Optimal upfront surgery for gastric adenocarcinoma. Real life situation in Brazil. Results comparable to neoadjuvant treatment
Augusto Canton GONÇALVES, Rodrigo Silveira RACY, Anna Clara Hebling MITIDIERI, Beny Goulart Dias de CASTRO, Caio de Carvalho ZANON, Wilson Rodrigues FREITAS, Osvaldo Antonio Prado CASTRO, Paulo KASSAB

TL;DR
This study shows that upfront surgery for gastric cancer in Brazil can be as effective as neoadjuvant treatment, especially when combined with adjuvant therapy and D2 dissection.
Contribution
The study demonstrates that optimal upfront surgery achieves similar survival outcomes to neoadjuvant treatment in gastric cancer patients.
Findings
Optimal upfront surgery resulted in similar overall survival to neoadjuvant treatment (56.6% vs. 52.4%).
Preoperative chemotherapy, D2 lymphadenectomy, and complication rates were independent factors influencing survival.
Optimal surgery was achieved in 68.6% of the neoadjuvant group and 51.9% of the upfront group.
Abstract
Complete neoadjuvant treatment for gastric cancer is not always tolerated due to nutritional and clinical reasons, such as gastric outlet obstruction. In this context, upfront surgery becomes an alternative. The aim of the study was to compare upfront resection with neoadjuvant systemic therapy followed by surgery and identify factors influencing their outcomes. Retrospective study of 410 patients with locally advanced gastric adenocarcinoma followed between 2012 and 2020, comparing upfront surgery and perioperative treatment. Patients with early tumor (cT1N0), metastasis, and stump cancer were excluded. The comparison was stratified by stage without the influence of systemic treatment (primary stage). Resections with D2 dissection, no residual tumor (no R2), and no complications were considered optimal surgery. Upfront resection was performed in 216 patients (85% of upfront…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
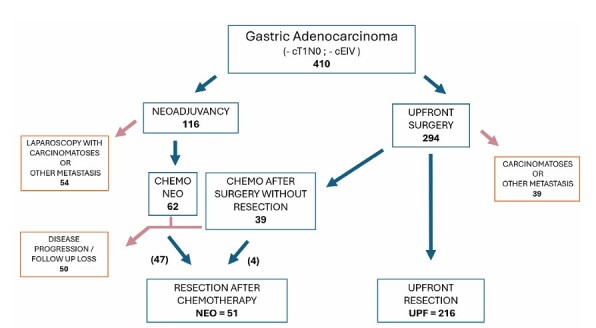 Figure 1
Figure 1| Characteristics | UPF | NEO | p-value | |
|---|---|---|---|---|
| n=216 | n=51 | |||
| Age (years) | ||||
| Mean (SD) | 61.8 (12.8) | 58.0 (10.9) | 0.05 | |
| Median (min–max) | 63 (24–92) | 57 (30–78) | ||
| Lauren’s type (%) | ||||
| Diffuse | 138 (63.9) | 24 (47.1) | 0.086 | |
| Intestinal | 72 (33.3) | 25 (49.0) | ||
| Mixed | 6 (2.8) | 2 (3.9) | ||
| Primary stage (pUPF x cNEO) (%) | ||||
| Initial | 78 (36.1) | 14 (27.5) | 0.242 | |
| More advanced | 138 (63.9) | 37 (72.5) | ||
| Lymphadenectomy (%) | ||||
| D1 | 82 (38.0) | 13 (25.5) | 0.094 | |
| D2 | 134 (62.0) | 38 (74.5) | ||
| Lymphadenectomy D2—8a/9/11p dissection (%) | ||||
| Absent | 14 (10.4) | 3 (7.9) | 0.767 | |
| Present | 120 (89.6) | 35 (92.1) | ||
| Lymphadenectomy D1—8a/9/11p dissection (%) | ||||
| Absent | 71 (86.6) | 10 (76.9) | 0.4 | |
| Present | 11 (13.4) | 3 (23.1) | ||
| D1 resected lymph nodes | ||||
| Mean (SD) | 20.3 (10.2) | 20.2 (9.2) | 0.918 | |
| Median (IQR) | 20 (12–27) | 18 (14–22) | ||
| D2 resected lymph nodes | ||||
| Mean (SD) | 34.5 (14.9) | 36,5 (11.9) | 0.205 | |
| Median (IQR) | 31 (24–43) | 34 (29–48) | ||
| (y)pN (%) | ||||
| (y)pN0 | 45 (20.8) | 31 (60.8) | <0.001 | |
| (y)pN+ | 171 (79.2) | 20 (39.2) | ||
| Surgery (%) | ||||
| Subtotal gastrectomy | 171 (79.2) | 24 (47.1) | <0.001 | |
| Total gastrectomy | 45 (20.8) | 27 (52.9) | ||
| Multivisceral surgery (%) | ||||
| No | 193 (89.4) | 46 (90.2) | 0.86 | |
| Yes | 23 (10.6) | 5 (9.8) | ||
