The role of gender in early childcare practices in low- and middle-income countries: a systematic review and meta-analysis
Manzura Jumaniyazova, Eliana Chavarría-Pino, Friederike Suhr, Cecilia Michelle Argueta, Janina Isabel Steinert

TL;DR
This study finds that girls in low- and middle-income countries face gender discrimination in early childcare practices like breastfeeding and immunization, though recent trends suggest some progress toward equality.
Contribution
The study provides the first comprehensive meta-analysis of gender disparities in early childcare practices across low- and middle-income countries.
Findings
Girls experience significant discrimination in breastfeeding and immunization practices in low- and middle-income countries.
Gender disparities are linked to a country’s ranking on the Gender Inequality Index, with higher inequality correlating with worse outcomes for girls.
Recent data suggests a narrowing gender gap in early childcare practices, indicating potential progress toward equity.
Abstract
Gender disparities in early childcare practices impede gender equality and create long-lasting barriers to girls’ health, well-being, and future opportunities. Through this systematic review and meta-analysis, we aimed to quantitatively synthesise evidence on gender disparities in low- and middle-income countries (LMICs) across the World Health Organization’s five components of nurturing care: breastfeeding, immunisation, prenatal check-ups, postnatal check-ups, and healthcare expenditure for children under five. We searched sixteen scientific databases, journals, and repositories in November 2021 and again in January-February 2024, for studies examining gender differences in early childcare practices in LMICs, covering breastfeeding, immunisation, prenatal, and postnatal check-ups, and healthcare expenditure for children under five. We set no restrictions on publication type or date,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
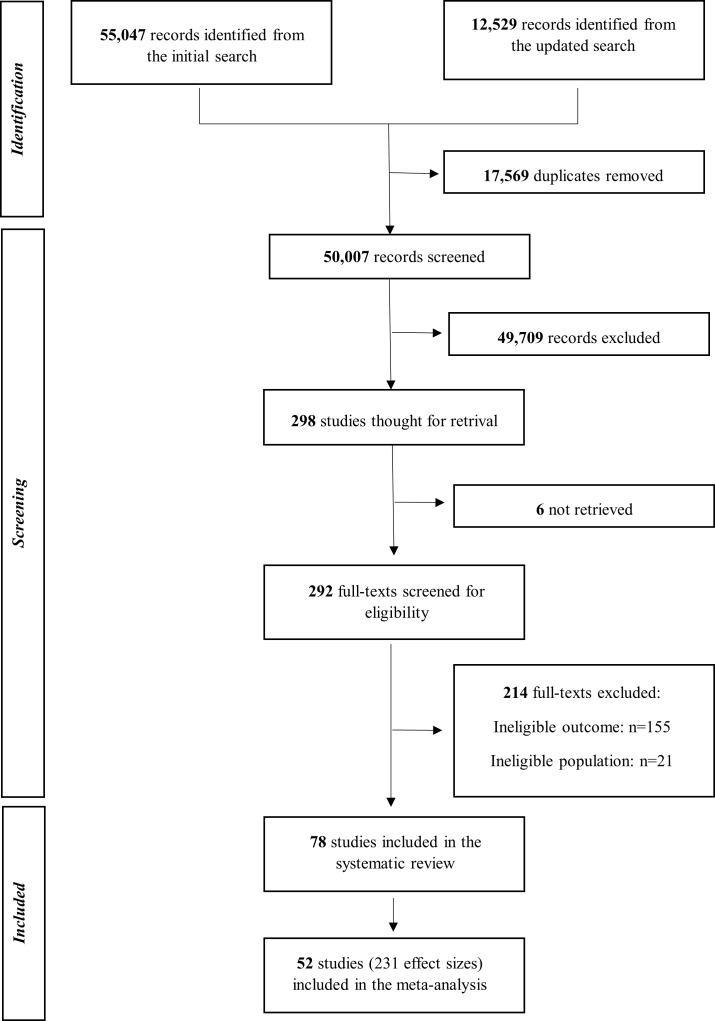 Figure 1
Figure 1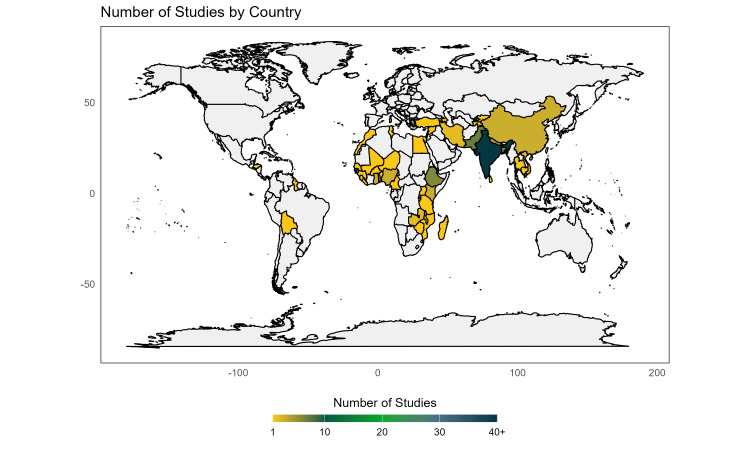 Figure 2
Figure 2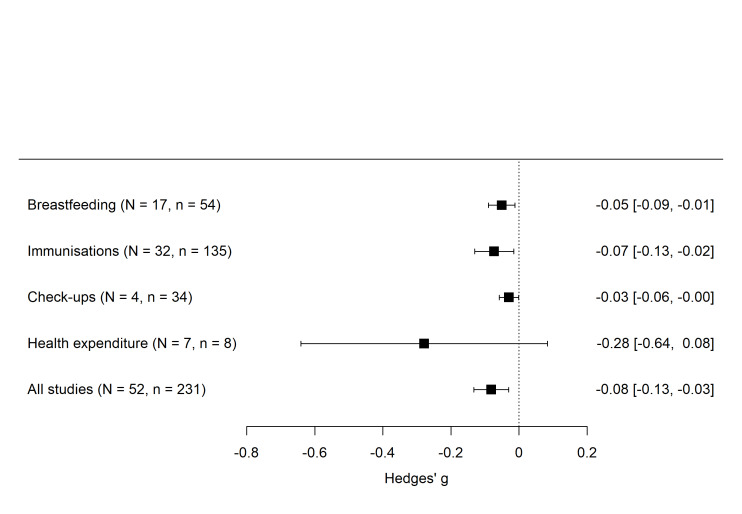 Figure 3
Figure 3| Authors | Type | Year | Country | Region | Sample size | Breastfeeding | Immunisation | Pre- and post-natal check-ups | Healthcare expenditure | Summary for girls | Quality |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Allan | A | 2021 | Kenya | Sub-Saharan Africa | 3943 |
| Y |
|
| No gender differences | 81% |
| Antai [ | A | 2012 | Nigeria | Sub-Saharan Africa | 24 910 |
| Y |
|
| Advantage | 89% |
| Barcellos | A | 2014 | India | South Asia | 110 00 | Y | Y |
|
| Disadvantage | 89% |
| Bharadvaj and Lakdawala [ | A | 2013 | India, China, Bangladesh, Pakistan, Sri Lanka, Thailand, Ghana | Multiple | 36 755 |
|
| Y |
| Disadvantage | 89% |
| Borooah [ | A | 2004 | India | South Asia | 4333 |
| Y |
|
| Disadvantage | 72% |
| Chakravarty [ | A | 2015 | Egypt | Middle East and North Africa | 48 304 | Y |
|
|
| Disadvantage | 67% |
| Chaudhry and Khan [ | A | 2020 | India | South Asia | 105 660 | Y |
| Y |
| No gender differences in breastfeeding; disadvantage in postnatal check-ups. | 67% |
| Chaudhuri [ | A | 2015 | India | South Asia | 777 705 | Y | Y |
|
| No gender differences in breastfeeding; disadvantage in immunisation. | 94% |
| Choi and Lee [ | A | 2006 | India | South Asia | 34 386 |
| Y |
|
| Disadvantage | 100% |
| Chowdhury | A | 2003 | Bangladesh | South Asia | 3570 |
| Y |
|
| Disadvantage | 57% |
| Devasenapathy | A | 2016 | India | South Asia | 1849 |
| Y |
|
| Disadvantage | 94% |
