The impact of acute coronary syndrome on long-term survival in cancer patients
Daniel Finke, Markus B. Heckmann, Jessica M. Schug, Lukas F. Entenmann, Hauke Hund, Hugo A. Katus, Norbert Frey, Lorenz H. Lehmann

TL;DR
This study finds that cancer patients with acute coronary syndrome, especially NSTEMI, have higher mortality and need special care.
Contribution
The study identifies ACS, particularly NSTEMI, as a strong predictor of mortality in cancer patients, independent of other comorbidities.
Findings
Cancer patients with NSTEMI had significantly higher mortality rates compared to non-cancer patients with NSTEMI.
Cancer independently increased all-cause mortality and cardiovascular readmission risks in ACS patients.
NT-proBNP was a useful biomarker for risk stratification in cancer patients with ACS.
Abstract
Although cancer and atherosclerosis are based on shared risk factors, the impact of the acute coronary syndrome (ACS) on long-term survival in cancer patients is still unclear. We retrospectively analyzed 441 patients with initial diagnosis of cancer prior to ACS who were subjected to cardiac catheterization (CC) with a follow-up of at median 4.78 years (IQR: 0.58–9.33). These patients were compared to non-cancer ACS patients via propensity score matching according to the cardiac risk factors age, sex, arterial hypertension and diabetes. We found ACS, and overall Non-ST-elevation myocardial infarction (NSTEMI), as a relevant