Taste Dysfunction in Oral Candidiasis: Impact of Candida Carriage and Hyphal Presence
Younjung Park, Hyo‐Jung Jung, Sin Hye Hwang, Eunae Sandra Cho, Hyung‐Joon Ahn

TL;DR
This study shows that carrying Candida albicans, especially in its hyphal form, is linked to reduced taste sensitivity, and antifungal treatment improves taste function.
Contribution
The study identifies a link between hyphal forms of Candida albicans and taste dysfunction, suggesting a causal role in oral candidiasis.
Findings
Candida carriers showed reduced sensitivity to sweet, bitter, and umami tastes compared to noncarriers.
Hyphal presence in Candida carriers was associated with greater taste impairment.
Topical fluconazole treatment reduced hyphae and improved taste sensitivity.
Abstract
Taste dysfunction is a common symptom of oral candidiasis; however, its underlying mechanisms remain unclear. This study aimed to determine whether Candida albicans carriage, particularly its hyphal phenotype, is associated with impaired taste sensitivity. Fifty‐seven participants were divided into three groups: noncarriers (n = 20), carriers without hyphae (n = 20), and carriers with hyphae (n = 17). Tongue biofilm samples were collected for Candida culture and smear tests. Salivary flow rates were measured, and taste sensitivity was assessed using standardised taste strips. Carriers underwent topical fluconazole treatment, and post‐treatment taste sensitivity was re‐evaluated. Carriers exhibited reduced sensitivity to sweet and bitter tastes, with an additional decline in umami sensitivity among those with hyphae. In addition, both unstimulated and stimulated salivary flow rates…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
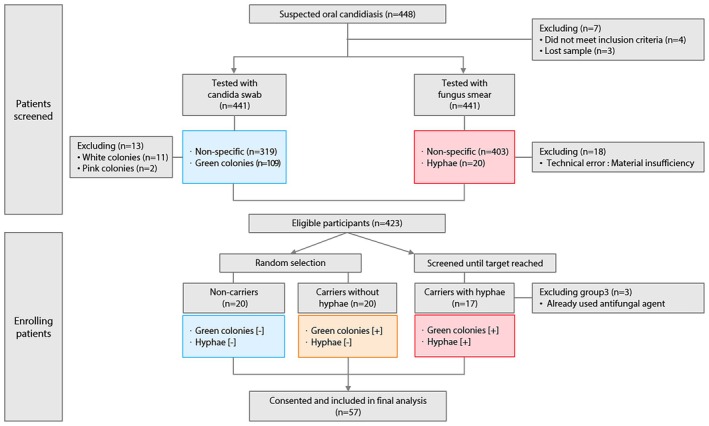 FIGURE 1
FIGURE 1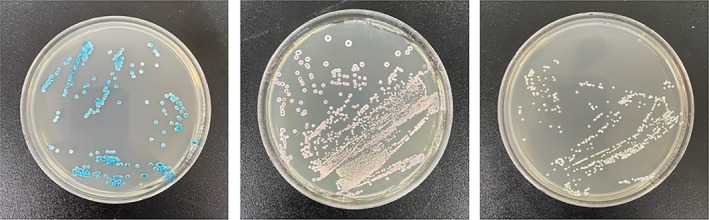 FIGURE 2
FIGURE 2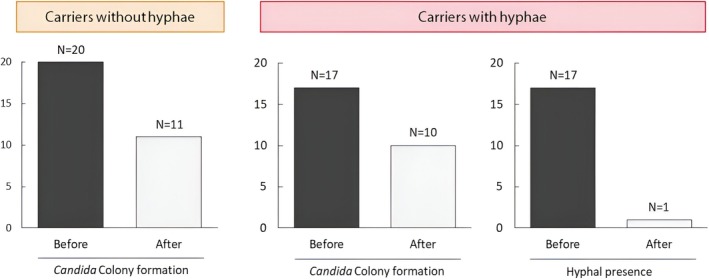 FIGURE 3
FIGURE 3| Taste modality | Concentration level | |||
|---|---|---|---|---|
| Sweet (sucrose, g/mL) | 0.05 | 0.1 | 0.2 | 0.4 |
| Bitter (quinine‐hydrochloride, g/mL) | 0.0004 | 0.0009 | 0.0024 | 0.006 |
| Salty (sodium chloride, g/mL) | 0.016 | 0.04 | 0.1 | 0.25 |
| Sour (citric acid, g/mL) | 0.05 | 0.09 | 0.165 | 0.3 |
| Umami (monosodium glutamate, g/mL) | 0.016 | 0.04 | 0.1 | 0.25 |
| Variable | Non‐carrier ( | Carriers without hyphae ( | Carriers with hyphae ( |
|
|---|---|---|---|---|
| Age (years) | 46.7 ± 11.7 | 48.9 ± 9.7 | 54.2 ± 8.6 | 0.080 |
| Sex | ||||
| Male | 2 (10.0) | 5 (25.0) | 2 (11.8) | 0.370 |
