joint kinematics, heart rate, and perceived discomfort to determine how the exoskeleton influences physical effort, movement control, and user experience during stair-based carrying. Specifically, the following research questions were addressed:
Does carrying 12 kg with the CarrySuit^Ⓡ^ on stairs influence heart rate, discomfort, and muscle activity (erector spinae, vastus lateralis, gastrocnemius medialis, and biceps brachii) compared to performing the same task without the exoskeleton in both males and females?Does wearing the CarrySuit^Ⓡ^ alter sagittal plane joint kinematics during stair ascent and descent relative to the no-exoskeleton condition in both sexes?Are side-based asymmetries in joint angles or muscle activity affected by exoskeleton use?
By answering these questions, the present study contributes much-needed evidence on the applicability of passive upper-body exoskeletons in complex, vertical movement tasks, offering critical insights for their ergonomic implementation in occupational settings where mechanical aids are impractical.
Methods
Participants
The study involved thirty adults, equally divided between men and women, all of whom had no prior experience with exoskeletons. Participants were recruited via internal university announcements and social media platforms. Participants volunteered and underwent a brief screening oral questionnaire administered by the research team to confirm the absence of MSDs, physical or neurological conditions, or pregnancy that might affect their ability to carry a 12 kg load or wear the exoskeleton. The average demographic data were a weight of 66.70 ± 7.28 kg, height of 176.20 ± 6.99 cm, and age of 21.33 ± 1.36 years for males, and a weight of 59.56 ± 8.39 kg, height of 160.80 ± 4.17 cm, and age of 21.47 ± 1.25 years for females. All participants were right-handed. The tested sample size provided an achieved statistical power of 91%, based on a partial eta-squared (ηp2) effect size of 0.1, and an alpha level of 0.05 (calculated using G*Power 3.1.9.7).
The study was approved by the Ethics Committee of the Universidad San Francisco de Quito (#2021-145M) and adhered to the principles outlined in the Declaration of Helsinki. All participants provided written informed consent before the experimental sessions. Participants were recruited from August 15, 2022 until December 31, 2022. This study is part of a larger investigation [15] in which participants also tested the exoskeleton during inclined treadmill walking.
CarrySuitⓇ exoskeleton
The carrying task was assessed both with and without the passive upper-body exoskeleton, the Auxivo CarrySuit^Ⓡ^ (v1.0, Schwerzenbach, Switzerland, 2021). The CarrySuit^Ⓡ^ is designed to reduce strain on the upper extremities and back during heavy manual material handling, as reported by Auxivo. Weighing 5.6 kg, the exoskeleton supports an external load of up to 50 kg. Its design resembles a backpack, featuring textile straps and cushioned contact points that connect to the hips, chest, and shoulders. The exoskeleton includes a rigid, yet adjustable, framework that extends from the hips to the shoulders, accommodating a range of anthropometric dimensions. Proper fit was ensured by adjusting the straps and aligning the frame to each participant’s torso and hip measurements, as recommended by the manufacturer. Fit was confirmed both visually and through participant feedback prior to beginning trials. External objects were secured to the front frame using straps with carabiners (see Fig 1). The load was primarily transferred through the hips and shoulders, and, since the system lacks active energy storage mechanisms such as springs, it primarily provides support during static carrying rather than during lifting or lowering actions.
Participant wearing the CarrySuitⓇ exoskeleton (EXO condition) while ascending stairs while carrying a 12 kg load.
Measures and instrumentation
Electromyography (EMG).
Surface bipolar Trigno EMG sensors (Delsys Inc., Boston, MA), with a sampling frequency of 1926Hz, were placed bilaterally on the biceps brachii along the line connecting the medial acromion to the cubital fossa at one-third of the distance from the cubital fossa [21]. Avanti EMG Sensors (Delsys Inc., Boston, MA), a newer model with a sampling frequency of 2148 Hz, were used for all other muscles tested. Sensors for the vastus lateralis were positioned at two-thirds of the distance along the line extending from the anterior superior iliac spine to the lateral aspect of the patella [21]. Sensors for the medial gastrocnemius were placed at the most prominent portion of the muscle belly [21]. For the erector spinae, sensors were positioned at the L3 height, approximately 3 cm to the left and right of the spine [22]. To ensure optimal contact, the skin was prepared by shaving, cleaning with alcohol, and lightly abrading with gel (Skin Prep Gel, Nuprep®, Aurora, USA).