predictor of outcome in cancer patients with the highest mortality rates (88 deaths (40%) in non-cancer patients with NSTEMI vs. 174 deaths (64.9%), in the respective cancer patients p < 0.001). In multivariable COX models including other comorbidities, cancer was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
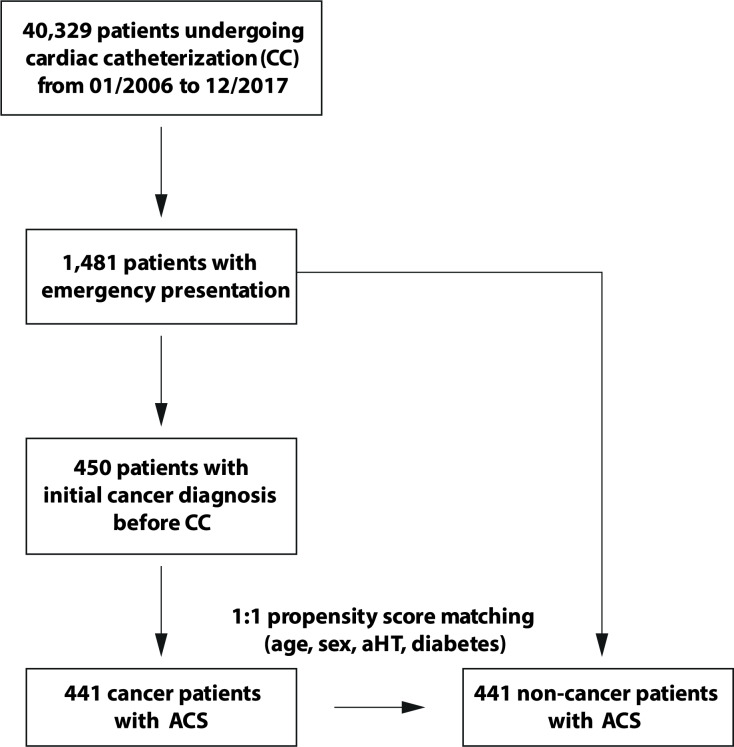 Figure 1
Figure 1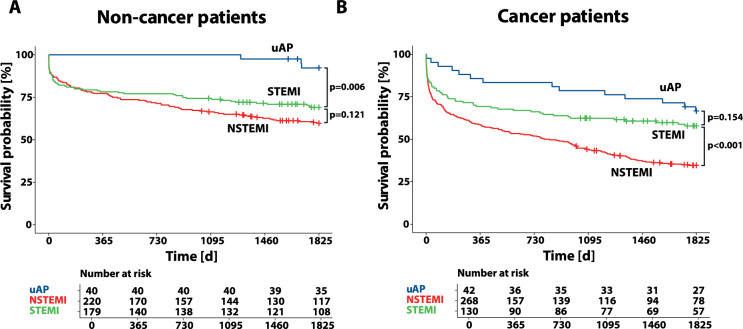 Figure 2
Figure 2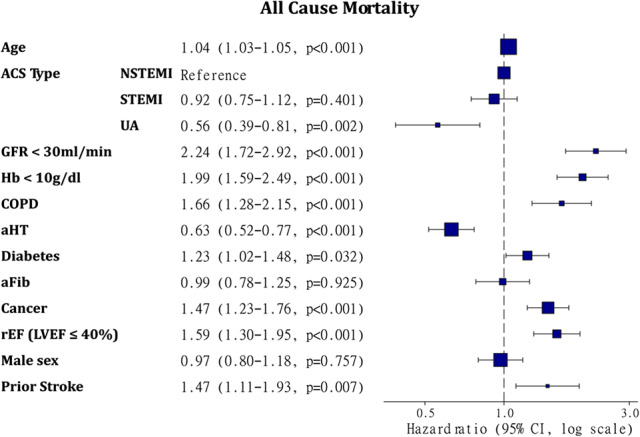 Figure 3
Figure 3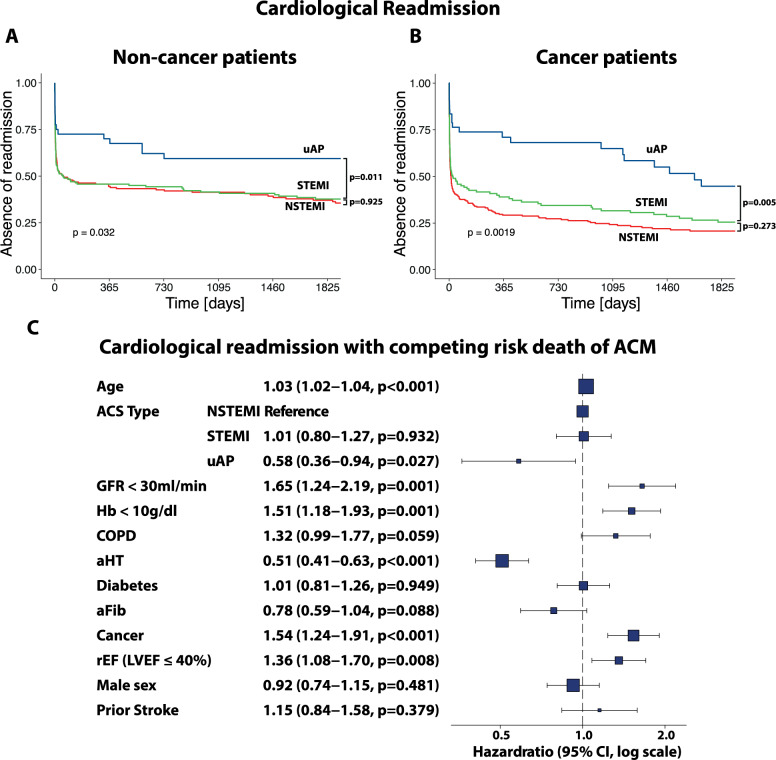 Figure 4
Figure 4- —Universitätsklinikum Heidelberg (8914)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChemotherapy-induced cardiotoxicity and mitigation · Acute Myocardial Infarction Research · Cardiac Imaging and Diagnostics
Introduction
Cancer patients are at increased risk of coronary artery disease (CAD) and acute coronary syndromes (ACS) due to their malignant disease, the related therapies and shared risk factors for cancer and atherosclerosis [1–3]. Advances in cancer therapies with the use of potentially cardiotoxic agents, lately e.g., immune checkpoint inhibitors or tyrosine kinase inhibitors, achieved major improvements in cancer survival [4, 5]. Given improved outcomes, cardiovascular complications of the underlying disease are becoming increasingly important [6]. In cancer types with many long-term survivors, such as breast cancer, cardiovascular disease is a leading cause of mortality [7].