| Female | 18 (90.0) | 15 (75.0) | 15 (88.2) | |
| Spontaneous pain | ||||
| Yes | 14 (70.0) | 8 (40.0) | 8 (47.1) | 0.141 |
| No | 6 (30.0) | 12 (60.0) | 9 (52.9) | |
| Stimulated pain | ||||
| Yes | 14 (70.0) | 12 (60.0) | 13 (76.5) | 0.552 |
| No | 6 (30.0) | 8 (40.0) | 4 (23.5) | |
| Subjective dry mouth | ||||
| Yes | 9 (45.0) | 13 (65.0) | 13 (76.5) | 0.135 |
| No | 11 (55.0) | 7 (35.0) | 4 (23.5) | |
| UWS flow rate | 0.31 ± 0.17 | 0.21 ± 0.11 | 0.21 ± 0.16 | 0.045 |
| SWS flow rate | 1.32 ± 0.79a | 0.82 ± 0.33b | 0.81 ± 0.48b | 0.011 |
| Tongue moisture | 27.4 ± 3.4a | 25.2 ± 2.1b | 23.9 ± 2.8b | 0.001 |
| Variable | Non‐carrier ( | Carriers without hyphae ( | Carriers with hyphae ( |
|
|---|---|---|---|---|
| Sweet | 3.50 ± 0.69a | 2.80 ± 1.06b | 2.71 ± 0.92b | 0.016 |
| Sour | 2.25 ± 0.64 | 1.90 ± 0.64 | 1.82 ± 0.95 | 0.178 |
| Salty | 2.55 ± 1.19 | 2.10 ± 1.07 | 1.94 ± 1.09 | 0.230 |
| Bitter | 3.65 ± 0.67a | 2.00 ± 1.49b | 2.00 ± 1.62b | < 0.001 |
| Umami | 2.50 ± 1.05a | 2.10 ± 1.45a | 1.41 ± 1.06b | 0.029 |
| Total score | 14.55 ± 2.12a | 10.85 ± 3.94b | 9.82 ± 3.34b | < 0.001 |
| Carriers without hyphae ( | Carriers with hyphae ( |
| |||
|---|---|---|---|---|---|
| Mean ± SD |
| Mean ± SD |
| ||
| Sweet | 0.45 ± 1.15 | 0.095 | 0.47 ± 0.51 | 0.002 | 0.946 |
| Sour | 0.15 ± 0.59 | 0.267 | 0.29 ± 0.69 | 0.096 | 0.495 |
| Salty | −0.10 ± 0.72 | 0.541 | 0.47 ± 0.62 | 0.007 | 0.015 |
| Bitter | 0.55 ± 0.89 | 0.012 | 0.53 ± 0.72 | 0.008 | 0.939 |
| Umami | 0.05 ± 0.69 | 0.748 | 0.59 ± 0.80 | 0.008 | 0.034 |
| Total score | 1.15 ± 2.50 | 0.053 | 2.35 ± 1.66 | < 0.001 | 0.099 |
- —the National Research Foundation of Korea10.13039/501100003725
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSalivary Gland Disorders and Functions · Biochemical Analysis and Sensing Techniques · Oral microbiology and periodontitis research
Introduction
1
Candida is a dimorphic fungus that exists in the oral cavity either as a commensal yeast or in an invasive hyphal form [1, 2]. The hyphal phenotype is associated with increased virulence, epithelial infiltration, tissue damage, and biofilm formation [3, 4, 5]. Oral candidiasis (OC) assessments have conventionally focused on overall Candida carriage or cultured specimens under controlled conditions [6, 7, 8, 9]. However, recent evidence suggests that biofilm formation plays a critical role in the pathogenesis of OC by creating a persistent, drug‐resistant microbial ecosystem composed of Candida, extracellular matrix, and occasionally bacteria [10, 11, 12, 13, 14].