| Residual tumor (R2) (%) | ||||
| No | 201 (93.1) | 50 (98.0) | 0.322 | |
| Yes | 15 (6.9) | 1 (2.0) | ||
| Complications (%) | ||||
| No | 179 (82.9) | 47 (92.2) | 0.098 | |
| Yes | 37 (17.1) | 4 (7.8) | ||
| Complications – Leaks (%) | ||||
| No | 199 (92.1) | 51 (100) | 0.05 | |
| Yes | 17 (7.9) | 0 | ||
| Clavien-Dindo (%) | ||||
| No complication | 179 (82.9) | 47 (92.2) | 0.265 | |
| I/II | 15 (6.9) | 2 (3.9) | ||
| III/IV/V | 22 (10.2) | 2 (3.9) | ||
| Optimal surgery (%) | ||||
| No | 104 (48.1) | 16 (31.4) | 0.03 | |
| Yes | 112 (51.9) | 35 (68.6) | ||
| General characteristics | UPF | NEO | p-value | ||
|---|---|---|---|---|---|
| n=216 | n=51 | ||||
| Age (years) | |||||
| Mean (SD) | 61.8 (12.8) | 58.0 (10.9) | 0.050
| ||
| Median (min–max) | 63 (24–92) | 57 (30–78) | |||
| Sex (%) | |||||
| Female | 88 (40.7) | 17 (33.3) | 0.330
| ||
| Male | 128 (59.3) | 34 (66.7) | |||
| Tumor center gastric segment (%) | |||||
| Low centered | 141 (65.3) | 18 (35.3) | <0.001
| ||
| Middle centered | 45 (20.8) | 12 (23.5) | |||
| Upper centered | 30 (13.9) | 21 (41.2) | |||
| Number of affected segments (%) | |||||
| 1 | 132 (61.1) | 37 (72.5) | 0.291
| ||
| 2 | 68 (31.5) | 12 (23.5) | |||
| 3 | 16 (7.4) | 2 (3.9) | |||
| Lauren’s type (%) | |||||
| Diffuse | 138 (63.9) | 24 (47.1) | 0.086
| ||
| Intestinal | 72 (33.3) | 25 (49.0) | |||
| Mixed | 6 (2.8) | 2 (3.9) | |||
| Primary stage (pUPF x cNEO) (%) | |||||
| Initial | 78 (36.1) | 14 (27.5) | 0.242
| ||
| More advanced | 138 (63.9) | 37 (72.5) | |||
| Pathological stage | |||||
| Complete response | 0 | 5 | 0.001
| ||
| IA | 0 | 9 | |||
| IB | 17 | 9 | |||
| IIA | 25 | 5 | |||
| IIB | 36 (36.1%) | 4 (62.7%) | |||
| Initial | |||||
| IIIA | 62 | 11 | |||
| IIIB | 54 | 6 | |||
| IIIC | 22 (63,9%) | 2 (37,3%) | |||
| Lymphadenectomy characteristics | UPF | NEO | p-value | |
|---|---|---|---|---|
| Resected lymph nodes | ||||
| Mean (SD) | 29.1 (15.0) | 32.4 (13.3) | 0.066
| |
| Median (min–max) | 27 (2–86) | 32 (8–56) | ||
| Affected lymph nodes | ||||
| Mean (SD) | 5.9 (7.5) | 2.8 (5.5) | <0.001
| |
| Median (min–max) | 4 (0–51) | 0 (0–25) | ||
| Lymphadenectomy (%) | ||||
| D1 | 82 (38.0) | 13 (25.5) | 0.094
| |
| D2 | 134 (62.0) | 38 (74.5) | ||
| Lymphadenectomy D2 – 8a/9/11p dissection (%) | ||||
| Absent | 14 (10.4) | 3 (7.9) | 0.767
| |
| Present | 120 (89.6) | 35 (92.1) | ||
| Lymphadenectomy D1 – 8a/9/11p dissection (%) | ||||
| Absent | 71 (86.6) | 10 (76,9) | 0.400
| |
| Present | 11 (13.4) | 3 (23.1) | ||
| D1 resected lymph nodes | ||||
| Mean (SD) | 20.3 (10.2) | 20.2 (9.2) | 0.918
| |
| Median (IQR) | 20 (12–27) | 18 (14–22) | ||
| D2 resected lymph nodes | ||||
| Mean (SD) | 34.5 (14.9) | 36.5 (11.9) | 0.205
| |
| Median (IQR) | 31 (24–43) | 34 (29–48) | ||
| (y)pN (%) | ||||
| (y)pN0 | 45 (20.8) | 31 (60.8) | <0.001
| |
| (y)pN+ | 171 (79.2) | 20 (39.2) | ||
| Surgical characteristics | UPF | NEO | p-value | ||
|---|---|---|---|---|---|
| n=216 | n=51 | ||||
| Surgery (%) | |||||
| Subtotal gastrectomy | 171 (79.2) | 24 (47.1) | <0.001
| ||
| Total gastrectomy | 45 (20.8) | 27 (52.9) | |||
| Multivisceral surgery (%) | |||||
| No | 193 (89.4) | 46 (90.2) | 0.860
| ||
| Yes | 23 (10.6) | 5 (9.8) | |||
| Pancreas | 0 | 3 (5.9) | 0.007
| ||
| Liver | 2 (0.9) | 2 (3.9) | 0.166
| ||
| Colon | 7 (32) | 3 (5.9) | 0.409
| ||
| Spleen | 11 (5.1) | 2 (3.9) | 0.999
| ||
| Diaphragm | 3 (1.4) | 0 | 0.999
| ||
| Residual tumor (R2) (%) | |||||