| Dixit | A | 2020 | India | South Asia | 19 2151 |
| Y |
|
| No gender differences | 56% |
| Duraisamy and Duraisamy [ | A | 1995 | India | South Asia | 1272 |
| Y |
|
| No gender differences | 83% |
| Ganatra and Hirve [ | B | 1994 | India | South Asia | 456 |
|
|
| Y | Disadvantage | 72% |
| Geweniger and Abbas [ | A | 2020 | Ethiopia | Sub-Saharan Africa | 2004 |
| Y |
|
| No gender differences | 89% |
| Hajian-Tillaki [ | A | 2005 | Iran | Middle East and North Africa | 600 |
| Y |
|
| No gender differences | 72% |
| Jayachandran and Kuziemko [ | A | 2011 | India | South Asia | 110 000 | Y |
|
|
| Disadvantage | 94% |
| Mahmood | A | 1994 | Pakistan | South Asia | 6558 | Y | Y |
|
| Disadvantage | 64% |
| Mishra | A | 2004 | India | South Asia | 60 125 | Y | Y |
|
| Disadvantage | 78% |
| Nath and Goswami [ | A | 1997 | India | South Asia | 1650 | Y |
|
|
| Disadvantage | 89% |
| Nuruddin | A | 2009 | Pakistan | South Asia | 3740 |
|
|
| Y | No gender differences | 83% |
| Obermeyer and Cardenas [ | A | 1997 | Morrocco, Tunisia | Middle East and North Africa | 6431 | Y | Y |
|
| No gender differences in breastfeeding; disadvantage in immunisation | 78% |
| Pande [ | A | 2003 | India | South Asia | 25 549 |
| Y |
|
| Disadvantage | 78% |
| Pande and Yazbeck [ | A | 2003 | India | South Asia | 89 777 |
| Y |
|
| Disadvantage | 57% |
| Pandey | A | 2002 | India | South Asia | 530 |
|
|
| Y | Disadvantage | 72% |
| Patra [ | W | 2008 | India | South Asia | 304 162 |
| Y |
|
| Disadvantage | 64% |
| Prusty | A | 2014 | India | South Asia | NA |
| Y |
|
| Disadvantage | 61% |
| Rajan and Morgan [ | A | 2018 | India | South Asia | 83 707 | Y | Y |
|
| Disadvantage | 72% |
| Rammohan | A | 2014 | India | South Asia | 22 960 |
| Y |
|
| Disadvantage | 78% |
| Saini | A | 2012 | India | South Asia | 161 |
|
|
| Y | No gender differences | 56% |
| Singh [ | A | 2011 | India | South Asia | NA |
| Y |
|
| No gender differences | 44% |
| Singh [ | A | 2012 | India | South Asia | 5587 |
| Y |
|
| Disadvantage | 89% |
| Singh [ | A | 2013 | India | South Asia | 30 601 |
| Y |
|
| Disadvantage | 83% |
| Singh [ | A | 2019 | India | South Asia | 4811 | Y |
|
|
| Disadvantage | 72% |
| Song | A | 2020 | Nepal | South Asia | 1025 |
| Y |
|
| No gender differences | 61% |
| Srivastava and Navak [ | A | 1995 | India | South Asia | NA |
| Y |
|
| Disadvantage | 29% |
| Swenson | A | 1993 | Vietnam | East Asia and Pacific | 4434 | Y |
|
|
| No gender differences | 50% |
| Vilms | A | 2017 | India | South Asia | 11 570 |
| Y | Y |
| Disadvantage | 83% |
| Willis | A | 2009 | India | South Asia | 255 |
|
|
| Y | Disadvantage | 83% |
| Altinkaynak | A | 2004 | Turkey | Europe and Central Asia | 663 |
| Y |
|
| No gender differences | 64% |
| Arsenault | A | 2017 | Global | Multiple | 63 233 |
| Y |
|
| No gender differences | 81% |
| Bhagyalaxmi | A | 2007 | India | South Asia | 3073 |
| Y |
|
| No gender differences | 39% |
| Bhatia | A | 2004 | India | South Asia | 796 |
| Y |
|
| No gender differences | 50% |
| Corsi | A | 2009 | India | South Asia | 121 110 |
| Y |
|
| Disadvantage | 64% |
| Egondi | A | 2015 | Kenya | Sub-Saharan Africa | 382 |
| Y |
|
| Disadvantage | 50% |
| Gaudin and Yazbeck [ | A | 2006 | India | South Asia | 20 157 |
| Y |
|
| Disadvantage | 64% |
| Hanifi | A | 2018 | Bangladesh | South Asia | 4584 |
| Y |
|
| Disadvantage | 83% |
| Hu | A | 2019 | China | East Asia and Pacific | 847 |
| Y |
|
| No gender differences | 83% |
| Jain and Bongraats [ | A | 2013 | India | South Asia | 1537 | Y |
|
|
| Disadvantage | 67% |