Data processing was performed in MATLAB (MathWorks, Inc., Natick, USA), including detrending, filtering with a 4th-order Butterworth bandpass filter (30–300 Hz), and Fast Fourier Transform for visual inspection of the power spectra to ensure the absence of noise. Root mean square (RMS) values were calculated using a 250 ms moving window with 50% overlap and normalized to the average of the peak EMG values obtained from three submaximal voluntary contractions per muscle. These peak values were obtained during isometric exercises described in the procedure section [23]. The RMS normalization was then applied to the EMG signals recorded during the experimental stair trials. The primary outcome variables were the mean and peak normalized EMG amplitudes (% RMS values) for each muscle. The mean normalized EMG amplitude reflects the average level of muscle activation throughout the task [24], whereas the peak normalized EMG amplitude, defined as the 90th percentile of the normalized values, represents the highest consistently sustained muscle activity during the task [25].
Kinematics.
A 10-camera motion capture system (Vicon MX, Oxford, UK) recorded whole-body kinematics at a sampling frequency of 100 Hz. Groups of four 10 mm reflective spherical markers, as well as individual markers, were placed on anatomical landmarks including the head, thorax, pelvis, humerus, radius, femur, tibia, and foot (as depicted in Fig 2) to define their local coordinate systems. Following the methodology of previous studies [14,26,27], a biomechanical model including 52 markers was employed to obtain comprehensive whole-body kinematic data. 3D joint angles were calculated for the head-trunk, pelvis-trunk, shoulder (humerus-thorax), elbow (humerus-radius), hip (pelvis-femur), knee (femur-tibia), and ankle (foot-tibia) relative to a neutral standing posture used as the zero reference. The Cardan angle sequence [28] was used to determine sagittal plane angles.
Reflective marker placement for 3D motion capture.Abbreviations: L = Left, R = Right; FE = femur, TB = tibia, FT = foot, LA = lower arm, UA = upper arm, H = head, T = thorax, P = pelvis.
Data were exported and processed in MATLAB by a custom program. Angular data were segmented into individual strides, and a time-normalized waveform (0–100%) of the typical stair gait cycle was created using 1% sample steps [26,27,29]. Normalized strides for the leading leg were defined as beginning with the pull-up of the leading leg and heel contact on the first stair, followed by weight acceptance, push-off, pull-up of the stance leg, forward movement to the second stair, foot clearance, and ending with the placement of the leading leg on the second step (S1 Fig). Three cycles were averaged for each leading side, and the range of motion (ROM) was calculated for each joint angle.
Heart rate.
Heart rate, measured in beats per minute (bpm), was assessed before and during the carrying task using a chest belt heart rate monitor (Polar H10, Polar, Finland) with a 1000 Hz sampling frequency. At the start of each experimental session, participants rested in an armchair for 5 minutes, and their resting heart rate was recorded, noting the lowest value observed. Heart rate was also continuously monitored throughout the carrying task, and the average heart rate for all stair trials was calculated.
Subjective evaluation of discomfort and fatigue.
To assess participants’ subjective experiences, a two-part questionnaire was administered both before and after each carrying task. The first section focused on discomfort perception and was adapted from the Nordic Musculoskeletal Questionnaire [30], as in previous studies [31–33]. Participants were presented with a human body diagram featuring horizontal visual analogue scales (VAS) for the neck, shoulders, arms, hands/wrists, back, upper legs/hips, knees, lower legs, ankles, and feet. The 10 cm VASs were anchored with “no discomfort” on the far left (0 mm) and “extreme discomfort” on the far right (10 cm). Participants marked the scale to indicate their perceived level of discomfort, and the results were recorded in centimeters. A similar VAS was included to assess overall fatigue. The second section of the questionnaire explored the perceived usability and acceptability of the exoskeleton. It included four questions prompting participants to rate: (1) how easy was the task to perform while wearing the exoskeleton, (2) how comfortable the task felt, (3) whether they preferred performing the task with or without the exoskeleton, and (4) whether they would recommend the exoskeleton for similar carrying tasks.
