The risk factors of future exacerbations and treatment responses among different inhalation therapies of patients with preserved ratio impaired spirometry
Jun Cao, Tian Sun, Huan Yang, Lijie Zhou, Qin Shen, Ling Lin, Tao Li, Ping Zhang, Yuqin Zeng, Ping Chen, Qing Song, Si Lei, Jianmin Li

TL;DR
This study examines how different inhalation therapies affect future exacerbations in patients with preserved ratio impaired spirometry (PRISm), a condition linked to COPD.
Contribution
The study identifies risk factors for future exacerbations and compares treatment responses among inhalation therapies for PRISm patients.
Findings
Patients without inhalation therapy had higher exacerbation and hospitalization rates.
Mono-LAMA therapy is recommended for PRISm patients to reduce future exacerbation risks.
No significant differences were found among combination inhalation therapies in reducing exacerbations.
Abstract
Preserved ratio impaired spirometry (PRISm) is closely related to chronic obstructive pulmonary disease (COPD). However, there is a lack of relevant research on the treatment of patients with PRISm. Therefore, this study aimed to investigate the risk factors of future exacerbations and treatment responses among different inhalation therapies of patients with PRISm. This is a retrospective cohort study. Patients with PRISm were registered in the real-world study on the status of diagnosis and treatment of COPD (RealDTC) study between January 2017 and August 2024. Data on demographics, pulmonary function, symptom scores, number of exacerbations and hospitalisations in the past year, inhalation therapy regimens including long-acting muscarinic antagonist (LAMA), long-acting β2-agonist (LABA) + inhaled corticosteroid (ICS), LABA + LAMA, and LABA + LAMA + ICS, and comorbidities were…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
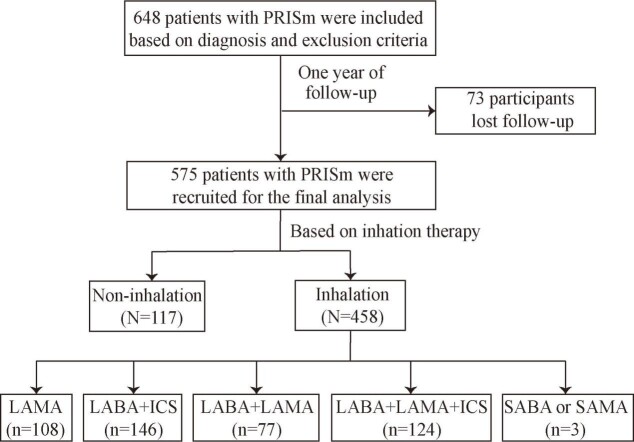 Figure 1
Figure 1| Variables | Non-exacerbation, (n = 431) | Exacerbation, (n = 144) | |
|---|---|---|---|
|
| 63.3 ± 10.3 | 65.3 ± 8.4 | 0.032* |
|
|
|
| 0.902 |
| Male | 312 (72.4) | 105 (72.9) |
|
| Female | 119 (27.6) | 39 (27.1) |
|
|
|
|
| 0.304 |
| Under junior high school | 339 (78.7) | 119 (82.6) |
|
| Over high school | 92 (21.3) | 25 (17.4) |
|
|
| 24.1 ± 4.1 | 23.6 ± 4.4 | 0.280 |
|
|
|
| 0.666 |
| Never smoker | 175 (40.6) | 61 (42.4) |
|
| Former smoker | 80 (18.6) | 30 (20.8) |
|
| Current smoker | 176 (40.8) | 53 (36.8) |
|
|
| 24.0 (0.0, 40.5) | 20.0 (0.0, 40.0) | 0.439 |
|
|
|
| <0.001* |
| Yes | 147 (34.1) | 75 (52.1) |
|
| No | 284 (66.6) | 69 (51.8) |
|
|
|
|
|
|
| FEV1%pred | 69.7 ± 11.8 | 67.5 ± 11.3 | 0.050 |
| FEV1/FVC | 75.0 ± 5.3 | 75.0 ± 4.4 | 0.951 |
|
| 13.0 ± 6.6 | 13.7 ± 5.8 | 0.254 |
|
|
|
| 0.020* |
| <10 | 140 (32.5) | 32 (22.2) |
|
| ≥20 | 291 (67.5) | 112 (77.8) |
|
|
| 1 (1, 2) | 2 (1, 2) | 0.028* |
|
|
|
| 0.170 |
| 0–1 | 229 (53.1) | 67 (46.5) |
|
| ≥2 | 202 (46.9) | 77 (53.5) |
|
|
|
|
| <0.001* |
| LAMA | 95 (22.0) | 13 (9.0) |
|
| LABA+LAMA | 63 (14.6) | 14 (9.7) |
|
| LABA+ICS | 118 (27.4) | 28 (19.4) |
|
| LABA+LAMA+ICS | 95 (22.0) | 29 (20.1) |
|
| SABA or SAMA | 2 (0.5) | 1 (0.7) |
|
| No inhalation | 58 (13.5) | 59 (41.1) |
|
|
|
|
|
|
| Chronic heart disease | 20 (4.6) | 7 (4.9) | 0.914 |
| Hypertension | 26 (6.0) | 8 (5.6) | 0.834 |
| Lung cancer | 7 (1.6) | 1 (0.7) | 0.686 |