| Joe [ | A | 2015 | India | South Asia | 21 184 |
| Y |
|
| Disadvantage | 56% |
| Selvaraj | A | 2017 | India | South Asia | 110 | Y |
|
|
| Disadvantage | 94% |
| Mugada | A | 2017 | India | South Asia | 377 |
| Y |
|
| Disadvantage | 50% |
| Oster [ | W | 2006 | India | South Asia | 10 854 |
| Y |
|
| Disadvantage | 83% |
| Pillai and Conaway [ | A | 1992 | Zambia | Sub-Saharan Africa | 277 |
| Y |
|
| No gender differences | 67% |
| Pokhrel and Sauerborn [ | A | 2004 | Nepal | South Asia | 8112 |
|
|
| Y | No gender differences | 67% |
| Schoenbaum | A | 1995 | Gaza | Middle East and North Africa | 4051 | Y |
|
|
| No gender differences | 72% |
| Shibre | A | 2020 | Ethiopia | Sub-Saharan Africa | 7951 |
| Y |
|
| No gender differences | 67% |
| Budu | A | 2022 | Ghana | Sub-Saharan Africa | 3650 |
| Y |
|
| Disadvantage | 50% |
| Fekadu | A | 2024 | Ethiopia | Sub-Saharan Africa | 38 500 |
| Y |
|
| No gender differences | 72% |
| Fleddejohann and Channon [ | A | 2022 | Nepal | South Asia | 25648 | Y |
|
|
| Disadvantage | 89% |
| Ghosh | A | 2022 | India | South Asia | 61431 | Y |
|
|
| Disadvantage | 83% |
| Iqbal | A | 2023 | Pakistan | South Asia | 19 894 |
|
| Y |
| Disadvantage | 72% |
| Lai | A | 2023 | China | East Asia and Pacific | 5294 |
| Y |
|
| No gender differences | 83% |
| Magalhães | A | 2022 | Ethiopia | Sub-Saharan Africa | 102 | Y |
|
|
| Advantage | 78% |
| Saikia | A | 2023 | India | South Asia | 43 291 |
| Y |
|
| No gender differences | 72% |
| Samuel | A | 2022 | Ethiopia | Sub-Saharan Africa | 2036 | Y |
|
|
| No gender differences | - |
| Siddiqi | A | 2023 | Pakistan | South Asia | 6 235 305 |
| Y |
|
| Disadvantage | 86% |
| Taneja | A | 2023 | India | South Asia | NA |
| Y |
|
| Disadvantage | 22% |
| Al-Akour | A | 2014 | Syria | Middle East and North Africa | 334 | Y |
|
|
| No gender differences | 89% |
| Joshi | A | 2014 | Bangladesh | South Asia | 121 | Y |
|
|
| No gender differences | 67% |
| Odusanya | A | 2008 | Nigeria | Sub-Saharan Africa | 339 |
| Y |
|
| No gender differences | 67% |
| Parashar [ | A | 2005 | India | South Asia | 5623 |
| Y |
|
| Disadvantage | 100% |
| Partha and Bhattacharya [ | A | 2002 | India | South Asia | 11 748 |
| Y |
|
| Disadvantage | 67% |
| Phukan | A | 2009 | India | South Asia | 616 |
| Y |
|
| No gender differences | 56% |
| Sahu | A | 2010 | India | South Asia | 15 518 |
| Y |
|
| Disadvantage | 72% |
| Vafaee | A | 2010 | Iran | Middle East and North Africa | 1450 | Y |
|
|
| No gender differences | 33% |
| Hafeez and Quintana-Domeque [ | A | 2018 | Pakistan | South Asia | 6955 | Y |
|
|
| Disadvantage | 100% |
| Yan and Ren [ | A | 2019 | China | East Asia and Pacific | 620 | Y | No gender difference | 100% |
| Basic controls | Extended controls | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
| Middle East and North Africa | −0.065 | 3.98 |
|
|
|
|
|
| −0.030 | 11.93 |
|
| 0.070 |
|
|
|
|
|
|
| 0.294 |
|
| Sub-Saharan Africa | 0.003 | 3.5 |
|
|
|
|
|
| −0.385 | 12.44 |
|
| 0.089 |
|
|
|
|
|
|
| 0.377 |
|
| South Asia | −0.115 | 2.33 |
|
|
|
|
|
| −0.389 | 12.43 |
|
| 0.073 |
|
|
|
|
|
|
| 0.375 |
|
| Multiple | −0.028 | 1.99 |
|
|
|
|
|
| −0.238 | 11.22 |
|
| 0.065 |
|
|
|
|
|
|
| 0.245 |
|
|
|
|
| 0.011† | 23.3 |
|
|
|
| 0.022‡ | 7.31 |
|
|
|
| 0.004 |
|
|
|
|
| 0.011 |
|
|
|
|
|
|
| −0.068 | 13.9 |
|
| −0.080 | 20.94 |
|
|
|
|
|
| 0.105 |
|
|
| 0.147 |
|
|
|
|
|
|
|
|
| −0.565‡ | 6.75 | 1.357 | 8.78 |
|
|
|
|
|
|
|
| 0.242 |
| 1.131 |
|
|