Procedure
Upon arrival of the participant at the laboratory, a demonstration of the exoskeleton was given after a brief introduction. Written informed consent was obtained, and demographic data including age, sex, and handedness were collected, while stature and body mass were measured using a weight scale and a stadiometer, respectively. A 5-minutes rest was then provided while the resting heart rate was measured. Afterward, EMG electrodes were placed on the selected muscles, and participants performed three repetitions of 10-second isometric submaximal voluntary contractions for each muscle, with 1-minute rest periods in between.
For the biceps brachii, elbow flexion exercises in the vertical plane were performed with a 7.5 kg kettlebell [34]. For the gastrocnemius medialis, calf raises were performed in the upright standing posture while holding a 7.5 kg kettlebell [35]. For the vastus lateralis, knee extensions and leg raises with 2.5 kg ankle weight [36] were performed in a sitting posture. For the erector spinae, the Biering-Sorensen maneuver, extension of the trunk against a 5 kg resistance was performed with the whole body in a horizontal position [37]. These exercises are commonly used to obtain reference contractions for expressing muscle activity as a percentage of submaximal effort.
After the placement of reflective markers, participants first completed a 1-minute walk to warm up and become familiar with the exoskeleton. This was followed by 1-minute inclined treadmill walking trial under two conditions, with and without the exoskeleton, while carrying a 12 kg box, as part of the prior experiment reported elsewhere [15]. This sequence was chosen to provide progressive full-body familiarization with the device under dynamic but controlled conditions, allowing participants to acclimate to the exoskeleton’s support and movement constraints before performing the more demanding stair negotiation task. Afterward, a 30-minute rest period was provided. During this time, participants were seated and monitored to ensure full recovery between tasks, and rest durations were strictly timed using a stopwatch. Following the rest, participants performed a 1-minute stair ascent and descent trial to rewarm and complete initial subjective evaluations of discomfort and fatigue. These pre-task ratings were used to confirm that any subsequent discomfort reflected the experimental condition and not residual effects from previous tasks. Subsequently, the stair-carrying task with a 12 kg box was completed under two randomized conditions (with and without the exoskeleton). Randomization was performed using a simple random number generator to determine the order of conditions for each participant. The carrying task consisted of a total of six stair ascent and descent trials for each condition. One leg was randomly assigned as the lead for the first three trials (both ascent and descent), and the opposite leg was used as the lead for the remaining three trials. Stair ascent and descent were performed at a self-selected but consistent pace across conditions. Participants were instructed to maintain a natural rhythm and avoid sudden or exaggerated steps. Throughout the stair task, heart rate was monitored continuously, and kinematic and EMG data were recorded for each trial and were averaged for each condition and leading side. For symmetry comparisons, only the gait cycle data from the leading sides were analyzed.
Subjective evaluations of discomfort and fatigue were evaluated immediately after completion of each carrying condition (with and without the exoskeleton). The conditions were separated by a 10-minute rest period. After each rest, a control evaluation of discomfort and fatigue was conducted to ensure that discomfort levels had returned to baseline, confirming that subsequent ratings reflected the experimental condition rather than residual fatigue. Finally, the user satisfaction questionnaire was completed after all experimental trials. Participants were not informed of the specific study hypotheses prior to data collection to minimize potential bias in subjective responses.