| Diabetes | 11 (2.6) | 1 (0.7) | 0.311 |
| Bronchiectasis | 34 (7.9) | 9 (6.2) | 0.517 |
|
| 0 (0, 1) | 1 (0, 2) | 0.020* |
|
|
|
| 0.018* |
| 0 | 236 (54.8) | 60 (41.7) |
|
| 1 | 93 (21.6) | 44 (30.6) |
|
| ≥20 | 102 (23.7) | 40 (27.7) |
|
|
| 0 (0, 1) | 0 (0, 1) | <0.001* |
|
|
|
| <0.001* |
| 0 | 311 (72.2) | 76 (52.8) |
|
| ≥1 | 120 (27.8) | 68 (47.2) |
| Variables | OR | 95% CI | |
|---|---|---|---|
| Age | 1.026 | 1.004–1.049 | 0.020† |
| Biofuel exposure |
|
|
|
|
| Reference |
|
|
|
| 1.903 | 1.246–2.906 | 0.003† |
| Hospitalisations in the past year |
|
|
|
|
| Reference |
|
|
|
| 2.186 | 1.427–3.350 | <0.001† |
| Therapy |
|
|
|
|
| Reference |
|
|
|
| 1.783 | 0.769–4.145 | 0.177 |
|
| 1.851 | 0.892–3.841 | 0.099 |
|
| 1.781 | 0.854–3.714 | 0.124 |
|
| 3.070 | 0.242–38.949 | 0.387 |
|
| 8.382 | 4.117–17.066 | <0.001† |
| Variables | PSM | ||
|---|---|---|---|
|
|
|
|
|
| Exacerbations during one year (MD, IQR) | 0 (0, 2) | 0 (0, 0) | <0.001* |
| Exacerbations, n (%) |
|
| <0.001* |
|
| 55 (49.5) | 85 (19.1) |
|
|
| 56 (50.5) | 359 (80.9) |
|
| Frequent exacerbations, n (%) |
|
| <0.001* |
|
| 29 (26.1) | 34 (7.7) |
|
|
| 82 (73.9) | 410 (92.3) |
|
| Hospitalisations during one year (MD, IQR) | 0 (0, 1) | 0 (0, 0) | <0.001* |
| Hospitalisations, n (%) |
|
| <0.001* |
|
| 30 (27.0) | 44 (9.9) |
|
|
| 81 (73.0) | 400 (90.1) |
|
| All-cause of mortality, n (%) |
|
| 0.589 |
|
| 0 (0.0) | 4 (0.9) |
|
|
| 111 (100.0) | 440 (99.1) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Asthma and respiratory diseases
Preserved ratio impaired spirometry (PRISm) is a common pulmonary dysfunction that is closely related to chronic obstructive pulmonary disease (COPD), multiple comorbidities and other risk factors. The PRISm is not always a stable status and may develop into COPD over time [1,2]. Therefore, early diagnosis and treatment of patients with PRISm are crucial for preventing and treating COPD.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2024 report defined PRISm in detail and proposed that PRISm patients are at risk of developing airflow obstruction [3]. Consequently, this comorbidity subgroup has garnered increasing clinical focus. Currently, researches on patients with PRISm have predominantly centred on their prevalence, risk factors, and clinical outcomes [4–6]. Nevertheless, PRISm is strongly associated with increased respiratory symptoms [7]. Cough, sputum production, and dyspnea are prevalent respiratory manifestations in patients with PRISm. Those presenting with respiratory symptoms further demonstrate significantly elevated risks of gastrointestinal symptoms and cardiovascular complications [8,9]. In addition, exacerbations are important deterioration events for patients with chronic respiratory diseases [10]. Previous studies have shown that patients with PRISm have a risk of future exacerbations [11]. Consequently, early intervention in this population is clinically significant for reducing symptoms and the risk of exacerbations. Inhalation therapy – including long-acting β_2_-agonists (LABA), long-acting muscarinic antagonists (LAMA), and inhaled corticosteroids (ICS) – serve as a first-line therapy for COPD patients to alleviate symptoms and reduce the risk of exacerbations [3]. However, their therapeutic efficacy in patients with PRISm remains incompletely elucidated.