| No | 201 (93.1) | 50 (98.0) | 0.322
| ||
| Yes | 15 (6.9) | 1 (2.0) | |||
| Bleeding (ml) | |||||
| Mean (SD) | 263.9 (149.3) | 371.3 (263.2) | 0.001
| ||
| Median (min-max) | 220 (50–780) | 350 (50–1500) | |||
| Surgery duration (min) | |||||
| Mean (SD) | 209.9 (67.0) | 238.0 (65.3) | 0.016
| ||
| Median (min-max) | 210 (45–390) | 240 (140–480) | |||
| Complications (%) | |||||
| No | 179 (82.9) | 47 (92.2) | 0.098
| ||
| Yes | 37 (17.1) | 4 (7.8) | |||
| Complications – Leaks (%) | |||||
| No | 199 (92.1) | 51 (100) | 0.050
| ||
| Yes | 17 (7.9) | 0 | |||
| Clavien-Dindo (%) | |||||
| No complication | 179 (82.9) | 47 (92.2) | 0.265
| ||
| I/II | 15 (6.9) | 2 (3.9) | |||
| III/IV/V | 22 (10.2) | 2 (3.9) | |||
| Variable | HR non-adjusted (95%CI) | p-value | HR adjusted (95%CI) | p-value | |
|---|---|---|---|---|---|
| Conduct | |||||
| Upfront | 1 | 1 | |||
| Neoadjuvancy | 0.57 (0.36–0.90) | 0.017 | 0.60 (0.38–0.95) | 0.03 | |
| Primary stage | |||||
| Initial | 1 | 1 | |||
| More advanced | 1.65 (1.14–2.37) | 0.007 | 1.62 (1.12–2.34) | 0.01 | |
| Lymphadenectomy | |||||
| D1 | 1 | 1 | |||
| D2 | 0.60 (0.43–0.83) | 0.002 | 0.63 (0.45–0.87) | 0.005 | |
| Complications | |||||
| No | 1 | 1 | |||
| Yes | 2.19 (1.47–3.25) | <0.001 | 2.04 (1.37–3.03) | <0.001 | |
| Pathological stage | |||||
| 0–II | 1 | ||||
| III | 2.25 (1.58–3.20) | <0.001 | |||
| Angiolymphatic invasion | |||||
| No | 1 | ||||
| Yes | 2.12 (1.37–3.28) | 0.001 | |||
| Perineural invasion | |||||
| No | 1 | ||||
| Yes | 1.79 (1.23–2.61) | 0.002 | |||
| Age (years) | 1.02 (1.01–1.04) | <0.001 | |||
| Variable | HR non adjusted (95%CI) | p-value | |||
| Gastrectomy | |||||
| Subtotal | 1 | ||||
| Total | 1.39 (0.99–1.97) | 0.059 | |||
| Lauren’s type | |||||
| Diffuse | 1 | ||||
| Intestinal | 0.79 (0.56–1.11) | 0.171 | |||
| Mixed | 0.97 (0.36–2.62) | 0.944 | |||
| Multivisceral surgery | |||||
| No | 1 | ||||
| Yes | 1.29 (0.78–2.13) | 0.328 | |||
| Tumor center | |||||
| Lower | 1 | ||||
| Middle | 1.06 (0.72–1.58) | 0.76 | |||
| Upper | 0.93 (0.60–1.43) | 0.733 | |||
| Bleeding (mL) | 1.001 (1.000–1.002) | 0.207 | |||
| Surgery duration (min) | 0.998 (0.996–1.001) | 0.149 | |||
| Sex | |||||
| Female | 1 | ||||
| Male | 0.94 (0.68–1.31) | 0.728 | |||
| Variable | Mean survival time (months) | Overall survival probability | p-value | |||
|---|---|---|---|---|---|---|
| 1 year | 3 years | 5 years | ||||
| Upfront (n=216) | ||||||
| Lymphadenectomy (%) | ||||||
| D1 | 27 | 63.10 | 30.90 | 28.30 | <0.001 | |
| D2 | 39.5 | 80.60 | 58.00 | 48.30 | ||
| Gastrectomy (%) | ||||||
| Subtotal | 36.5 | 78.30 | 51.00 | 43.30 | 0.043 | |
| Total | 28.4 | 57.80 | 35.60 | 30.80 | ||
| Complications (%) | ||||||
| No | 37.7 | 78.70 | 52.60 | 43.90 | <0.001 | |
| Yes | 20.8 | 51.40 | 24.30 | 24.30 | ||
| Complications (%) | ||||||
| No | 37.7 | 78.70 | 52.60 | 43.90 | <0.001 | |
| Yes | 20.8 | 51.40 | 24.30 | 24.30 | ||
| pN (%) | ||||||
| pN0 | 43.4 | 82.20 | 71.10 | 59.50 | 0.008 | |
| pN+ | 32.5 | 71.80 | 41.50 | 35.60 | ||
| Primary stage (pathological) (%) | ||||||
| IB-II | 41 | 79.50 | 64.10 | 54.20 | 0.005 | |
| III | 31.2 | 70.80 | 38.40 | 33.00 | ||
| Optimal surgery (%) | ||||||
| No | 26.1 | 60.40 | 30.20 | 28.10 | <0.001 | |
| Yes | 42.9 | 86.60 | 64.00 | 52.40 | ||
| Neoadjuvancy (n=51) (%) | ||||||
| Lymphadenectomy | ||||||
| D1 | 47.8 | 92.30 | 76.90 | 68.40 | 0,369 | |
| D2 | 42.3 | 81.60 | 65.70 | 57.50 | ||