Data analysis
Statistical analyses were performed using SAS Studio (SAS Institute Inc.) with a significance level set at α = .05. Mixed models with a variance-components covariance structure and residual maximum likelihood estimation were used (via the PROC MIXED procedure in SAS) to evaluate the outcome variables: mean and peak muscular activity, heart rate, and ROM joint angles in the sagittal plane; all data fulfilled the normality tests. For muscular activity and ROM outcome variables, participants were treated as random effects, condition (with [EXO] or without [NOEXO] the exoskeleton), and side (left or right) were treated as fixed effects. For heart rate and discomfort, the statistical model included only condition as a fixed factor. Separate models were run for male and female participants to account for anatomical and biomechanical differences known to affect musculoskeletal responses, postural strategies, and exoskeleton fit and interaction. All models were run by sex. Post-hoc analyses were conducted using least square means, and p-values were adjusted using the Tukey-Kramer method. The effect size, expressed as ηp², was calculated using the Tippey & Longnecker approach for mixed models in SAS Studio [38]. Cohen’s thresholds, which categorize effect sizes as small (ηp² = .01), medium (ηp² = .06), and large (ηp² = .14), were applied to interpret the ηp² values [39]. Descriptive results are reported as the mean with standard error. As the discomfort ratings violated the assumption of normality, a nonparametric Friedman two-way analysis of variance by ranks was conducted to assess differences across conditions.
Results
Muscle activity
Descriptive statistics (means and standard errors) and mixed-model fixed effects results for bilateral mean and peak muscle activation during stair descent while carrying a 12 kg box, with and without the exoskeleton, are presented in Table 1 for both male and female participants.
Table 1: Descriptive statistics (mean and standard error) and fixed effects analysis results for bilateral mean and peak muscle activation (% normalized RMS EMG amplitude) in male and female participants during stair descent while carrying a 12 kg box, performed with (EXO) and without (NOEXO) the exoskeleton.
In females, a significant condition-by-side interaction was found only for the peak activity of the gastrocnemius medialis, with a small to medium effect size (Table 1). Post hoc comparisons revealed significant asymmetry in both conditions, with higher activation of the right gastrocnemius medialis compared to the left (EXO: p = .01; NOEXO: p = .02). Additionally, a main effect of condition was observed for the peak activity of the gastrocnemius medialis (medium effect size), and for the mean and peak activity of the biceps brachii (large effect sizes), with higher activation in the NOEXO condition compared to the EXO condition. A main effect of side was also detected for all muscles except the vastus lateralis, indicating a right-side dominance regardless of condition (Table 1).
In males, a significant condition-by-side interaction was found only for the peak activity of the vastus lateralis, with a small to medium effect size (Table 1). Post hoc comparisons revealed only one significant asymmetry: greater vastus lateralis peak activation in the right muscle compared to the left during the EXO condition (p = .003). Additionally, a main effect of condition was observed for the mean and peak activity of the biceps brachii, erector spinae, and gastrocnemius medialis, with higher activations in the NOEXO condition compared to the EXO condition. A main effect of side was also detected for all muscles, indicating right-side dominance regardless of condition (Table 1).
Descriptive statistics (means and standard errors) and mixed-model fixed effects results for bilateral mean and peak muscle activation during stair ascent while carrying a 12 kg box, with and without the exoskeleton, are presented in Table 2 for both male and female participants.
Table 2: Descriptive statistics (mean and standard error) and fixed effects analysis results for bilateral mean and peak muscle activation (% normalized RMS EMG amplitude) in male and female participants during stair ascent while carrying a 12 kg box, performed with (EXO) and without (NOEXO) the exoskeleton.
In females, a significant condition-by-side interaction was found for the mean activity of the erector spinae and the peak activity of the biceps brachii, both showing small effect sizes (Table 2). Post hoc comparisons revealed only one significant asymmetry: during the EXO condition, the right biceps brachii exhibited higher activation compared to the left (p = .01), while no significant asymmetry was observed for the erector spinae or in the NOEXO condition. Additionally, a main effect of condition was identified for both the mean and peak activities of the biceps brachii and erector spinae, with medium to large effect sizes, showing higher activation levels in the NOEXO condition compared to the EXO condition. A main effect of side was also detected for the biceps brachii and gastrocnemius medialis, indicating right-side dominance regardless of condition.
In males, a significant condition-by-side interaction was observed only for the mean and peak activities of the biceps brachii, with small to medium effect sizes (Table 2). However, post hoc comparisons did not reveal any significant asymmetries in these muscles. A main effect of condition was observed for the mean and peak activities of the biceps brachii and erector spinae, with higher activation in the NOEXO condition compared to the EXO condition. Additionally, a main effect of condition was found for the mean and peak activities of the vastus lateralis, showing lower activation in the NOEXO condition compared to the EXO condition. Finally, a main effect of side was detected for the mean activation of the vastus lateralis, peak activation of the erector spinae, and both mean and peak activations of the gastrocnemius medialis, all indicating right-side dominance regardless of condition.