Therefore, this study aimed to investigate the risk factors of future exacerbations and treatment responses among different inhalation therapies of patients with PRISm.
METHODS
Study participants
This was a retrospective cohort study. The patients were registered in the real-world study on the status of diagnosis and treatment of COPD (RealDTC) study between January 2017 and August 2024, as described previously [12]. They had been diagnosed with PRISm according to the GOLD 2024 report [3]: the ratio of forced expiratory volume in one second to forced vital capacity (FEV1/FVC) was ≥ 0.7, and the forced expiratory volume in one second percentage predicted (FEV1%pred) was < 0.8 after inhaling a bronchodilator. Patients with active tuberculosis, asthma, and severe heart, liver or kidney disease were excluded from this study.
This study was approved by the ethic review board of the Second Xiangya Hospital of Central South University and conducted in accordance with the Declaration of Helsinki (2016076). All patients provided written informed consent.
Data collection
Data on age, sex, education level, body mass index (BMI), smoke history, smoking (packs/y), biofuel exposure, FEV1%pred, FEV1/FVC, COPD assessment test (CAT) scores, modified Medical Research Council (mMRC) scores, number of exacerbations and hospitalisations in the past year, comorbidities including chronic heart disease, hypertension, lung cancer, diabetes, and bronchiectasis, and inhalation therapy regimens including LAMA, LABA + LAMA, LABA + ICS, LABA + LAMA + ICS, short-acting β_2_-agonists (SABA), and short-acting muscarinic antagonists (SAMA) were recorded for patients first visited hospitals. The clinicians provided inhalation therapy regimens based on the patient’s condition.
All patients completed one year of follow-up to collect data on exacerbations, frequent exacerbations, hospitalisations, and all-cause of mortality. The patients lost to follow-up were excluded from this study.
Sample size calculation
The sample size was calculated using PASS 15.0 in the part of confidence interval (CI) for one proportion. We used the pre-experiment exacerbation incidence rate (24.9%) as the assumed sample proportion, a confidence level of 0.95, and a two-sided CI. Accounting for a 20% dropout rate, the minimum required sample size was calculated to be 556.
Variable definition
Exacerbation was defined as a condition requiring antibiotics, oral corticosteroids, or hospitalisation [13]. Frequent exacerbation was defined as two or more exacerbations per year [14]. Biofuel exposure was defined as the use of biomass fuels for cooking or heating for at least two hours per day for at least one year [15]. A former smoker has had ≥ 10 packs/y but has not smoked for more than six months, while a current smoker has had smoking exposure of ≥ 10 packs/y [16].
Prescription outcomes, including adjusting treatment, were defined as changing the inhalation therapy drugs or stopping them for more than three months during the one year of follow-up [17].
Statistical analysis
The Student’s t-test was used to analyse continuous variables with normal distributions and homogeneity of variance, and the results are expressed as mean ± standard deviation. Otherwise, the variables are expressed as median and interquartile range (IQR) and non-parametric tests was used to analyse data. The χ^2^ test or Fisher exact test was used to analyse categorical variables. Multivariate logistic regression was used to assess the relative factors for patients with PRISm who experienced exacerbations during follow-up; the variables were listed in Table 1 (P < 0.05); the odds ratio (OR) and 95% CI were calculated. Propensity score matching (PSM) between those who used inhalation therapy and those who without inhalation therapy was conducted using R package version 2.15.3 (R Foundation for Statistical Computing, Vienna, Austria), with a ratio 4:1. A value of P < 0.05 was considered statistically significant. For statistical analysis we used the SPSS 26.0 (IBM, Armonk, USA) and Free Statistics software version 1.7.1 (Beijing Fengrui Technology Co., Ltd, Beijing, China).
RESULTS
The clinical characteristics of the patients
A total of 648 patients were included based on diagnosis and exclusion criteria. During one year of follow-up, 73 patients lost to follow-up. A total of 575 patients were recruited for the final analysis (Figure 1).
Flowchart. ICS – inhaled corticosteroid, LAMA – long-acting muscarinic antagonist, LABA – long-acting β2-agonist, PRISm – preserved ratio impaired spirometry, SAMA – short-acting muscarinic antagonist, SABA – short-acting β2-agonist.