| Gastrectomy (%) | ||||||
| Subtotal | 48.2 | 91.70 | 79.20 | 65.20 | 0,239 | |
| Total | 39.7 | 77.80 | 59.30 | 47.60 | ||
| Complications (%) | ||||||
| No | 43.6 | 85.10 | 68.00 | 59.00 | 0,81 | |
| Yes | 45 | 75.00 | 75.00 | 37.50 | ||
| ypN (%) | ||||||
| ypN0 | 52.5 | 90.30 | 87.10 | 83.70 | <0,001 | |
| ypN+ | 29.9 | 75.00 | 39.40 | 15.00 | ||
| Primary stage (clinical) (%) | ||||||
| I*/II | 47.6 | 92.90 | 71.40 | 64.30 | 0,532 | |
| III/IVa | 42.3 | 81.10 | 67.60 | 54.30 | ||
| Optimal surgery (%) | ||||||
| No | 46.4 | 87.50 | 75.00 | 60.60 | 0,646 | |
| Yes | 42.5 | 82.90 | 65.60 | 56.60 | ||
| Pathological stage (%) | ||||||
| 0–II | 52.5 | 90.60 | 90.60 | 73.20 | <0,001 | |
| III | 29 | 73.70 | 30.70 | 30.70 | ||
| Variable | OR non-adjusted (95%CI) | p-value | OR adjusted (95%CI) | p-value | |
|---|---|---|---|---|---|
| Age (ref.>62 years)
| 1 | 1 | |||
| ≤62 years | 3.53 (2.00–6.24) | <0.001 | 3.73 (2.00–6.97) | <0.001 | |
| Sex (ref. Male) | 1 | ||||
| Female | 1.31 (0.76–2.28) | 0.337 | |||
| Stage (ref. More advanced) | 1 | 1 | |||
| Initial | 1.47 (0.84–2.59) | 0.182 | 1.66 (0.88–3.12) | 0.118 | |
| Gastrectomy (ref. Subtotal) | 1 | 1 | |||
| Total | 1.79 (0.90–3.56) | 0.095 | 3.40 (1.28–9.08) | 0.014 | |
| Multivisceral (ref. Yes) | 1 | 1 | |||
| No | 1.68 (0.68–4.11) | 0.259 | 3.38 (1.06–10.73) | 0.039 | |
| Main segment (ref. L) | 1 | ||||
| Segment M | 1.42 (0.72–2.83) | 0.314 | |||
| Segment U | 1.06 (0.47–2.35) | 0.894 | |||
| Number of segments (ref. 1) | 1 | 1 | |||
| 2 | 1.65 (0.91–3.02) | 0.102 | 1.27 (0.64–2.49) | 0.497 | |
| 3 | 0.82 (0.29–2.32) | 0.703 | 0.20 (0.05–0.84) | 0.028 | |
| Histology (ref. Intestinal) | 1 | 1 | |||
| Diffuse | 1.93 (1.08–3.44) | 0.026 | 2.04 (1.07–3.91) | 0.031 | |
| Angiolymphatic inv. (ref. Yes) | 1 | ||||
| No | 1.22 (0.61–2.46) | 0.579 | |||
| Perineural inv. (ref. Yes) | 1 | ||||
| No | 0.75 (0.40–1.39) | 0.355 | |||
| Variable | OR non-adjusted (95%CI) | p-value | OR adjusted (95%CI) | p-value | |
|---|---|---|---|---|---|
| Age (ref.>62 years)
| 1 | 1 | |||
| ≤62 years | 7.28 (2.28–23.30) | 0.001 | 9.57 (2.76–33.20) | <0.001 | |
| Sex (ref. Male) | 1 | ||||
| Female | 3.21 (1.01–10.23) | 0.048 | |||
| Stage (ref. More advanced) | 1 | ||||
| Initial | 1.62 (0.58–4.52) | 0.361 | |||
| Gastrectomy (ref. Subtotal) | 1 | ||||
| Total | 1.37 (0.42–4.43) | 0.604 | |||
| Multivisceral (ref. Yes) | 1 | ||||
| No | 3.74 (1.10–12.68) | 0.034 | |||
| Main segment (ref. L) | 1 | 1 | |||
| Segment M | 0.34 (0.12-0.96) | 0.042 | 0.22 (0.07–0.71) | 0.012 | |
| Segment U | 0.58 (0.14-2.45) | 0.458 | 0.62 (0.13–2.82) | 0.533 | |
| Number of segments (ref. 1) | 1 | ||||
| 2 | 1.59 (0.52–4.84) | 0.102 | |||
| 3 | 0.45 (0.10–2.00) | 0.703 | |||
| Histology (ref. Intestinal) | 1 | ||||
| Diffuse | 1.78 (0.66–4.76) | 0.254 | |||
| Angiolymphatic inv. (ref. Yes) | 1 | ||||
| No | 4.81 (0.61–37.87) | 0.136 | |||
| Perineural inv. (ref. Yes) | 1 | ||||
| No | 0.93 (0.31–2.80) | 0.895 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Esophageal Cancer Research and Treatment
INTRODUCTION