In the 2022 ESC cardiooncology guidelines and current publications in the field, there is an emphasis on the cardiological risk assessment of oncological patients using e.g., cardiac biomarkers and cardiac imaging, mainly in stable patients, not suffering from an acute cardiac event [8–12].
Generally, there are clear guidelines on the management of ACS [13]. Nevertheless, clinical practice shows uncertainties in the implementation of these established guidelines in patients with cancer. Reasons are mostly attributed to difficulties in anti-platelet treatments after percutaneous coronary interventions (PCI) and bleeding complications [14, 15]. Given the reduced life expectancy associated with a cancer diagnosis, the clinical value of invasive cardiac assessments remains a subject of debate [15, 16].
Still, detailed data are lacking on both the long-term survival of patients with acute coronary syndrome (ACS) and concomitant cancer, as well as on effective strategies for their risk stratification. There is a gap in knowledge, if biomarkers can be used for risk stratification in cancer patients when suffering from ACS. Further it is not known, if ACS relevantly alters the morbidity of cancer patients.
Given the high overlap of cancer and risk factors for ACS, we aimed to assess, if the co-occurrence of cancer and ACS is relevant for the patients’ survival. The study also aims to evaluate the clinical features such as ACS classification (unstable Angina pectoris (uAP), ST- or Non-ST Elevation myocardial infarction (STEMI/NSTEMI)), other co-morbidities and cardiac assessments (left ventricular ejection fraction (LVEF) and CAD) in order to look for outcome-relevant potential risk factors in this patient collective. Lastly, we assessed re-hospitalization due to cardiac disease as an indicator for morbidity that is not only cancer-dependent.
These insights may contribute to improvements in clinical care for cancer patients that are suffering from ACS.
Materials and methods
Study design and patients
This retrospective matched study was conducted at the University Hospital Heidelberg. Data were acquired from patients who underwent cardiac catheterization (CC) at University Hospital Heidelberg between January 1, 2006 and December 31, 2017. The first CC of each patient was considered for the analysis. We selected a subgroup of patients who were subjected to CC in an emergency setting. These patients’ medical records were screened for ACS subtype specification (ST-elevation myocardial infarction (STEMI), NSTEMI and unstable Angina (uAP)). The cancer group consists of patients with an initial diagnosis of the malignant disease before CC. We included patients with the diagnosis of gastrointestinal cancer (ICD-10: C15, C16, C18, C19, C20, C22, C24, C25, C78.7, D01.0), lung cancer (ICD-10: C34, C78.0), breast cancer (ICD-10: C50, D05), melanoma/skin tumors (ICD-10: C43, C44, D03, D04), prostate cancer (ICD-10: C61), leukemia (ICD-10: C91, C92, C93, D45, D46, D47), lymphoma (ICD-10: C81, C82, C83, C84, C85), kidney tumors (ICD-10: C64, C65), soft tissue tumors (ICD-10: C46, C48, C49) and others (ICD-10: C02, C03, C07, C09, C11, C14, C32, C37, C40, C51, C53, C54, C55, C56, C60, C62, C67, C69, C71, C73, C80, C90, D00.0, D09, D32, D33, D35, D39, D41, D43, Y35.7). Non-cancer patients were matched according to age, sex, diabetes and arterial hypertension to serve as a control group.
The study protocol was approved by the ethics committee of the Medical Faculty of the University of Heidelberg (S-286/2017, 390/2011). The investigation conformed with the principles outlined in the Declaration of Helsinki.