OC is typically classified based on its clinical manifestations, such as pseudomembranous and erythematous candidiasis; however, it often presents with less obvious symptoms, including taste dysfunction [15, 16]. Despite being a hallmark symptom, the precise mechanisms underlying taste impairment in OC remain poorly understood [17, 18]. As the tongue serves as the primary reservoir for Candida colonisation, and saliva is essential for transporting taste stimuli, disturbances in these factors may contribute to altered gustatory function [17, 19].
In this study, we investigated the association between Candida albicans ( C. albicans ) carriage, with an emphasis on its hyphal phenotype, and taste dysfunction and concomitant changes in salivary flow. By employing both Candida carriage and smear tests to assess tongue biofilms, we aimed to elucidate the clinical relevance of Candida biofilms and hyphal transitions in the development of taste impairment in patients with OC.
Patients and Methods
2
Sample Size Calculation
2.1
The sample size required for this study was determined using GPower 3.1.9.7. A one‐way ANOVA was used as the primary analysis to detect differences among the three groups in taste threshold and related variables. The expected effect size (f = 0.471) was derived from the mean taste threshold values reported by Sakashita et al. [18]. With an effect size of 0.471, a significance level (α) of 0.05, and a statistical power of 85%, the minimum required sample size was calculated to be 54 participants. Considering an anticipated dropout rate of 10%, the final target sample size was set at 60 participants (20 per group).
Participants and Study Design
2.2
This prospective clinical study was conducted at Yonsei University Dental Hospital from February 2021 to September 2022, enrolling patients who visited the Department of Orofacial Pain and Oral Medicine with suspected oral candidiasis.
The inclusion criteria were: (1) age between 20 and 65 years; (2) clinical suspicion of oral candidiasis; (3) completion of both candida swab and fungus smear tests; and (4) voluntary written informed consent. The exclusion criteria were: (1) uncontrolled systemic diseases (e.g., diabetes mellitus, gastroesophageal reflux disease, chronic hepatic or renal disease, hypothyroidism); (2) current use of antipsychotic medications; (3) history of Sjögren's syndrome; (4) prior head and neck radiotherapy; (5) significant oral lesions (widespread dental caries, severe periodontal disease with probing depth ≥ 6 mm, stomatitis, or mucosal diseases such as lichen planus); and (6) other reasons deemed inappropriate for participation by the principal investigator.
Eligible participants were classified into three groups according to candida swab and fungus smear test results. For Group 1 (non‐carriers) and Group 2 (carriers without hyphae), random selection among eligible subjects was performed to achieve a target sample size of 20 per group, and additional recruitment ceased once enrollment targets were met. For Group 3 (carriers with hyphae), detection was rare, so recruitment continued until the target was reached among all screened patients. After excluding three subjects in Group 3 who had previously received antifungal agents, a total of 57 participants were included in the final analysis.
The three study groups were defined as follows:
Non‐carriers: negative for both C. albicans colonies on swab and hyphal forms on smear (n = 20).
Carriers: positive for C. albicans colonies on swab but negative for hyphal forms on smear (n = 20).
Carriers with hyphae: positive for both C. albicans colonies on swab and hyphal forms on smear (n = 17).
A detailed flow of participant inclusion, exclusion, and classification is depicted in Figure 1.
Flow diagram of participant enrollment and group allocation. The study screened 448 adult patients with suspected oral candidiasis. After candida swab and fungus smear testing, exclusions were made as indicated. Eligible participants were classified into three groups according to test results: Non‐carriers (green colonies [−], hyphae [−]), carriers without hyphae (green colonies [+], hyphae [−]), and carriers with hyphae (green colonies [+], hyphae [+]). Random selection was performed for non‐carriers and carriers without hyphae; recruitment for carriers with hyphae continued until the target was reached. Three subjects in the carriers with hyphae group were excluded due to prior antifungal agent use. Ultimately, 57 patients consented and were included in the final analysis.
Candida Swab Test
2.3
To detect C. albicans , the biofilm on the participant's tongue dorsum was sampled three times with a sterile cotton swab. The collected sample was then transferred to a liquid transport medium prepared with Difco YM Broth 271,120 (BD DIFCO, USA) according to the manufacturer's instructions and incubated at 37°C for 24 h. Subsequently, 50 μL of the cultured suspension was inoculated onto CHROMagar Candida plates (Paris, France) and incubated at 37°C for 48 h. Soft, convex, green colonies were identified as C. albicans (Figure 2). Participants were classified as non‐carriers if no green colonies formed and as carriers if green colonies were present [20, 21].