Whole-body kinematics
Descriptive statistics (means and standard errors) and mixed-model fixed effects results for bilateral sagittal plane joint angles during stair descent while carrying a 12 kg box, with and without the exoskeleton, are presented in Table 3 for both male and female participants.
Table 3: Descriptive statistics (mean and standard error in degrees) and fixed effects analysis results for bilateral sagittal plane joint angles in male and female participants during stair descent while carrying a 12 kg box, performed with (EXO) and without (NOEXO) the exoskeleton.
In females, a significant main effect of condition, with large effect sizes, was found for the knees, hips, and neck. Specifically, the EXO condition resulted in greater ROM in the knees and hips, and reduced ROM in the neck compared to the NOEXO condition. In males, a significant main effect of condition, also with large effect sizes, was observed for the shoulders, elbows, and pelvis, with higher ROM in the NOEXO condition compared to the EXO condition. No significant main effect of side or condition-by-side interaction was detected in either males or females.
Descriptive statistics (means and standard errors) and mixed-model fixed effects results for bilateral sagittal plane joint angles during stair ascent while carrying a 12 kg box, with and without the exoskeleton, are presented in Table 4 for both male and female participants.
Table 4: Descriptive statistics (mean and standard error in degrees) and fixed effects analysis results for bilateral sagittal plane joint angles in male and female participants during stair ascent while carrying a 12 kg box, performed with (EXO) and without (NOEXO) the exoskeleton.
In females, a significant main effect of condition, with large effect sizes, was found for the ankles, hips, shoulders, and thorax. Specifically, ROM was greater in the ankles, hips, and shoulders, and reduced in the thorax in the EXO compared to the NOEXO condition. Additionally, a main effect of side was observed for the knees and hips, indicating greater ROM on the right side regardless of condition. However, no significant condition-by-side interaction was detected.
In males, a significant condition-by-side interaction, with medium effect size, was observed only for the knees. Post hoc comparisons revealed only one significant asymmetry: during the NOEXO condition, the right knee exhibited higher ROM compared to the left (p < .0001), whereas no significant asymmetry was found under the EXO condition. Additionally, a main effect of condition, with medium to large effect sizes, was observed for the ankles, knees, hips, shoulders, elbows, pelvis, and thorax. Specifically, ROM was greater in the ankles and knees, and reduced in the hips, shoulders, elbows, pelvis, and thorax in the EXO compared to the NOEXO condition. Finally, a main effect of side was observed for the knees and hips indicating greater ROM on the right side regardless of condition.
Subjective evaluation of discomfort and fatigue
Descriptive statistics (means and standard errors) and Friedman test results for discomfort and fatigue ratings following stair ascent and descent while carrying a 12 kg box, with and without the exoskeleton, are presented in Table 5 for both male and female participants.
Table 5: Descriptive statistics (mean and standard error) and Friedman test results for discomfort and fatigue ratings (0-10) in male and female participants after stair ascent and descent while carrying a 12 kg box, performed with (EXO) and without (NOEXO) the exoskeleton.
In females, discomfort in the hands/wrists and overall fatigue were significantly higher in the NOEXO condition compared to the EXO condition. In males, more differences were observed: discomfort was significantly higher without the exoskeleton in the elbows/arms, hands/wrists, lower back, knees, and ankles. However, no significant difference was found in overall fatigue between conditions.
Regarding the second section of the questionnaire, 22 out of 30 participants rated the task as easy to perform with the exoskeleton, selecting scores above 7/10. Additionally, 19 participants gave scores above 7/10 for how comfortable it is to perform the task with the exoskeleton. A total of 25 out of 30 participants indicated a preference for performing the task with the exoskeleton, and 28 out of 30 participants reported that they would recommend the exoskeleton for similar load-carrying tasks.