| 98.75% | 98.57% | 98.79% | 98.7% | 98.55% | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Maternal and Child Health · Child Nutrition and Water Access · Poverty, Education, and Child Welfare
Son preference, entrenched in many societies, significantly influences parental decisions on early childcare practices. Such cultural norms not only disadvantage girls in early childhood, but also reinforce societal structures that hinder gender equality in the long run. While a recent systematic review concluded that boys are more likely to be undernourished [1], a large body of scientific evidence highlights that, in countries and settings with a high son preference, girls have higher mortality rates [2], are less likely to be fully immunised [3], are weaned earlier [4], have lower educational attainment [5], have worse long-term economic prospects [6], and have poorer mental health as adults [7], which in turn has detrimental long-term consequences for women and their offspring [8].
Addressing gender disparities in early childcare practices is vital for breaking the cycle of intergenerational poverty and ill health and fostering gender-equitable societal development. The first 1000 days from conception is crucial for a child’s long-term physical and cognitive development; during the first days of life, a child’s brain connects millions of neurons per second at a rate never equalled later [9]. Yet, around 250 million children are expected not to reach optimal development due to inadequate nutrition and care [10]. Children who fail to reach their developmental potential due to gender-biased practices are less likely to enjoy good health, educational success, or equal employment opportunities [6,8,10], directly contradicting several of the United Nations’ Sustainable Development Goals (SDGs).
In synthesising evidence on early childcare practices, previous reviews have focused on the links between children’s sex and exclusive breastfeeding in Ethiopia [11], on gender discriminatory care-seeking practices in South Asia [12] and on the global parent-level barriers to child vaccination [13,14]. Yet, to the best of our knowledge, these reviews have only presented narrative syntheses and have not comprehensively assessed the extent of gender discrimination in early childcare practices across different geographic locations and outcomes.
To address this gap, we conduct a systematic review and meta-analysis to quantitatively synthesise the existing evidence on the role of gender in early childcare practices in low- and middle-income countries (LMICs). Drawing on the five components of nurturing care proposed by the World Health Organization (WHO), we specifically assess gender disparities in immediate parental health investments, including breastfeeding, immunisation, pre- and post-natal check-ups, and healthcare expenditure [15]. Since a comprehensive systematic review and meta-analysis on gender differences in growth and nutrition-related outcomes has already been conducted [1], we deliberately exclude long-term outcomes such as growth and nutrition from our analysis. We also applied robust variance estimation, an advanced meta-analysis technique, to provide a nuanced, solid understanding of how gender influences early childcare practices.
METHODS
Search strategy and selection criteria
We sought to identify reports and studies on any potential gender difference in early childcare practices, specifically, in breastfeeding, immunisation, pre- and post-natal check-ups, and healthcare expenditure in LMICs. We registered the protocol with PROSPERO (CRD42021286151) and reported our findings per the PRISMA guidelines [16].