Representative CHROMagar Candida culture plates. Photographs illustrating the results of CHROMagar Candida after 48 h of incubation at 37°C. Green colonies indicate the presence of Candida albicans (left plate), pink colonies indicate Candida krusei (middle plate), and white colonies (right plate) lack specific identification and were excluded from analysis.
Fungus Smear Test
2.4
Participants who tested positive for C. albicans in the swab test underwent a fungus smear test for pathological evaluation. A sample was collected from the biofilm on the dorsal surface of the tongue using a wooden tongue depressor and transferred onto a glass slide. It was then fixed with ethyl alcohol and stained using the periodic acid–Schiff (PAS) method. Slides were examined under a light microscope to detect Candida hyphae [22]. According to the pathology reading recorded in the electronic medical record (EMR), participants were classified into carriers without hyphae or carriers with hyphae based on the presence or absence of hyphal forms.
Taste Strip Test
2.5
Taste sensitivity was assessed using validated taste strips (Burghart, Wedel, Germany) that are widely used in clinical settings. Each set contained five taste qualities (sweet, bitter, salty, sour, and umami), each present at four different concentrations (Table 1), along with two blank (tasteless) strips, yielding a total of 22 test strips. The test was performed according to the manufacturer's instructions. One point was awarded for each correct taste identification, with a maximum score of 20 [23].
Participant Questionnaire
2.6
A structured questionnaire was used to assess patients' subjective oral symptoms, especially tongue symptoms such as spontaneous pain, stimulated pain, and oral dryness; responses for each item were recorded as “yes” or “no”.
Saliva Flow Rate
2.7
To exclude participants with xerostomia that could affect taste function, salivary flow rates were assessed at baseline in all subjects. Unstimulated whole saliva (UWS) flow rate was measured by instructing the participant to sit comfortably and tilt their head slightly forward, allowing saliva to naturally pool in the mouth without swallowing. Over a 5‐min period, all spontaneously secreted saliva was expectorated into a pre‐weighed sterile container. The total volume was recorded, and flow rate was expressed in mL/min. Stimulated whole saliva (SWS) flow rate was measured immediately after UWS collection. Participants were asked to chew a standardised, colourless, and odourless gum base at a rate of one chew per second for 5 min, expectorating all saliva into a separate pre‐weighed sterile container. SWS flow rate was calculated in the same way as UWS.
Tongue Moisture
2.8
Tongue moisture was assessed using a mucus device (Saitama, Japan). The sensor was placed at the centre of the tongue, approximately 10 mm from the tip, and three readings were recorded. The median of these readings was recorded as the final moisture level.
Antifungal Treatment
2.9
In both the “carriers without hyphae” and “carriers with hyphae” groups, where C. albicans was detected, a topical fluconazole oral suspension was prescribed for 2 weeks. The concentration (0.2%), frequency (once daily), and amount (5 mL) of the fluconazole application were specified, ensuring the treatment regimen was clearly described and standardised for all participants. All previously administered tests were repeated during the second visit to assess treatment efficacy.
Statistical Analysis
2.10
One‐way analysis of variance (ANOVA) and chi‐square tests were used to compare participant characteristics among the groups. Differences in taste sensitivity were analysed using ANOVA followed by Tukey's post hoc test. Changes in participant characteristics following antifungal treatment were summarised using descriptive statistics. Paired t‐tests were used to assess within‐group changes in taste sensitivity following antifungal treatment, and independent t‐tests were used for between‐group comparisons. All analyses were performed using SPSS version 25.0 (IBM Corp., Armonk, NY), with statistical significance set at p < 0.05.
Results
3
Participant Characteristics
3.1
A total of 57 participants were included in the study: (1) non‐carriers of C. albicans (n = 20), (2) carriers without hyphae (n = 20), and (3) carriers with hyphae (n = 17). Although the mean age was higher in the group with hyphae, the difference was not significant. The clinical tongue symptoms (spontaneous pain, stimulated pain, and subjective dry mouth) were evenly distributed among the groups. The unstimulated and stimulated salivary flow rates and tongue moisture measurements were significantly lower in the carrier groups than in the non‐carrier group (Table 2).
