Radiofrequency Catheter Ablation-Induced Gastroparesis and Gastrointestinal Distension
Leizhi Ku, Shengpeng Guo, Xiaojing Ma

TL;DR
This paper discusses a case where a medical procedure caused stomach issues, emphasizing the need for quick diagnosis and treatment.
Contribution
The paper presents a novel case highlighting gastric complications from RFCA and effective treatment with mosapride citrate.
Findings
RFCA can lead to gastroparesis and gastrointestinal distension.
Prompt treatment with gastrokinetic medication like mosapride citrate is effective.
Abstract
Teaching point: The case highlights the importance of identifying gastric complications after RFCA and the need for prompt diagnosis and treatment of gastroparesis with gastrokinetic medication, such as mosapride citrate.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
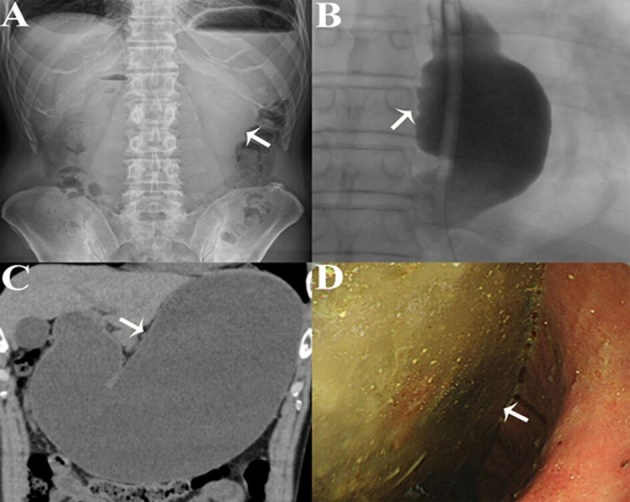 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal motility and disorders · Gastroesophageal reflux and treatments · Bariatric Surgery and Outcomes
Case History
A 56-year-old male was referred to the hospital because of vomiting, epigastric pain, and abdominal distension for 5 days. The patient had a medical history of radiofrequency catheter ablation (RFCA) for persistent atrial fibrillation one week earlier. On physical examination, the abdomen was distended but nontender on palpation. Laboratory examinations were unremarkable. An abdominal X-ray suggested significant gastric distension (Figure 1A). Contrast radiography of the upper gastrointestinal tract showed significant esophageal distension (Figure 1B and Video S1). Abdominal CT revealed marked gastric dilatation without gastric or intestinal obstruction (Figure 1C). Esophagogastroduodenoscopy revealed an abundance of food residue (Figure 1D) and no obstructing cause at the pylorus. Gastroparesis and gastrointestinal distension after catheter ablation for atrial fibrillation were diagnosed. After fasting for several days, the patient was subsequently administered mosapride citrate (5 mg, three times a day). His symptoms gradually improved and resolved completely three months after RFCA.
(A) An abdominal X-ray suggests gastric distension. (B) The X-ray iodine contrast radiography image shows esophageal distension. (C) Abdominal CT revealed gastric dilatation without any gastric or intestinal obstruction. (D) Esophagogastroduodenoscopy reveals an abundance of food residue, and no obstructing lesion at the pylorus.
Comment
Gastroparesis and gastrointestinal distension following RFCA are uncommon extracardiac complications and the most likely mechanism is periesophageal vagal nerve injury. These remain underrecognized complications among gastroenterologists, general physicians, and radiologists, and may be masked by delayed presentation after RFCA. Contrast-enhanced gastric X-ray and plain abdominal CT are essential for accurate diagnosis and timely, appropriate treatment. The characteristic radiographic finding is gastric distension and massive accumulation of food residues [1]. Generally, the management of gastroparesis and gastrointestinal distension is conservative; fasting and bowel rest, gastric decompression, and administration of antiemetics and prokinetic agents are recommended. The case emphasizes the importance of identifying gastric complications after RFC and the need for prompt diagnosis and treatment of gastroparesis with gastrokinetic medication.
The reference list from the paper itself. Each links out to its DOI / PubMed record.