We systematically searched the following databases and organisational repositories for both scientific and grey literature: PubMed, Web of Science, Cochrane Library, EconPapers, EBSCO, NBER Working papers, World Bank Open Knowledge Repository, United Nations Children’s Fund, WHO, OpenGrey, Emergency Nutrition Network, and ProQuest, from 16 November 2021 to 24 November 2021, and again from 24 January 2024 to 25 February 2024. We applied no restrictions on publication date or type; records were retrieved from the earliest available entries in each database up to the most recent search date (Table S4 in the Online Supplementary Document). We further hand-searched the three journals (BMJ Global Health, Journal of Global Health, and Lancet Global Health), conducted a structured search in Google Scholar using predefined search teams, and reviewed the references of retrieved systematic reviews and meta-analyses.
We included studies that relied on quantitative cross-sectional or longitudinal data and reported gender-segregated information for any of the following outcomes for children under five years old: any breastfeeding, breastfeeding duration, immunisation status (full immunisation or single vaccination doses), the number of pre- and post-natal check-ups, and child-focused healthcare expenditure (any direct household spending on healthcare services for the child, including visits, medications, and treatment). Eligible studies needed to be conducted in LMICs, defined according to the World Bank 2024 definition [17] (Table S3 in the Online Supplementary Document), and written in English. Following the Central Limit Theorem, we excluded studies with fewer than 30 observations to ensure stable sampling distributions and to improve the reliability of the pooled effect size estimates [18]. We also excluded qualitative research, literature reviews, and systematic reviews.
One author (MJ) ran the initial searches and later performed an updated search alongside another author (FS). The search results were imported into the Rayyan online screening tool (Rayyan, Cambridge, Massachusetts, USA). After deduplication, rotating reviewer pairs independently screened all the titles and abstracts against the eligibility criteria (Table S5 in the Online Supplementary Document). Conflicts were resolved through discussion and consensus or by contacting a third reviewer. Subsequently, one author (MJ) performed the full-text screening, contacting a co-author (JS) in case of any uncertainty.
Quality appraisal
We modified the Joanna Briggs Institute critical appraisal tool for cross-sectional studies to assess the quality of the included studies [19]. Given that our review focused on gender differences, rather than exposure-outcome relationships, we omitted exposure-related items and added others assessing whether study aims, objectives, and limitations were reported. We thus assessed the quality of the included studies using nine criteria about sampling, study setting, methods, and limitations of the study, with each criteria a value of 1 (met), 0.5 (partially met/unclear), or 0 (not met), and the total score being divided by nine to produce a standardised quality score ranging from 0 (lowest quality) to 1 (highest quality) (Table S6 in the Online Supplementary Document). We piloted the tool in 10% of studies, with the remaining studies assessed by three authors (EC, FS, CA). Any differences were discussed and resolved through consensus or by contacting another author (JS).
Data extraction
We extracted the following characteristics: author, title, publication type (journal article, working paper, preprint, or bulletin), year of publication, region, country, study design, data source, year of data collection, sample size, age, outcome (breastfeeding/breastfeeding duration, complete immunisation, number of vaccinations, immunisation status for specific vaccines, number of pre-/post-natal check-ups, and child-related healthcare expenditure), and the corresponding effect sizes (e.g. odds ratios, risk ratios, ordinary least squares coefficients, means) into a piloted data extraction form. For studies where multiple effect sizes for the same outcome were available, we kept the most statistically rigorous ones from the estimation model including the highest number of control variables.
Standardisation of effect sizes
To provide pooled estimates across all studies, we converted the study-specific estimates, where possible, to a common metric of a standardised mean difference, Cohen’s d, and its variance V_d_. For studies reporting odds ratio, we converted them to Cohen’s d values using the following formula:
For studies that reported means for boys and girls, we calculated Cohen’s d as [20]:
Here, Y_g_ and Y_b_ are mean values of the respective outcome variable, s_g_^2^ and s_b_^2^ stand for the standard deviation of these means, and n_g_ and n_b_ are sample sizes for girls and boys, respectively. For studies where we retrieved ordinary least square coefficients, we estimated the standardised mean difference as follows:
Here, sd^2^ is the standard deviation of the β coefficient.
Probit coefficients were first converted to log odds ratios using the following formula:
and then converted to Cohen’s d using equations 1) and 2).
To avoid overestimation due to small sample sizes, we applied Hedges’ small sample size correction and converted Cohen’s d to Hedges’ g using the following formula [21]:
Meta-analysis
The included studies may have had a statistical dependence due to correlated effect sizes, which arises if a single study reports multiple effect sizes or if a similar study population was used in several studies [22,23]. Since most of the studies relied on secondary data, some of them use identical datasets, such as the Demographic Health Survey and the National Family Health Survey. To adjust for dependency in included effect sizes, we applied a robust variance estimation (RVE) model, which takes into account the statistical dependence among the effect sizes, corrects the standard errors, and allows the inclusion of multiple effect sizes per study, regardless of their dependence structure [22,23]. Following the literature, we assumed correlated effect sizes and a rho of 0.8 for the observed effect sizes [24]. The estimated RVE model is defined as follows:
Here, y_ij_ is the estimated effect size i in study j for the outcome of interest (breastfeeding, immunisation, prenatal and post-natal check-ups, or healthcare expenditure), α is the pooled average of the true effect, u_j_ is a study-level random effect, var(u_j_) = τ^2^ is the between-study variance component, and e_ij_ is an error term for ith effect size in the jth study. We performed the RVE for effect sizes pooled across all outcomes and separately by each outcome of interest. We present the between-study variance and proportion of observed differences due to heterogeneity rather than the sampling error using τ^2^ and I^2^ measures, respectively.