Taste Sensitivity
3.2
Significant differences in taste sensitivity were observed among the groups for sweet (p = 0.016), bitter (p < 0.001), and umami (p = 0.029) tastes. Compared with the non‐carrier group, the carrier groups showed reduced sensitivity to sweet and bitter tastes. Notably, sensitivity to umami taste significantly decreased only in the carrier group with hyphae. Overall, the carrier groups had lower taste sensitivity scores, indicating a general decrease in taste sensitivity (Table 3).
Therapeutic Effect of Antifungal Treatment
3.3
Following topical fluconazole administration, changes in colony formation and hyphal presence were assessed. Treatment with antifungal agent resulted in a marked reduction in hyphae (93.8%) among carriers with hyphae, whereas the decrease in colony formation was modest (45.0% in carriers without hyphae and 37.5% in carriers with hyphae; Figure 3).
Changes in Candida colony formation and hyphal presence before and after antifungal treatment. Bar graphs depicting the proportions of participants with detectable Candida colonies and hyphal forms in tongue biofilms before and after 2 weeks of topical fluconazole treatment resulted in a substantial reduction in hyphal presence, particularly in carriers with hyphae, whereas decreases in overall colony formation were more modest.
Changes in Taste Sensitivity Before and After Antifungal Treatment
3.4
Following topical fluconazole administration, changes in taste sensitivity were observed in both carrier groups. Carriers without hyphae showed a significant improvement only in their sensitivity to bitter tastes (p = 0.012). In contrast, carriers with hyphae displayed significant improvements in sweet (p = 0.002), salty (p = 0.007), bitter (p = 0.008), and umami (p = 0.008) tastes, except sour. Notably, changes in sensitivity for salty (p = 0.015) and umami (p = 0.034) tastes were significantly greater in carriers with hyphae than in those without hyphae (Table 4).
Discussion
4
Taste dysfunction is a hallmark symptom of OC; however, its precise pathogenesis remains elusive. We hypothesized that either the presence of C. albicans or, more specifically, its hyphal phenotype may contribute to impaired taste sensitivity, a notion that is significant given the opportunistic nature of Candida infection and its diverse clinical phenotypes [9, 16]. Biofilm formation, which involves the transition from yeast to hyphal forms, is a key factor contributing to Candida pathogenicity and variability in OC presentation [24, 25, 26].
Previous studies have investigated the relationship between C. albicans and taste disorders by comparing taste sensitivity among non‐carriers, healthy carriers, and patients with tongue candidiasis. These studies demonstrate that C. albicans carriage, even without clinical candidiasis, is associated with altered taste perception. Additionally, antifungal treatment has been shown to improve gustatory function in both symptomatic and asymptomatic carriers, suggesting a direct link between C. albicans and taste dysfunction [18]. However, the underlying mechanisms, particularly the roles of biofilm formation and hyphal transition, remain unclear.
Our study analysed both Candida carriage and smear tests to assess tongue biofilms, allowing a more precise evaluation of C. albicans colonisation. By stratifying participants into non‐carriers, carriers without hyphae, and carriers with hyphae, we aimed to determine the distinct role of hyphal transition in taste dysfunction. Our findings provide new insights into the clinical impact of biofilm‐associated hyphal forms, as biofilms are known to compromise epithelial integrity and interfere with taste stimulus transmission [5, 8, 27]. Notably, hyphal forms were consistently present whenever a colony was detected in culture, reinforcing their association with active disease progression and mucosal invasion.
Our results demonstrated that both unstimulated and stimulated salivary flow rates were significantly lower in Candida carriers than in non‐carriers, with particularly robust differences observed for stimulated saliva, as confirmed by post hoc analyses. This finding aligns with previous evidence that hyposalivation is a well‐known risk factor for OC, with Candida carriage frequently observed in individuals with xerostomia [28, 29, 30]. Because saliva contains antifungal proteins, antibodies, and other innate immune components that inhibit Candida adhesion and colonisation [28, 29], reduced salivary flow may predispose individuals to persistent biofilm formation. However, the distinct roles of unstimulated and stimulated saliva in biofilm formation remain unclear. Variations in the molecular composition between unstimulated and stimulated saliva highlight the potential for differing roles in Candida colonisation and biofilm dynamics [31]. This observation underscores the need for further research.