Heart rate
In females, statistical analysis revealed a significantly lower mean heart rate during the EXO condition (M = 96.20, SE = 3.96 bpm) compared to the NOEXO condition (M = 107.60, SE = 3.97 bpm), p = .002. Similarly, in males, a significantly lower mean heart rate was observed in the EXO condition (M = 90.71, SE = 5.15 bpm) compared to the NOEXO condition (M = 99.86, SE = 5.16 bpm), p < .0001. Resting heart rates prior to each experimental condition were not significantly different for either sex and were both significantly lower than the corresponding mean heart rates during activity (p < .0001; Females: M = 75.15, SE = 2.10 bpm; Males: M = 77.15, SE = 4.04 bpm).
Discussion
This study evaluated the effects of a passive upper-body exoskeleton (CarrySuit^Ⓡ^) on physiological, biomechanical, and perceptual outcomes during stair ascent and descent while carrying a load. Despite growing interest in passive exoskeletons for manual material handling, little is known about their impact during stair negotiation. By comparing heart rate, muscle activity, joint motion, and perceived discomfort in 30 participants carrying a 12 kg load with and without the exoskeleton, the findings demonstrate that the CarrySuit^Ⓡ^ can reduce muscular and cardiovascular strain and improve user comfort without significantly altering natural movement patterns that are critical for safe stair mobility.
Muscle activity and cardiovascular response
As expected, the most consistent finding across conditions and sexes was the reduced mean and peak activation of the biceps brachii when using the exoskeleton. This aligns with previous reports on the CarrySuit^Ⓡ^ during carrying tasks on flat surfaces [13,40], which also demonstrated an effective reduction of upper-limb muscular effort compared to carrying without the exoskeleton. Regarding the lower back, a reduced activation was evident for both sexes during stair ascent, but not in females during stair descent. This suggests that the CarrySuit^Ⓡ^’s effect on reducing lumbar load may be more consistent in males during stair negotiation. While lumbar activity remained stable in females during descent, this did not indicate added low back strain, highlighting a positive benefit of the device for load carriage during stair negotiation. These findings are consistent with earlier evaluations of the CarrySuit^Ⓡ^ on level ground (13), treadmill walking [41], and inclined surfaces (15), as well as with a study involving an active back-support exoskeleton [42].
In the upper leg, males exhibited increased vastus lateralis activation during stair ascent and a notable asymmetry during stair descent when using the exoskeleton, with approximately 20% greater activation on the right side. Given that all participants were right-handed, this asymmetry may reflect habitual limb dominance influencing stabilization strategies or movement patterns rather than random variability. These upper-leg alterations were not observed in females, suggesting potential sex-specific differences in muscle recruitment patterns or stabilization strategies when using the CarrySuit^Ⓡ^ during stair negotiation. These patterns are in line with prior research evaluating the CarrySuit^Ⓡ^ during carrying tasks on level surfaces [14,15]. In the lower leg, gastrocnemius medialis tended to be lower with the exoskeleton, particularly during stair descent, which contrast with reports of increased calf muscle demand in other back-support exoskeletons during industrial tasks [43,44]. This suggests that lower-limb muscle responses are influenced by specific design of the exoskeleton and the nature of the task. Notably, in the present study, gastrocnemius activation was asymmetric in females under both conditions, but the magnitude of asymmetry was reduced with the exoskeleton (~10%) compared to without it (~30%). Previous research has suggested that asymmetries exceeding 20% may indicate neuromuscular imbalance and could increase the risk of falling [45,46]. Therefore, the reduced asymmetry observed with the exoskeleton may reflect a more balanced muscle recruitment strategy during stair negotiation.
Finally, the reduction in muscle activity observed with the exoskeleton is supported by significantly lower heart rates in the EXO condition for both sexes, indicating reduced cardiovascular strain and overall physical effort during stair negotiation. Importantly, this reduction occurred despite the added weight of the CarrySuit^Ⓡ^, suggesting that the device’s ergonomic support more than offset its mass. These results reinforce the notion that the exoskeleton effectively reduces physiological load, even under complex, vertical movement tasks. This finding is also consistent with previous studies on carrying tasks with the CarrySuit^Ⓡ^ [13,15,41].