Meta-regression
We ran meta-regressions to estimate the effect of selected study characteristics on standardised effect sizes using the following equation:
X_ij_ is a vector of moderator variables, including geographic region, year of data collection, study quality, and the Gender Inequality Index (GII) score of the respective country. We included the GII in our meta-regression to test if countries with higher gender inequality ratings also find more pronounced gender differences in health outcomes between girls and boys. We ran meta-regressions by including each moderator variable separately and then by including all moderator variables together in one final estimation model.
We cleaned the data in Stata/MP, version 17.0 (StataCorp LLC, College Station, TX, USA) and performed the analysis in R, version 4.4.0 (R Foundation for Statistical Computing, Vienna, Austria).
Publication bias
We assessed publication bias using the traditional methods of visual inspection of funnel plots and the formal Egger’s regression test, despite its sensitivity to heterogeneity and small sample sizes [25]. We also employed more recent methods, including visual inspection of DOI plots and the LFK index, for greater accuracy [26].
Patient and public involvement
Patients were not involved in design, conduct, analysis, or reporting of this work.
RESULTS
Study selection
We identified 67 576 records, of which 17 569 were duplicates, leaving 50 007 unique records for title and abstract screening (Figure 1). Following full-text screening of 298 articles, we included 78 studies in our systematic review [3,4,27–102] and 52 in the meta-analysis [3,4,28,30,32,34,37–40,43–46,48–54,57–63,65,69,71,73–75,77–79,81–86,88,90,92–94,99–102]. Twenty-six studies could not be included in the meta-analysis due to missing information on coefficients, standard deviations, or the number of observations. We contacted the corresponding authors of the studies with insufficient information, asking for additional data, and followed up with authors in case on non-response after two weeks. We dropped studies from the meta-analysis in case of non-response from the authors after the follow-up. Hazard ratios, risk reduction, risk differences, relative risk reduction, female-to-male ratios, Tobit estimates, accelerated failure time, and proportional hazard ratios were dropped from quantitative synthesis due to high heterogeneity in the nature of studies and/or due to insufficient data to calculate Cohen’s d and Hedges’ g values. Studies without sufficient data to calculate the standardised means scores were retained in the narrative synthesis. Specifically, we created a separate column in the table of included studies to summarise whether reported estimates suggested any health disadvantage for boys or for girls or reported null effects. Overall, 231 effect sizes were included in the analysis, with an average of 4.44 effect size estimates per study.
PRISMA flow diagram. Figures S1 and S2 in the Online Supplementary Document show the detailed number of studies retrieved from the original and updated searches from each of the data sources. n – number of studies.
Study characteristics
The 78 included studies covered 55 LMICs, with 54 (69%) focusing on South Asia, 11 (14%) on sub-Saharan Africa, 6 (8%) on the Middle East and North Africa, 4 (5%) on East Asia and Pacific, 2 (3%) on multiple countries and regions, and 1 (1%) on Europe and Central Asia. Forty-three (55%) studies focused on India, five (6%) on Ethiopia, and another five (6%) on Pakistan (Figure 2). Fifty-two (67%) studies focused on immunisation and 23 (30%) on breastfeeding, while only 7 (9%) assessed gender disparities in healthcare expenditure and 4 (5%) investigated pre- and post-natal check-ups. The sample size across studies ranged from 102 to over six million participants, with a total sample size of 16 936 585 across all studies included in the meta-analysis. The included studies were published between 1992 and 2024. 96% (n = 75) of included studies were journal articles, 3% (n = 2) were working papers or pre-prints, and 1% (n = 1) was a bulletin. In summary, 58% (n = 47) indicated that girls faced disadvantages, 40% (n = 32) showed no gender differences, 2% (n = 2) reported more favourable outcomes for girls (Table 1). The quality of included studies varied substantially between 22% (i.e. only 2 out of 9 criteria marked with highest quality) and 100%. This variation suggests significant differences in methodological quality, study conduct, and transparency in reporting across the included studies.
*Geographical coverage of the included studies. Estimations are based on 78 included studies identified in this review.
Meta-analysis
The majority of the 52 studies included in the meta-analysis concentrated on gender differences in immunisation (n = 32) and breastfeeding (n = 17), with only a few examining differences in pre-and post-natal check-ups (n = 4) and healthcare expenditures (n = 7). We found a negative and statistically significant overall effect of −0.082 (95% confidence interval (CI) = −0.133, −0.03; P = 0.002), indicating an overall health(care) disadvantage for girls (Figure 3). The I^2^ for the pooled estimates was high (98.75%), demonstrating high heterogeneity across studies that was not solely due to sampling error **(**Table S7 in the Online Supplementary Document). The analysis by outcome type showed more pronounced gender disparities for breastfeeding (Hedges’ g = −0.05; 95% CI = −0.089, −0.012; P = 0.013) and immunisation practices (Hedges’ g = −0.073; 95% CI = −0.13, −0.016; P = 0.015), with lower rates for girls compared to boys. Although the effect of pre- and post-natal check-ups was negative and significant (Hedges’ g = −0.029; 95% CI = −0.058, −0.000; P = 0.048), the associated degrees of freedom were 2.8 (Figure 3; Table S8 in the Online Supplementary Document). Results with less than four degrees of freedom should not be trusted as reliable [23], which is why we should interpret this finding with caution. Overall, since all pooled Hedges’ g values fell below 0.20, the observed gender differences represent small effect sizes. Nonetheless, these small effects translate into consistent disadvantages for girls, corresponding to approximately 9% lower breastfeeding, 12% lower immunisation, and 5.1% fewer pre- and post-natal check-ups compared to boys. We found no significant effect for health expenditure patterns when comparing boys and girls (Hedges’ g = −0.278; 95% CI = −0.641, 0.083; P = 0.109). These insignificant estimates may have stemmed from an absence of clear gender differences in healthcare spending or could have been related to the limited number of studies (n = 7) and effect sizes (n = 8) available for this outcome category. The I^2^ was over 70% across all sub-group specifications (Table S8 in the Online Supplementary Document). This high heterogeneity may have resulted from differences in outcome categories and from including different effect size measures. Note that I^2^ approaching 100% could have also been driven by a few studies where standard errors tend to approach zero due to large sample sizes [103].