Taste sensitivity assessments revealed that carriers exhibited reduced sensitivity to sweet and bitter tastes, with an additional significant decline in sensitivity to umami taste in carriers with hyphae. These findings suggest that C. albicans colonisation may impair taste function even in the absence of overt infection, while the presence of hyphal forms may contribute to more severe dysfunction via multiple mechanisms. A possible explanation for this phenomenon is interference with taste signal transmission caused by the development of biofilms by Candida. These structured communities of yeast and hyphal cells form a physical and biochemical barrier that impedes effective contact between taste stimuli and receptors on the lingual epithelium [17]. This obstruction may be particularly relevant for umami perception, which relies on the detection of amino acids and nucleotides and requires effective interactions with the receptor sites.
Beyond physical obstruction, biofilm‐associated hyphal forms mediate taste dysfunction through enhanced epithelial disruption, immune activation, and interference with molecular signalling. Hyphae are known to penetrate mucosal layers, forming intercellular gaps and facilitating deeper invasion into host tissues [5, 32]. This process triggers inflammatory responses characterised by the upregulation of proinflammatory cytokines such as interleukin (IL)‐1β, IL‐6, and IL‐17, which influence taste bud cell turnover and may disrupt peripheral neural signalling [33, 34, 35]. Virulence factors, including candidalysin and Als3, play a central role by activating mitogen‐activated protein kinase (MAPK) pathways particularly p38 and EGFR‐ERK through interaction with epithelial receptors such as epidermal growth factor receptor (EGFR) and ephrin type‐A receptor 2 (EphA2), amplifying mucosal injury and inflammatory signalling [36, 37]. Pattern‐recognition receptors, such as TLR2, TLR4, and Dectin‐1/2, expressed on gustatory and epithelial cells, recognise Candida antigens and contribute to innate immune activation [34]. These pathways may modulate taste perception by altering ion channel activity (e.g., ENaC), promoting apoptosis of taste bud cells, and impairing neural signal transduction [35]. Additionally, inflammation‐induced changes in the tongue's microenvironment including shifts in local pH, salivary protein composition, and immune effector activity may further compromise epithelial integrity and receptor sensitivity, compounding the effects of biofilm formation and hyphal invasion on gustatory function [38, 39]. While our study design could not isolate the individual contributions of these factors, future mechanistic studies should delineate the specific roles of pH alteration, virulence factor signalling, and physical obstruction in hyphae‐associated dysgeusia.
Following topical fluconazole treatment, taste sensitivity significantly improved, particularly in carriers with hyphae. This clinical recovery underscores the pathogenic relevance of hyphal forms and supports their role as therapeutic targets in OC‐associated dysgeusia. The marked improvement following antifungal therapy targeting biofilm‐associated hyphal forms reinforces their role in driving taste dysfunction and aligns with prior evidence that eradication of hyphal structures restores taste perception [18]. This further supports the hypothesis that the presence of hyphae, rather than C. albicans carriage alone, is a significant factor contributing to taste impairment. Notably, although fluconazole effectively reduced the hyphal forms, its impact on overall Candida colony formation was less pronounced, indicating that biofilm‐associated hyphae may be the primary driver of taste dysfunction, rather than mere fungal presence. Consequently, antifungal treatment strategies targeting biofilm‐associated hyphal forms are essential, and early intervention in hyphae‐positive individuals may prevent progression to persistent taste disturbances [18, 40]. These results underscore the importance of differentiating between colonisation and active hyphal invasion when evaluating candidiasis associated taste disturbance.
Our study had several limitations. First, although our initial aim was to investigate Candida hyphae in healthy subjects, the opportunistic nature of Candida meant our cohort necessarily included individuals with heterogeneous comorbidities and medication histories, which may have affected our findings. Second, despite efforts to minimise confounding from oral lesions, the influence of other oral pathologies on taste perception could not be entirely excluded. Third, the absence of post‐treatment measurements of salivary flow limited our ability to determine whether the observed improvement in taste sensitivity following antifungal therapy was independent of salivary changes. Finally, our taste assessment methods did not incorporate more advanced techniques, such as trimatches, which might have provided further nuances in evaluating taste sensitivity.