The mean age was 63.8 ± 9.9 years, with males accounting for 72.5%. A total of three (0.5%) patients received SABA or SAMA, 108 (18.8%) received LAMA, 77 (13.4%) received LABA + LAMA, 146 (25.4%) received LABA + ICS, and 124 (21.6%) received LABA + LAMA + ICS, while 117 (20.3%) patients without inhalation therapy (Table S1 in the Online Supplementary Document). During one year of follow-up, there were 144 (25.0%) patients experienced exacerbations, 65 (11.3%) experienced frequent exacerbation, and 77 (13.4%) experienced hospitalisations. There were 101 (22.1%) patients adjusted inhalation therapy during one year of follow-up (Table S2 in the Online Supplementary Document). However, for the patients without inhalation therapy at baselines did not add inhalation therapy during follow-up.
The clinical characteristics of the patients experienced exacerbation during follow-up
Patients experienced exacerbation had higher age, mMRC scores, number of exacerbations and hospitalisations in the past year. In addition, these patients had a higher proportion of CAT scores ≥20, biofuel exposure, and without inhalation therapy (P < 0.05) (Table 1).
Multivariate logistic regression analysis showed that age (OR = 1.026; 95% CI = 1.004–1.049), number of hospitalisations in the past year ≥1 (OR = 2.186; 95% CI = 1.427–3.350), and without inhalation therapy (OR = 8.382; 95% CI = 4.117–17.066) were the independent risk factors for patients experienced exacerbations (P < 0.05) (Table 2).
The future exacerbation between inhalation and non-inhalation during one year of follow-up after PSM
After PSM, 111 patients without inhalation therapy and 444 patients with inhalation therapy were analysed for future exacerbations. The baseline clinical characteristics showed no significant differences between the two groups (Table S3 in the Online Supplementary Document).
Furthermore, compared with patients who used inhalation therapy, the patients without inhalation therapy had a higher number of exacerbations, frequent exacerbations, and hospitalisations during one year of follow-up. However, there was no significant difference in all-cause of mortality between the two groups (Table 3).
The treatment responses of different inhalation therapies in patients with PRISm
After adjusting for confounding factors including age, sex, BMI, smoke history, biofuel exposure, FEV1%pred, FEV1/FVC, CAT scores, mMRC scores, exacerbations in the past year, prescription outcomes, and comorbidities, there were no significant differences in future exacerbations, frequent exacerbations, hospitalisations, and all-cause of mortality among LAMA, LABA + LAMA, LABA + ICS, and LABA + LAMA + ICS (Table S4–6 in the Online Supplementary Document).
DISCUSSION
COPD is a common, preventable and treatable disease; however, the widespread underdiagnosis and misdiagnosis lead to patients receiving improper or no treatment [3]. The GOLD report is the most widely accepted guideline among clinicians for the management and treatment of COPD. According to the GOLD report, PRISm patients will not remain in this state indefinitely. Evidence indicates that the majority of patients with PRISm patients transition to normal spirometry, whereas the remainder maintain PRISm status or progress to COPD [3]. Notably, PRISm constitutes an independent risk factor for the development of airflow limitation [18–20].
Exacerbations, as important deterioration events for patients, can accelerate pulmonary function decline and disease progression. In fact, Wallström et al. [21] found that, with follow-up extended to a median of 1.90 years for moderate exacerbations, the exacerbation rate for PRISm patients was 0.17 events per patient-year. When the follow-up was extended to a median of 1.96 years, the hospitalisation rate for PRISm patients was 0.22 events per patient-year. Yoon et al. [11] found that the annual incidence of moderate-to-severe exacerbation was 0.56 in patients with PRISm. This was similar to our results. In our study, 25.0% of patients with PRISm experienced exacerbations during one year of follow-up. In addition, we identified several independent risk factors for patients with PRISm experienced exacerbations, including age and hospitalisations in the past year. This implies that for PRISm patients of advanced age and those with a history of hospitalisations, implementing targeted therapeutic strategies to mitigate the risk of future exacerbations is imperative.
In addition, we found that without inhalation therapy was an independent risk factor for patients with PRISm experienced exacerbations. Furthermore, we found that patients treated with inhalation therapy had a lower risk of future exacerbations, frequent exacerbations, and hospitalisations. This implies that it is necessary to provide inhalation therapy for patients with PRISm to decrease the risk of future exacerbations. However, there was no significant difference in all-cause of mortality between the two groups. This might be related to the short follow-up period and the relatively low mortality rate. In addition, the patients without inhalation therapy had a higher risk of future exacerbations which may reflect systematic differences rather than treatment effect.