Forest plot of pooled effect sizes on the effect of gender on pooled health care outcomes and by each outcome type separately with 95% CI. Full results and forest plots of individual studies by outcome types are presented in Figures S3–6 and Tables S7–10 in the Online Supplementary Document. CI – confidence interval, N – number of studies, n – number of effect sizes in each group.
Given that most of the studies in this review focused on India, we additionally ran a sensitivity analysis excluding studies with data from India (Table S10 in the Online Supplementary Document). The estimates for gender disparities across all outcomes were still negative, but no longer significant due to a loss of 31 studies and 160 effect sizes. Still, the consistently negative pattern of our results provided suggestive evidence that the observed negative pooled effect in the full sample of studies is not exclusively driven by the gender discrimination present in India.
Meta-regression
We performed meta-regressions to explore the potential sources of the high heterogeneity (Table 2). Effect sizes did not vary significantly between geographical regions. However, there were less than four degrees of freedom, and the results must, therefore, be treated cautiously. The year of data collection was significantly and positively correlated with effect sizes, suggesting a narrowing gender gap over time. The study quality did not determine the direction and magnitude of effect sizes. We also ran the analysis using a dichotomous variable for study quality, dividing study into below and above median quality; the analysis yielded similarly insignificant results. As hypothesised, the GII exhibited a moderately significant negative correlation with effect sizes, indicating that higher levels of gender inequality in a country are associated with larger health-related penalties for girls. We did not find any significant effects in the full meta-regression that included all moderator variables simultaneously, except for the year of data collection, which indicated a decline in the gender gap over time. The I^2^ exceeded 98% in all specifications, implying that the high heterogeneity between included studies must have largely stemmed from factors not included in the meta-regression.
Publication bias
A visual inspection of the funnel plot suggested no asymmetry, corroborated by a P-value of 0.22 for the Egger’s regression test (Figure S7 in the Online Supplementary Document). In the absence of publication bias, the LFK value should lie between −1 and 1 [24]. Here, the estimated LFK value based on the DOI plot was −0.86 (Figure S8 in the Online Supplementary Document); hence, we conclude that our results were unlikely to be affected by publication bias.
DISCUSSION
This systematic review explored gender differences in early childcare practices within LMICs. We identified 78 eligible studies covering 55 LMICs, of which 52 were included in the meta-analysis. We found evidence for significant gender discrimination against girls in parental health investments, including breastfeeding, immunisation, and pre- and post-natal check-ups. Our findings are alarming, given that adequate early childcare practices, as well as timely access to healthcare, are crucial determinants for child health and survival. Namely, breastfeeding is associated with a lower likelihood of contracting infectious diseases, higher intellectual abilities, and reduced risk of diabetes and being overweight [105]. Similarly, vaccinations in early life are estimated to prevent up to five million deaths annually [106]. A significant share of 2.6 million stillbirths and 2.7 million neonatal deaths could be averted with adequate and timely access to healthcare [107].
Very few reviews have focused on gender as a determinant of early childcare practices, with mixed conclusions. As opposed to our findings, qualitative evidence on child immunisation rarely identifies gender as a significant factor. For instance, a review of 25 qualitative studies reported that only one identified son preference as a parental barrier to child vaccination [14], while another review documented that only two out of 30 papers considered gender norms as a potential barrier [13]. In contrast, a review of quantitative studies on this topic, although limited in scope and focused primarily on India, pointed to a substantially higher vaccination coverage for boys than girls [108], in line with the pronounced gender differences in immunisation we observed here. Given that vaccinations are often provided free of charge in many countries, these gender-related disparities are likely driven by cultural norms and societal expectations around gender roles. Our findings also broaden the scope of existing reviews on the prevalence of pro-boy breastfeeding practices. For example, a review of studies conducted in Ethiopia found that newborn boys were 30% more likely to be exclusively breastfed than newborn girls in the first six months of their life [11]. A suggested underlying mechanism in the literature is fertility behaviour based on son preference, where mothers may use longer breastfeeding as a contraception method during boys’ infancy while shortening breastfeeding duration for infant girls to continue child-bearing in pursuit of having a boy [4].
Similarly, a previous systematic review on gender bias in healthcare access and utilisation documented wide gender disparities in favour of boys in hospital in-patient and out-patient attendance, duration from admission to death, and healthcare seeking behaviour, with the majority of studies conducted in Asia [109]. There is currently no systematic evidence on healthcare expenditure differences between boys and girls to compare our results to. Yet, a closer examination of included studies shows that healthcare expenditure patterns for boys and girls were not significantly different in China, Nepal, and Pakistan, and were slightly in favour of boys in India.