Despite the recent increase in cardia tumors, the distal stomach remains an important site of gastric adenocarcinoma^ 16 ,21,23 ,26 ^. Due to the high rate of late diagnoses, patients’ nutritional status is commonly affected, sometimes with gastric outlet obstruction, which often requires intervention before systemic treatment^ 5,6,14,17 ^. Patient morbidity, costs, side effects, and variable response rates also hinder the decision for neoadjuvant treatment. In this context, upfront surgery becomes an alternative. From 2013 to 2024, 85.7% of gastric cancer surgeries in the Brazilian public health system were performed within 60 days of the diagnosis, whereas only 52.5% of patients referred for chemotherapy started the treatment within this period^ 24 ^ . The objective of this study is to compare upfront resection with neoadjuvant systemic therapy followed by surgery and to identify factors influencing their outcomes.
METHODS
The study is a retrospective analysis of patients with locally advanced gastric adenocarcinoma followed between 2012 and 2020 at a single center, comparing upfront surgery and preoperative chemotherapy treatment. Patients with clinical diagnoses of early tumor (cT1N0), distant metastasis, and stump cancer were initially excluded. After staging laparoscopy or laparotomy, patients with unexpected carcinomatosis or other metastases were also excluded.
The treatment percentage in each group was calculated by dividing the total number of resections by the number of indicated patients, excluding cases with unexpected metastasis. Overall survival (OS) at 60 months was compared between the resections performed in an upfront (UPF) surgery setting and surgery following systemic treatment (neoadjuvant [NEO]), including resection cases with initial unsuccessful laparotomy attempts. The proposed treatment for each patient was chosen in routine tumor board meetings, considering tumor characteristics, patient clinical and social characteristics, such as conditions for regular transportation, family support, patient understanding and commitment to therapy. If possible, patients with more advanced tumors were intended to be referred for NEO treatment, but obstructive symptoms and social aspects frequently directed them to surgery. Lymphadenectomy D1 or D2 was defined by the surgeon based on intraoperative feasibility, where D1 was only performed when radical dissection was considered unsafe. Further postoperative analyses were performed, considering "true D2," the cases with dissection of at least stations 8a, 9, and 11p on the pathology report, whereas "true D1" was considered when it involved only perigastric nodes and station 7. Resections with D2 dissection, no residual tumor (no R2), and no complications were considered optimal surgery. As a retrospective study, these analyses did not influence treatment decisions.
Tumor staging was based on the TNM (Tumor, Lymph Node, Metastasis) 8th edition^ 3 ^ . For clinical staging of lymph nodes, the criteria used by Fukagawa et al.^ 10 ^ were applied. Nodes with a long axis=10 mm or a short axis=8 mm on tomography were considered positive. If the tumor depth was not defined by tomography, the endoscopic criteria of 6 cm size for more advanced lesions, used by Tanaguchi et al.^ 25 ^ , were applied. First, the entire cohort from both arms was compared, which was also adopted in prospective randomized studies^ 8,27 ^. Second, to stratify the comparison between NEO and UPF by stage without the influence of systemic treatment, the clinical classification was used for NEO and the pathological classification for UPF, named the primary stage. NEO clinical stages cE I–II and UPF pathological stages pE IB–II were considered initial tumors. NEO clinical stages III–IVa and UPF pathological stage III were considered more advanced tumors.