Nevertheless, our study is the first to explore the relationship between the presence of C. albicans , particularly its hyphal phenotype, and taste dysfunction in conjunction with changes in salivary flow, thereby offering valuable insights into the pathogenesis of taste dysfunction in OC. In particular, we demonstrated that the hyphal transition of C. albicans is associated with clinically observable taste impairment, highlighting its potential clinical relevance as a diagnostic and therapeutic marker beyond mere fungal presence. Future research should explore how hyphal invasion of the oral epithelium contributes to taste dysfunction using advanced histopathological and molecular approaches and whether antifungal treatment can restore salivary flow and enhance taste perception. In particular, studies utilising transcriptomic or immunohistochemical techniques could help elucidate how Candida‐induced inflammation influences the expression and function of taste receptors and downstream signalling molecules. Additionally, in vitro or in vivo models can be used to evaluate specific interactions between fungal virulence factors and host epithelial pathways.
Our findings suggest that C. albicans carriage, especially when accompanied by hyphal forms, is associated with reduced salivary function and impaired taste sensitivity. The marked improvement in taste perception following antifungal treatment, particularly in the hyphae‐positive group, suggests that hyphal invasion plays a critical role in the pathogenesis of taste dysfunction in patients with OC. Collectively, these results underscore the importance of early identification and management of hyphal invasion to prevent persistent or long‐term taste disturbances associated with OC.
Author Contributions
Younjung Park: conceptualization, data curation, methodology, resources, writing – original draft, validation. Hyo‐Jung Jung: conceptualization, data curation, investigation, methodology, writing – original draft, formal analysis. Sin Hye Hwang: investigation, writing – original draft. Eunae Sandra Cho: writing – review and editing, resources. Hyung‐Joon Ahn: conceptualization, project administration, supervision, writing – review and editing.
Funding
This work was supported by the National Research Foundation of Korea.
Ethics Statement
This study was conducted at Yonsei University Dental Hospital between February 2021 and September 2022 in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Institutional Review Board of Yonsei University Dental Hospital (IRB No. 2–2020‐0046). The authors confirm that the ethical policies of Mycoses, as outlined in the journal's author guidelines, have been adhered to.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. A. O. Lewis and D. W. Williams , “Diagnosis and Management of Oral Candidosis,” British Dental Journal 223 (2017): 675–681.29123282 10.1038/sj.bdj.2017.886 · doi ↗ · pubmed ↗
- 2D. S. Thompson , P. L. Carlisle , and D. Kadosh , “Coevolution of Morphology and Virulence in Candida Species,” Eukaryotic Cell 10 (2011): 1173–1182.21764907 10.1128/EC.05085-11PMC 3187052 · doi ↗ · pubmed ↗
- 3J. P. Richardson , J. Ho , and J. R. Naglik , “Candida‐Epithelial Interactions,” Journal of Fungi 4 (2018): 22.29419738 10.3390/jof 4010022 PMC 5872325 · doi ↗ · pubmed ↗
- 4P. E. Sudbery , “Growth of Candida albicans Hyphae,” Nature Reviews. Microbiology 9 (2011): 737–748.21844880 10.1038/nrmicro 2636 · doi ↗ · pubmed ↗
- 5W. Yang , L. Yan , C. Wu , X. Zhao , and J. Tang , “Fungal Invasion of Epithelial Cells,” Microbiological Research 169 (2014): 803–810.24670964 10.1016/j.micres.2014.02.013 · doi ↗ · pubmed ↗
- 6J. B. Epstein , N. N. Pearsall , and E. L. Truelove , “Quantitative Relationships Between Candida albicans in Saliva and the Clinical Status of Human Subjects,” Journal of Clinical Microbiology 12 (1980): 475–476.7012183 10.1128/jcm.12.3.475-476.1980 PMC 273612 · doi ↗ · pubmed ↗
- 7I. H. Sahand , J. L. Maza , E. Eraso , et al., “Evaluation of CHROM‐Pal Medium for the Isolation and Direct Identification of Candida Dubliniensis in Primary Cultures From the Oral Cavity,” Journal of Medical Microbiology 58 (2009): 1437–1442.19608690 10.1099/jmm.0.011320-0 · doi ↗ · pubmed ↗
- 8H. Tooyama , T. Matsumoto , K. Hayashi , et al., “Candida Concentrations Determined Following Concentrated Oral Rinse Culture Reflect Clinical Oral Signs,” BMC Oral Health 15 (2015): 150.26597294 10.1186/s 12903-015-0138-z PMC 4657271 · doi ↗ · pubmed ↗