Kinematics
Kinematic analysis revealed condition-dependent changes in sagittal plane joint angles. Notably, the EXO condition was associated with reduced joint ROM in several upper and lower body segments, particularly in males. Since the CarrySuit^Ⓡ^ is anchored at the pelvis and secured with straps around the trunk, it may contribute to maintaining a more neutral alignment of the pelvis and trunk during movement. Similar changes in pelvic and trunk positioning have been documented in gait studies involving backpack loads [47], as well as in previous assessments of the CarrySuit^Ⓡ^ on both level and inclined surfaces [14,15], particularly among male participants.
In females, reductions in ROM were limited to the neck and thorax, while increases were observed at the knees and hips during descent, and at the ankles, hips, and shoulders during ascent. This increased ROM at the knees and hips during descent may reflect a more dynamic or deeper movement strategy, which could demand greater postural control. Such compensatory control could explain the absence of reduced erector spinae activation observed in females during this phase. For males, ROM increases were confined to the ankles and knees during stair ascent.
Prior research has shown that carrying frontal loads on stairs tends to increase hip and knee ROM and reduce ankle dorsiflexion, potentially elevating biomechanical demand and fall risk [48,49]. In this study, while the EXO condition was associated with some increases in lower-limb ROM, particularly in females, ankle mobility was preserved, and exaggerated hip and knee angles were not substantially amplified. Importantly, the exoskeleton appeared to mitigate thoracic ROM during stair ascent, which contrasts with previous findings showing increased trunk tilt during loaded versus unloaded stair climbing [18,19,48]. This suggests a possible stabilizing effect of the exoskeleton on trunk posture. Overall, these findings indicate that the CarrySuit^Ⓡ^ does not restrict essential joint mobility and may help promote more stable movement patterns during stair negotiation, particularly given that no asymmetries in joint angles were observed with the exoskeleton. Moreover, although some reductions in joint ROM were observed, all values remained within functional and normative ranges [50,51], indicating that these changes are not restrictive or detrimental to task performance.
Perceived discomfort and user feedback
Perceived discomfort and fatigue ratings further support the physiological findings. Female participants reported significantly less discomfort in the hands and wrists, along with lower overall fatigue when using the exoskeleton. Male participants experienced even broader relief, with reduced discomfort reported in multiple regions, including arms, lower back, knees, and ankles. These subjective outcomes are consistent with the observed reductions in muscle activation and with previous evaluations of the CarrySuit^Ⓡ^ [13,14,41]. This may reflect the exoskeleton’s effective redistribution of load, as contact forces are transferred to different body regions, thereby reducing localized muscular demand, such as in the biceps brachii and erector spinae. Notably, user satisfaction was high: over 80% of participants rated the device as easy and comfortable to use, and more than 90% indicated they would recommend it for similar load-carrying tasks. These findings highlight the exoskeleton’s potential for real-world acceptance and practical implementation in occupational settings.
Study limitations
This study has several limitations. First, although stair tasks are highly relevant in occupational settings, the results may not be generalizable to other vertical or uneven terrains. Second, the standardized load of 12 kg may not capture the full range of load demands encountered in real-world job scenarios. Third, while a familiarization period was provided prior to testing, potential adaptation effects may still have influenced participant performance. Fourth, the participant sample consisted primarily of relatively young individuals, which may limit the applicability of the findings to a more age-diverse workforce. Fifth, all participants were university students, and data on physical activity levels or occupational background were not collected, which may limit the generalizability of the results to more diverse working populations. Finally, long-term use effects were not assessed. Nevertheless, the observed reductions in muscle activation and cardiovascular strain strongly support the ergonomic potential of the CarrySuit^Ⓡ^’s design. Future studies should investigate the cumulative impact of exoskeleton use over extended work durations and examine performance across a wider variety of environmental and task conditions.