Perioperative chemotherapy mainly consisted of protocols based on either Capecitabine or Epirubicin (XELOX or ECF). Most patients in the UPF group received postoperative MacDonald or XELOX protocol. Multivisceral surgery was defined by the resection of at least one of the following organs: colon, liver, pancreas, spleen, or diaphragm. The majority of patients (90%) were followed for at least 60 months, and the minimum period was 45 months. All data were obtained from the Esophagogastric and Bariatric Surgery Division of Santa Casa de São Paulo.
Patient characteristics were presented through frequencies and percentages for qualitative variables and by mean, median, standard deviation, minimum, and maximum values for quantitative variables. Association between qualitative variables was evaluated by Pearson’s ꭓ^2^ test or Fisher’s exact test (when 25% or more of the expected values were less than 5). The comparison between two groups for quantitative variables was assessed by Student’s t-test or Mann-Whitney test (if the data did not follow a normal distribution). In the overall survival analysis, the time from surgery to death or last information was calculated; patients alive at the end of follow-up were considered "censored." Survival curves were constructed using the Kaplan-Meier method and compared through the log-rank test. Additionally, Cox regression was used to calculate the hazard ratio (HR) and respective 95% confidence intervals. Finally, both unadjusted and adjusted HR values, according to variables of interest, were presented. Binary logistic regression was utilized to evaluate factors related to optimal surgery. Odds ratios (ORs) and 95% confidence intervals (95%CIs) were calculated for each variable of interest and presented through unadjusted and adjusted OR values. The analyses were performed using the statistical software SPSS for Windows v.25 and Stata v.14 for Windows. The study was approved by the Ethics Committee of the Institution (CAAE number 69680423.6.000).
RESULTS
During the study period, 410 patients with locally advanced gastric cancer attended our institution. Two-hundred and ninety-four patients were referred directly to surgery, and 39 of them had unexpected metastasis. Of the remaining 254, upfront resection (UPF) was performed in 216 (85%). In the NEO group with 116 patients, the staging laparoscopy detected metastasis in 54. Out of 62 patients, 47 (76%) underwent gastrectomy after neoadjuvancy, and another four were resected among 39 previous unsuccessful resection attempts (10%). In total, there were 51 resections after chemotherapy (NEO) (Figure 1).
Study flowchart.
UPF and NEO had similar mean ages of 61.8 and 58.0 (p=0.05). In both groups, male patients were more frequent. More advanced primary stage (pEIII) corresponded to 72.5% of UPF cases, and in NEO (cEIII and IVa), they were 63.9% of the patients, without statistical significance (p=0.242). The tumor size distribution, based on the number of affected stomach segments, was similar in UPF and NEO. The frequency of subtotal gastrectomies was 79.2% in UPF, with 65.3% of lower-centered tumors, whereas in NEO, subtotal resections represented 47.1% of cases (p<0.001), with 35.3% of the main portion of lesions in the distal stomach. There was no statistically significant difference in Lauren’s histological type, but NEO had 63.9% of diffuse cell adenocarcinoma, more than UPF with 47.1% (p=0.086). Complete pathological response corresponded to 9.8% of NEO patients, and ypN0 was observed in 60.8% of cases. The percentage of D2 lymphadenectomy was 62.0% in UPF and 74.5% in NEO, with no statistically significant difference (p=0.094). Among D2 surgeries, D2 with 8a/9/11p dissection was also similar in UPF and NEO, with 89.6% and 92.1% (p=0.767), as was D1 without 8a/9/11p among D1 surgeries, with 86.6% and 76.9% (p=0.400), respectively. The mean number of resected lymph nodes had no statistically significant difference between the two groups, with 29.1 in UPF and 32.4 in NEO (p=0.066, p>0.05). When analyzed separately by type of lymphadenectomy, numbers were also similar for both D1 (UPF with 20.2 vs. NEO with 20.4 resected nodes, p=0.918, p>0.05), and D2 (UPF with 34.5 vs. NEO with 36.6, p=0.205). Patients, main characteristics are presented in Table 1, and the complete data are presented in Tables 2, 3, and 4.
Considering all resected patients, the independent prognostic factors for overall survival at 60 months (OS) were: preoperative treatment, where NEO had better outcomes, with 57.3% compared to 40.7% in the UPF group (HR=0.60, p=0.029, p<0.05); complication rate (HR=1.99, p=0.001, p<0.05); D2 lymphadenectomy (HR=0.63, p=0.006, p<0.05); and primary stage (HR=1.62, p=0.010, p<0.05). Table 5 and 6 show the main variables associated with OS. UPF and NEO groups demonstrated no statistically significant difference in the survival curves for initial tumors (p=0.447, p>0.05), which was observed in the more advanced tumors group (p=0.027, p<0.05).
The UPF group had a lower bleeding rate and shorter procedures, but it demonstrated higher complication rates of 17.1% vs. 7.8% without a statistically significant difference (p=0.098, p>0.05). Among all UPF patients, the complications were characterized by 7.9% of anastomotic or stapler leaks and a 10.2% rate of Clavien-Dindo III or higher, including a 6% mortality rate, which was not seen in NEO (0%). Both UPF and NEO had around 10% of multivisceral resections, but with different distributions of affected organs. UPF had more R2 surgeries, with 6.9% vs. 2.0%, without statistical significance (p=0.322, p>0.05).