Data acquisition
Patient specific data were obtained in the clinical routine and were extracted from electronic medical records including demographic data, ACS classifications, laboratory results (including creatinine, hemoglobin (Hb), C-reactive protein (CRP), leucocyte count, high-sensitivity cardiac troponin T (hs-cTnT) and N-terminal prohormone of brain natriuretic peptide (NT-proBNP)), angiographic measurements and hospital readmission at University Hospital Heidelberg on a cardiological ward using the cardiac Research Data Warehouse (RWH). LVEF was assessed during CC via laevo-cardiography. Laboratory values that were assessed between seven days prior to seven days after the CC were considered for further analysis. Generally, the values closest to CC were taken into account. In terms of hs-cTnT, that is often measured repeatedly for ACS rule-out, we took the highest value. The oncological diagnosis (ICD-10 code), the metastasis status, date of diagnosis and type of treatment were retrieved from the Clinical Registry of the National Centre for Tumor Diseases (NCT) Heidelberg. Data of all-cause mortality and date of death were obtained from the registration office from the patients’ place of residence. Follow-up of ACM was analyzed by October 1, 2020.
In the clinical routine, in a subgroup of patients hs-cTnt and NT-proBNP was assessed. Measurement of hs-cTnT in plasma samples was performed using the Elecsys^®^ Troponin T high sensitive hs-cTnT assay (Roche Diagnostics) in the central laboratory at Heidelberg University Hospital. Limit of blank (LoB), Limit of detection (LoD), 10% coefficient of variation (CV) and 99th percentile cut-off values for the hs-cTnT assay were 3 ng/L, 5 ng/L, 13 ng/L and 14 ng/L. N-terminal pro brain‐type natriuretic peptide was measured at the same timepoint using the Stratus^®^ CS Acute Care™ NT‐proBNP assay (Siemens AG, Berlin and Munich, Germany).
Definitions
Impairments in the LVEF were defined as previously published and recommended in the guidelines of the European Society of Cardiology (ESC) from 2021. A reduced left ventricular ejection fraction (rEF) was defined as LVEF ≤ 40% [17]. Coronary stenosis ≥ 50% were used as cut-off for the occurrence CAD [18]. The diagnoses of COPD, stroke, diabetes and arterial hypertension prior to the CC were taken the medical reports. We used the cut-off Hb < 10 g/dl for detection of a relevant anemia with known impact on the outcome of heart failure patients as published earlier [19]. As a measure of kidney dysfunction we used the glomerular filtration rate (GFR) with a cutoff of 30 ml/min/1,73m^2^ for severely decreased kidney function and renal failure as suggested by the KDIGO [20]. An active oncological treatment was defined as chemotherapy or radiation that was administered within 6 months before the time of ACS.
Statistical analysis
In order to compare continuous variables according to cancer status, we used the Wilcoxon-rank sum test. The variables were presented as median values with interquartile range (IQR). Dichotomic data were compared using the Chi-squared test and is presented as numbers of events and percentages. A confidence interval of 95% was considered significant.
1:1 propensity score matching was performed with the use of MatchIt package (version 4.5.4) according to age, sex, diabetes and arterial hypertension. Nearest neighbor matching was performed. The distance measure was estimated via logistic regression. No units were discarded before matching. Thus, we were able to obtain an adequate balance of propensity scores between the cancer and non-cancer group (Supplemental Fig. 1).
Multivariable COX models were calculated in R (version 4.3.1) using the survival package (version 3.7.0). The model was illustrated as a forest plot using the survminer package (version 0.4.9).
Survival analysis shown in Kaplan Meier curves were also calculated in R using the survival package (version 3.7.0) and illustrated with help of the survminer package (version 0.4.9). Adjusted survival curves were built with the adjustedCurves package (version 0.11.2). Survival in dependence of ACS classification was adjusted to diabetes, aHT, Age > 65, male sex, rEF, COPD and prior stroke using a Cox multivariable model (Supplemental Fig. 2). The time-to-event in survival analyses was defined as the difference between the date of the CC due to ACS and the date of death. Data were censored when the observation interval was lower than 5 years. The log-rank test was used to determine differences in survival. A p-value < 0.05 was considered significant.