Gender-based differences also manifest in other dimensions of child development, extending beyond the outcomes addressed in this research. For example, despite a substantial progress towards achieving gender equality in education, girls (and women) still remain less educated than boys (and men) in many countries [110]. However, when focusing on nutritional status, a recent systematic review and meta-analysis found that boys are 14–29% more likely to be undernourished [1]. While this pattern is found more consistent across African countries, authors show that it diverges in other regions including East Africa, Central America, South and Southeast Asia, where the differences between boys and girls in undernutrition were either marginal or in favour of boys. These findings further highlight a gap in research explicitly examining the role of gender in healthcare investments and access.
This study has a few limitations that should be considered when interpreting its findings. First, as individual studies on pre- and post-natal care and healthcare expenditure are generally scarce, we are not able to include a larger number of related studies in this review, suggesting a cautious interpretation of observed gender differences in these dimensions. This limitation nevertheless underscores potential research avenues to explore gendered patterns in pre- and post-natal childcare as well as intra-household resource allocation among children. Second, a substantial share of the studies included in this review focused on India, which may limit the generalisability of our pooled findings to other contexts. This focus likely stems from the scientific interest in gender-related research in India, and more generally in South East Asia – especially following Amartya Sen’s seminal work on ‘missing women’ [111]. This region has long reported significant gender gaps in child development and mortality [2,3,112]. Nonetheless, other regions, such as East and Central Asia, which also exhibit strong son preference [113] but remain relatively understudied, need greater research efforts to uncover the patterns of gender inequalities and underlying contextual mechanisms. Third, a single reviewer conducted the full-text screening, which may have introduced a risk of selection bias or errors. However, this was mitigated by duplicate screening at earlier stages and by consulting JS in cases of uncertainty during full-text screening. Lastly, our language restriction is another shortcoming, as it may have excluded important studies written in languages other than English.
Despite these limitations, our systematic review and meta-analysis fill a critical gap in understanding the role of gender in early childcare practices, particularly in regions with a high prevalence of son preference. An important contribution of this study is its extensive scope, making it, to the best of our knowledge, the largest analysis of its kind. Additionally, we apply a rigorous quantitative approach to harmonise results based on diverse methodologies to systematically aggregate existing evidence. Another key strength of our review is the focus on child health ‘inputs’, as immediate parental investments in breastfeeding, child immunisation, and the use of healthcare services, rather than ‘outputs’, such as measures based on anthropometrics or mortality. This focus particularly underscores the urgency of continued efforts to understand the root causes of gender discrimination in early childcare practices, which ultimately contributes to closing gender gaps in adult life outcomes, and hence, more gender-equitable and prosperous societies. Policymakers should prioritise interventions that ensure equitable access to breastfeeding support, immunisation programs, and healthcare services for all children, regardless of gender.
CONCLUSIONS
This systematic review and meta-analysis provide robust evidence that gender discrimination in early childcare practices remains a significant challenge in many LMICs. Across breastfeeding, immunisation, and pre- and post-natal healthcare, girls consistently receive fewer health investments than boys, despite the profound implications for child survival and long-term development. While the evidence base remains uneven across regions and topics, our findings underscore the urgent need for greater research attention in regions where strong son preference persists but empirical evidence is limited. Strengthening gender-sensitive health policies and ensuring equitable access to essential early-life services should be central priorities for governments and global health practitioners.
Additional material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thurstans S Opondo C Seal A Wells JC Khara T Dolan C Boys are more likely to be undernourished than girls: a systematic review and meta-analysis of sex differences in undernutrition. BMJ Glob Health. 2020;5:e 004030. 10.1136/bmjgh-2020-00403033328202 PMC 7745319 · doi ↗ · pubmed ↗
- 2Bongaarts J Guilmoto C How many more missing women? Lancet. 2015;386:427. 10.1016/S 0140-6736(15)61439-826251384 · doi ↗ · pubmed ↗
- 3Pande RP Selective gender differences in childhood nutrition and immunization in rural India: the role of siblings. Demography. 2003;40:395–418. 10.1353/dem.2003.002912962055 · doi ↗ · pubmed ↗
- 4Jayachandran S Kuziemko I Why do mothers breastfeed girls less than boys? Evidence and implications for child health in India. Q J Econ. 2011;126:1485–538. 10.1093/qje/qjr 02922148132 · doi ↗ · pubmed ↗
- 5Wang W Fan CC Li J Son preference, eldest son preference, and educational attainment: Evidence from Chinese families. J Fam Issues. 2020;41:636–66. 10.1177/0192513 X 19874091 · doi ↗
- 6Hoddinott J Alderman H Behrman JR Haddad L Horton S Adult consequences of growth failure in early childhood. Am J Clin Nutr. 2013;98:1170–8. 10.3945/ajcn.113.06458424004889 PMC 3798075 · doi ↗ · pubmed ↗
- 7Wang Q Rizzo JA Fang H Parents’ son preference, childhood adverse experience and mental health in old age: Evidence from China. Child Abuse Negl. 2019;93:249–62. 10.1016/j.chiabu.2019.05.01231129427 · doi ↗ · pubmed ↗
- 8Victora CG Adair L Fall C Hallal PC Martorell R Richter L Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371:340–57. 10.1016/S 0140-6736(07)61692-418206223 PMC 2258311 · doi ↗ · pubmed ↗