Lymphadenectomy showed different outcomes in UPF, as in this group, D1 dissection had an OS of 28.3 vs. 48.3% with D2 dissection (p<0.001). The difference was not as large in the NEO group, with OS of 68.4% for D1 and 57.5% for D2 surgeries (p=0.369, p>0.05). Consequently, UPF and NEO had similar survival curves with D2 dissection (p=0.586, p>0.05) and different curves with D1 dissection (p=0.011, p<0.05). Optimal surgery represented 68.6% of NEO and 51.9% of UPF (p=0.030, p>0.05) and had similar OS curves in both groups (p=0.904, p>0.05).
We analyzed a UPF group of 210 patients, examining preoperatively predictable variables in relation to optimal surgery. Independent associated variables were age (less than 62 years), total gastrectomy, no multivisceral surgery, no three-segment tumor, and diffuse type (Table 7). Additionally, we assessed variables linked to increased complications in patients who underwent radical surgery (D2 lymphadenectomy without R2 resection, n=130) (Table 8).
DISCUSSION
Since the publication of the MAGIC trial in 2006^ 8 ^ , preoperative chemotherapy for gastric adenocarcinoma has improved, and its benefit in Western countries was further confirmed by FLOT trial in 2019^ 1,2 ^. Other Brazilian studies were compatible with our analysis, and they have also shown the advantage of preoperative chemotherapy in those patients that complete treatment, despite problems with patients’ poor conditions and health care systems^ 7,11,18 ^. Gastric outlet obstruction is one of the most important factors leading to the decision for upfront surgery in gastric cancer^ 5,6 ,14,17 ^, and it has been described as a worse prognostic factor for non-metastatic cases^ 6,14,17 ^. Unsurprisingly, our study identified more distal tumors, reflecting the necessity of intervention in patients with gastric outlet obstruction. The response to NEO therapy, considering the ypN0 rate and the absence of residual tumor percentage, was comparable to the literature, ranging from 31^ 8 ^ to 59%^ 1 ^ and from 3.0^ 26 ^ to 16%^ 1 ^ respectively. As expected, this response to preoperative chemotherapy was more beneficial for more advanced tumors, which contributes to validate the adopted stratification criteria.
In our study, UPF presented a higher complication rate than NEO, including Clavien-Dindo III or higher, which was not seen in other studies^ 8,11,20,27 ^. Although not all preoperative data were available, UPF patients might have had a worse clinical condition and nutritional status, due to obstructive disease. This may also be caused by the selection effect of neoadjuvancy. Patients operated on in the NEO group had already managed to overcome chemotherapy toxicity to be fit for surgery, representing a less vulnerable population, which is suggested by the lower percentage of patients reaching surgery in this group. This difference was also present in prospective trials^ 8,27 ^.
D2 dissection was an important prognostic factor in the UPF group, which was not seen in the NEO. The equivalent quality of lymphadenectomy was verified by the similar proportion of nodes resected during D1 and D2 surgeries in both groups, and they also had a similar percentage of D2 with 8a/9/11p and D1 without 8a/9/11p, which was adopted to verify more precisely "true" D1 and D2 lymphadenectomy postoperatively. Previous studies have contributed to this discussion in the upfront surgery setting^ 9 ,12,22 ^, but there are few studies concerning surgery radicality after the rise of preoperative chemotherapy.
The parameters used for optimal surgery are contemplated in the study of benchmarks for adenocarcinoma gastrectomies^ 19 ^ . When patients underwent optimal surgery, there were no statistical survival differences between UPF and NEO, which contributes to the discussion about the selection of patients who benefit from preoperative chemotherapy. In addition, the lower percentage of patients reaching surgery in NEO is also relevant, pointing out the importance of the upfront alternative. It may be considered in a high incidence of obstructive distal tumors scenario, but also in the context of primary initial tumors, where UPF was also demonstrated to be not statistically inferior to NEO. This reflects the need for more prospective studies with primary stage stratification. Nevertheless, upfront surgeries had more morbidity, and together with the necessity of D2 dissection, they might become riskier.
The analysis of preoperatively predictable variables within the UPF group reveals which patients had a better chance of optimal upfront surgery. While tumor location and stage were not statistically significant, three-segment tumors showed a worse outcome. Total gastrectomy, the absence of multivisceral surgery, and age were also independent factors for optimal surgery. It is important to consider that performing radical surgery (D2 lymphadenectomy without R2 resection) involves the surgeon’s intraoperative decisions. Objectively, we also analyzed the variables related to complication rate exclusively in patients who underwent radical surgery. The only independent factor that remained statistically significant in both analyses was age younger than 62 years. This suggests a greater relevance of the patient’s clinical condition over the tumor characteristics themselves for the likelihood of optimal procedures when focusing solely on the upfront surgery setting. However, this must be interpreted carefully, as larger lesions may indirectly affect a patient’s overall status, and older patients may also have poorer conditions for receiving chemotherapy, necessitating a tailored decision-making process. In the literature, more advanced stages and total gastrectomies are associated with a higher incidence of complications^ 4,15 ^, while middle segment tumors are linked with better prognoses, though the association with complications is not widely described^ 13 ^ . These differences from our results warrant further investigation with a larger patient cohort and more comprehensive preoperative factors, but this certainly provides a promising direction for future research.
