The Reversed Halo Sign: A Rare Presentation of Legionella Pneumonia
Alexandre Dias Mançano, Gláucia Zanetti, Edson Marchiori

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
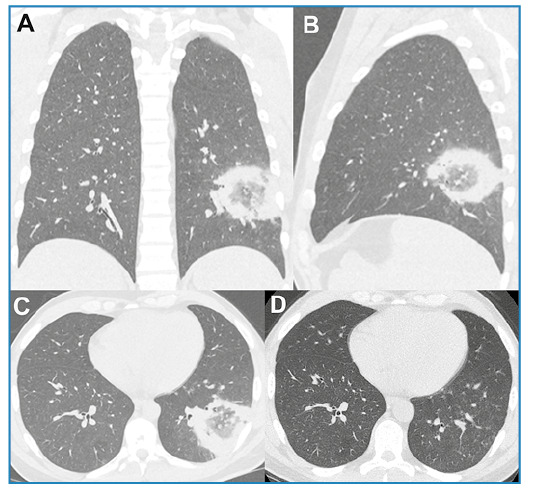 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLegionella and Acanthamoeba research · Pneumothorax, Barotrauma, Emphysema · Pleural and Pulmonary Diseases
A 28-year-old man presented with a 2-day history of fever (39ºC), myalgia, and dry cough, followed by general condition decline and onset of chills, left-sided pleuritic pain, and episodes of diarrhea. Physical examination revealed crackles in the lower third of the left lung. The patient’s oxygen saturation in ambient air was 97%.
Laboratory tests revealed leukocytosis, elevated C-reactive protein level (26.3 mg/L), and hyponatremia (128 mmol/L; reference range, 135-145 mmol/L). Human immunodeficiency virus (HIV) testing and blood cultures were negative. Chest computed tomography (CT) revealed a reversed halo sign (RHS) in the left lower lobe (Figure 1A-C). A polymerase chain reaction panel for respiratory infections tested positive for Legionella pneumophila.
FIGURE 1:Chest computed tomography (CT) images with coronal (A), sagittal (B), and axial (C) reconstruction showing a rounded area of ground-glass opacity surrounded by a complete ring of consolidation in the left lower lobe, compatible with the reversed halo sign. Control CT performed three weeks after the initial examination (D) revealed complete lesion regression.
The urinary antigen test result for Legionella was also positive. Bronchoalveolar lavage cultures confirmed the presence of L. pneumophila. The final diagnosis of L. pneumophila pneumonia was established. Azithromycin (500 mg for 14 days) was prescribed and yielded an excellent clinical response. Three weeks after the initial examination, a control CT revealed complete regression of the lesion (Figure 1D).
L. pneumophila is an aerobic gram-negative bacillus. The most common CT findings are consolidation and/or ground-glass opacities. Pleural effusion was frequently observed. Cavitation and lymphadenopathy are common in immunocompromised patients1 ^-^ 3. RHS is a focal, rounded area of ground-glass opacity surrounded by a complete or nearly complete ring of consolidation on chest CT. It was initially considered specific to cryptogenic organizing pneumonia, but has since been reported to be associated with diverse clinical entities, including infectious and noninfectious diseases4 ^,^ 5.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Yu H Higa F Hibiya K Furugen M Sato Y Shinzato T Computed tomographic features of 23 sporadic cases with Legionella pneumophila pneumonia Eur J Radiol 2010743 e 73-810.1016/j.ejrad.2009.04.01119423258 · doi ↗ · pubmed ↗
- 2Bai L Yang W Li Y Clinical and Laboratory Diagnosis of Legionella Pneumonia Diagnostics Basel 202313228028010.3390/diagnostics 1302028036673091 PMC 9858276 · doi ↗ · pubmed ↗
- 3Shroff GS Marom EM Wu CC Godoy MCB Wei W Ihegword A Pulmonary Legionellosis in Oncologic Patients: Findings on Chest CTJ Comput Assist Tomogr 201640691792210.1097/RCT.000000000000046127454787 · doi ↗ · pubmed ↗
- 4Marchiori E Zanetti G Escuissato DL Souza AS Jr. Meirelles GD Fagundes J Reversed halo sign: high-resolution CT scan findings in 79 patients Chest 20121411260126610.1378/chest.11-105022016487 · doi ↗ · pubmed ↗
- 5Godoy MC Viswanathan C Marchiori E Truong MT Benveniste MF Rossi S The reversed halo sign: update and differential diagnosis Brit J Radiol 2012851226123510.1259/bjr/5453231622553298 PMC 3487053 · doi ↗ · pubmed ↗