Inhalation therapy, including LAMA, LABA + LAMA, LABA + ICS, and LABA + LAMA + ICS, is the most commonly used treatment for patients [22]. Therefore, we analysed treatment responses among different inhalation therapies for patients with PRISm and found no significant differences in future exacerbations, frequent exacerbations, hospitalisations, and all-cause of mortality among LAMA, LABA + LAMA, LABA + ICS, and LABA + LAMA + ICS. This implies that mono-LAMA may be sufficient to reduce the risk of exacerbations in patients with PRISm, avoiding excessive medical treatment in the real-world.
This study has limitations. First, although this is a multicentre study, the sample size is relatively small. Therefore, a larger sample size will be required in future research. Second, a relatively small number of patients with PRISm used mono-SABA or SAMA, and LABA. Therefore, we cannot determine whether mono-SABA, SAMA, or LABA had efficacy similar to mono-LAMA in reducing future exacerbations. Third, this study had a relatively short follow-up period. Long-term follow-up observation of changes in pulmonary function is also particularly important. Fourth, this is a real-world study, randomised controlled trials (RCT) need to be investigated in the future. Fifth, we explicitly state that confounding by indication persists despite PSM adjustment, and that our findings should be interpreted as associative rather than causal. We further suggest that future confirmatory studies should adopt RCT designs. In addition, the heterogeneity of PRISm may exert a critically influence on treatment response. Finally, we are not sure whether it is health care access, socioeconomic status, or prescribing patterns, pulmonary function trajectories over 12 months were correlated with future exacerbations.
CONCLUSIONS
Patients with PRISm had high risk of future exacerbations. Inhalation therapy could reduce the risk of future exacerbations and clinicians should recommend mono-LAMA to patients with this condition.
Additional material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wan ES Fortis S Regan EA Hokanson J Han MK Casaburi R Longitudinal Phenotypes and Mortality in Preserved Ratio Impaired Spirometry in the COPD Gene Study. Am J Respir Crit Care Med. 2018;198:1397–405. 10.1164/rccm.201804-0663 OC 29874098 PMC 6290948 · doi ↗ · pubmed ↗
- 2Han MK Agusti A Celli BR Criner GJ Halpin DMG Roche N From GOLD 0 to Pre-COPD. Am J Respir Crit Care Med. 2021;203:414–23. 10.1164/rccm.202008-3328 PP 33211970 PMC 7885837 · doi ↗ · pubmed ↗
- 3GOLD Executive Committee. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease (REPORT). 2023. Available: https://goldcopd.org/. Accessed: 16 November 2022.
- 4Higbee DH Granell R Davey Smith G Dodd JW Prevalence, risk factors, and clinical implications of preserved ratio impaired spirometry: a UK Biobank cohort analysis. Lancet Respir Med. 2022;10:149–57. 10.1016/S 2213-2600(21)00369-634739861 · doi ↗ · pubmed ↗
- 5Huang J Li W Sun Y Huang Z Cong R Yu C Preserved Ratio Impaired Spirometry (PRI Sm): A Global Epidemiological Overview, Radiographic Characteristics, Comorbid Associations, and Differentiation from Chronic Obstructive Pulmonary Disease. Int J Chron Obstruct Pulmon Dis. 2024;19:753–64. 10.2147/COPD.S 45308638505581 PMC 10949882 · doi ↗ · pubmed ↗
- 6Choi H Oak CH Jung MH Jang TW Nam SJ Yoon T Trend of prevalence and characteristics of preserved ratio impaired spirometry (PRI Sm): Nationwide population-based survey between 2010 and 2019. P Lo S One. 2024;19:e 0307302. 10.1371/journal.pone.030730239042610 PMC 11265705 · doi ↗ · pubmed ↗
- 7Park HJ Byun MK Rhee CK Kim K Kim HJ Yoo KH Significant predictors of medically diagnosed chronic obstructive pulmonary disease in patients with preserved ratio impaired spirometry: a 3-year cohort study. Respir Res. 2018;19:185. 10.1186/s 12931-018-0896-730249256 PMC 6154818 · doi ↗ · pubmed ↗
- 8Kogo M Sato S Muro S Matsumoto H Nomura N Oguma T Longitudinal Changes and Association of Respiratory Symptoms with Preserved Ratio Impaired Spirometry (PRI Sm): The Nagahama Study. Ann Am Thorac Soc. 2023;20:1578–86. 10.1513/Annals ATS.202301-050OC 37560979 · doi ↗ · pubmed ↗