Regarding the implications for practice, we acknowledge that the current standard in many Western countries favors NEO treatment for advanced tumors when feasible. However, the reality of needing to perform upfront surgery, whether due to obstructive symptoms or patients’ poor clinical and support conditions for receiving chemotherapy, necessitates a deeper understanding of this approach. Our study aimed to explore these scenarios, and our conclusions about optimal surgery point out that by verifying its likelihood preoperatively, it might be possible to better select patients for systemic treatment to avoid the risk of progression and side effects. Conversely, another practical conclusion is the need to identify unexpected intraoperative findings that hinder safe, optimal surgery. In this situation, surgeons may consider not advancing to resections, evaluating nutritional procedures, such as gastroenterostomies or jejunostomies, and directing the patient to NEO treatment.
As a retrospective study, our analyses had some limitations. Imprecise clinical staging, which is a major concern in gastric cancer treatment decisions, is also expected in our study, and some staging exams were performed at different institutions before the patients were referred to our service. The preoperative chemotherapy started mainly in 2017 in our institution, leading to a smaller group of these patients. During the study period, systemic protocols were changed, with variable complete treatment rates, which corresponds to a bias. Comorbidities and body mass index information were frequently missing and could not be used.
We debated the use of propensity score matching, and we concluded that it might not be the most suitable approach given the smaller number of patients in the NEO arm, which could limit statistical power. Key baseline characteristics (age, primary stage, histological type, lymphadenectomy, multivisceral surgery, and residual tumor rate) were not statistically different between the groups. The higher incidence of distal tumors and subtotal gastrectomies in the UPF group, within a context of more advanced stages, might suggest a higher proportion of obstructive tumors and patients with poorer base line status. However, even in this context, the outcomes of optimal upfront surgery were similar to those of NEO treatment.
CONCLUSIONS
Optimal upfront surgery followed by adjuvant therapy, particularly with D2 dissection, is effective and was not statistically inferior to NEO treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al-Batran SE Hofheinz RD Pauligk C Kopp HG Haag GM Luley KB Histopathological regression after neoadjuvant docetaxel, oxaliplatin, fluorouracil, and leucovorin versus epirubicin, cisplatin, and fluorouracil or capecitabine in patients with resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT 4-AIO): results from the phase 2 part of a multicentre, open-label, randomised phase 2/3 trial Lancet Oncol 20161712169770810.1016/S 1470-2045(16)30531-927776843 · doi ↗ · pubmed ↗
- 2Al-Batran SE Homann N Pauligk C Goetze TO Meiler J Kasper S Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT 4): a randomised, phase 2/3 trial Lancet 20193931018419485710.1016/S 0140-6736(18)32557-130982686 · doi ↗ · pubmed ↗
- 3Amin MB Edge SB Gress DM Meyer LR AJCC cancer staging manual American Joint Committee on Cancer Chicago American Joint Committee on Cancer 2017
- 4Baiocchi GL Giacopuzzi S Reim D Piessen G Costa PMD Reynolds JV Incidence and grading of complications after gastrectomy for cancer using the GASTRODATA registry: a European retrospective observational study Ann Surg 202027258071310.1097/SLA.000000000000434132925254 · doi ↗ · pubmed ↗
- 5Blumenthaler AN Ikoma N Blum M Das P Minsky BD Mansfield PF Relationship between initial management strategy and survival in patients with gastric outlet obstruction due to gastric cancer J Surg Oncol 2020122713738210.1002/jso.2617732810292 PMC 7722201 · doi ↗ · pubmed ↗
- 6Chen JH Wu CW Lo SS Li AFY Hsieh MC Shen KH Outcome of distal gastric cancer with pyloric stenosis after curative resection Eur J Surg Oncol 20073355566010.1016/j.ejso.2007.01.02017329063 · doi ↗ · pubmed ↗
- 7Coimbra FJF Jesus VHF Ribeiro HSC Diniz AL Godoy AL Farias IC Impact of yp T, yp N, and adjuvant therapy on survival in gastric cancer patients treated with perioperative chemotherapy and radical surgery Ann Surg Oncol 2019261136182610.1245/s 10434-019-07454-031222685 · doi ↗ · pubmed ↗
- 8Cunningham D Allum WH Stenning SP Thompson JN Van de Velde CJ Nicolson M Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer N Engl J Med 20063551112010.1056/NEJ Moa 05553116822992 · doi ↗ · pubmed ↗