Conclusions
The present study evaluated the biomechanical and physiological effects of a passive upper-body exoskeleton (CarrySuit^Ⓡ^) during stair ascent and descent while carrying a 12 kg load. The findings indicate that the exoskeleton effectively reduced muscle activation in the biceps brachii and erector spinae during stair negotiation. However, this reduction in erector spinae activity was not observed in female participants during descent, although activation levels remained comparable to the condition without exoskeletal support. Lower-leg muscle activity during descent was reduced across all participants, while an increase in upper-leg muscle activation was observed exclusively in males during ascent. Side-to-side differences in lower-limb muscle activity were minimal with the exoskeleton, and no asymmetries were found in joint ROM. Reductions in joint movement amplitude were observed in several segments, particularly in males, with the most notable decreases at the shoulders, elbows, pelvis, hips, and thorax. In females, reductions were limited to the neck and thorax. In contrast, increases in ROM were noted in the ankles and knees in both sexes, and in the hips and shoulders among females. Overall, the CarrySuit^Ⓡ^ significantly reduced muscular and cardiovascular strain and improved user comfort during stair-based load carrying, although effects varied by sex and movement direction. Importantly, these benefits were achieved without compromising essential joint mobility, highlighting the exoskeleton’s potential as a supportive ergonomic intervention for occupational tasks involving stair negotiation. Notably, these positive outcomes were observed despite the exoskeleton’s additional 5.6 kg of mass, demonstrating a net physiological benefit even in demanding vertical tasks where added weight might otherwise be expected to increase strain. Future research should explore the long-term effects of exoskeleton use across more diverse occupational populations and environmental conditions.
Supporting information
S1 FigPhases of the stair ascent gait cycle.Illustration of the seven phases of stair ascent. The leading leg is shown in orange. This schematic supports the kinematic segmentation described in the Methods section.(TIF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Eurofound and International Labour Organization. Working conditions in a global perspective. Publications Office of the European Union, Luxembourg, and International Labour Organization, Geneva; 2019. 196 p. Available from: https://www.eurofound.europa.eu/publications/report/2019/working-conditions-in-a-global-perspective
- 2da Costa BR, Vieira ER. Risk factors for work-related musculoskeletal disorders: a systematic review of recent longitudinal studies. Am J Ind Med. 2010;53(3):285–323. doi: 10.1002/ajim.20750 19753591 · doi ↗ · pubmed ↗
- 3Farioli A, Mattioli S, Quaglieri A, Curti S, Violante FS, Coggon D. Musculoskeletal pain in Europe: the role of personal, occupational, and social risk factors. Scand J Work Environ Health. 2014;40(1):36–46. doi: 10.5271/sjweh.3381 24009006 PMC 3964819 · doi ↗ · pubmed ↗
- 4Garcia M-G, Graf M, Läubli T. Lower limb pain among workers: a cross-sectional analysis of the fifth European Working Conditions Survey. Int Arch Occup Environ Health. 2017;90(7):575–85. doi: 10.1007/s 00420-017-1220-4 28417255 PMC 5934451 · doi ↗ · pubmed ↗
- 5Nieminen LK, Pyysalo LM, KankaanpääMJ. Prognostic factors for pain chronicity in low back pain: a systematic review. Pain Rep. 2021;6(1):e 919. doi: 10.1097/PR 9.0000000000000919 33981936 PMC 8108595 · doi ↗ · pubmed ↗
- 6Bevan S. Economic impact of musculoskeletal disorders (MS Ds) on work in Europe. Best Pract Res Clin Rheumatol. 2015;29(3):356–73. doi: 10.1016/j.berh.2015.08.002 26612235 · doi ↗ · pubmed ↗
- 7Hulshof CTJ, Pega F, Neupane S, van der Molen HF, Colosio C, Daams JG, et al. The prevalence of occupational exposure to ergonomic risk factors: a systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ Int. 2021;146:106157. doi: 10.1016/j.envint.2020.106157 33395953 · doi ↗ · pubmed ↗
- 8Espinoza MA, Bilbeny N, Abbott T, Carcamo C, Zitko P, Zamorano P, et al. Cost analysis of chronic pain due to musculoskeletal disorders in Chile. P Lo S One. 2022;17(10):e 0273667. doi: 10.1371/journal.pone.0273667 36301984 PMC 9612497 · doi ↗ · pubmed ↗