To account for competing risks in the time-to-event analyses, we employed Fine and Gray’s subdistribution hazard model for competing risk regression. Specifically, we modeled the cumulative incidence of rehospitalization events, considering death as a competing event. Models were fitted, subdistribution hazard ratios (SHRs) and their corresponding 95% confidence intervals (CIs) were estimated using the cmprsk package (version 2.2.12), and results were organized with the finalfit package (version 1.0.8).
Tables were created with the use of packages tableone (version 0.13.2), flextable (version 0.9.2) and utile.tables (version 0.3.0). Data wrangling was supported by the tidyverse package (version 2.0.0). Figures were composed in Adobe Illustrator (version 29.0.1). Bar charts and pie charts were illustrated in GraphPad Prism (version 10.4.1.).
Results
40,329 patients underwent CC between January 2006 and December 2017 at University Hospital Heidelberg. Among those, 3,666 patients were diagnosed with cancer prior to CC. Risk stratification using cardiac parameters in the total cancer group including LVEF, CAD and biomarkers was published earlier [21]. As a subgroup, 1,481 patients with an emergency presentation were identified in the present analysis. 450 patients were diagnosed with cancer prior to the presentation for CC, with nine patients being excluded due to a missing diagnosis of ACS. 441 cancer patients and 441 propensity score matched non-cancer patients were followed up for further analysis (Fig. 1, Suppl. Figure 1).
Fig. 1. Flowchart of patient selection. 40,329 patients underwent cardiac catheterization. 1,481 of these patients presented as an emergency examination. Among those, we found 450 patients with a prior diagnosis of cancer. 441 cancer patients could be verified as ACS cases. Non-cancer controls with ACS were propensity score matched according to age, sex, arterial hypertension (aHT) and diabetes
The median age of all patients in the study was 80.1 years, 67.1% of patients were male, 69.6% were diagnosed with arterial hypertension and 28.3% were diabetic. These parameters were used for propensity score matching and, thus, equally distributed in the cancer and non-cancer group that were further analyzed. The most prevalent malignant diseases in the patients of this study were gastrointestinal cancer (15.6%), basal cell tumors (11.8%) and breast cancer (8.6%). Metastasis were known in 5% of cancer patients. At the time of ACS, 11.8% of patients had an active oncological therapy within the last 6 months. Cancer patients had significantly more diagnoses of comorbidities, such as COPD or prior stroke. Neither left ventricular function nor high-grade coronary stenosis, nor the cardiac biomarker hs-cTnT, nor NT-proBNP showed any relevant differences between the two groups (Suppl. Figure 2, Table 1). Cancer patients were more frequently diagnosed with NSTEMI (49.9% vs. 60.8%, p = 0.001) and less frequently with STEMI (41% vs. 29.7%, p < 0.001). PCI rates (51.7% vs. 51.5%, p = 0.945) and the frequency of coronary artery bypass graft (CABG) surgery (6.8% vs. 4.5%, p = 0.145) did not differ significantly between non-cancer and cancer patients. In NSTEMI patients, the rate of PCI was slightly lower than in the total cohort and comparable between the groups (Suppl. Figure 3). Medical therapies, including anti-platelet therapies, heart failure medication and statins were significantly less frequently administered in the cancer group (Table 1).
Table 1. Patient characteristics according to cancer diagnosis. ACE/AT1-inhibitors: angiotensin-converting enzyme and angiotensin II type 1 receptor inhibitors, ACS: acute coronary syndrome, CABG: coronary artery bypass graft, CAD: coronary artery disease, COPD: chronic obstructive pulmonary disease, hs-cTnT: high-sensitivity cardiac troponin T, LAD: left anterior descending artery, LCA: left coronary artery, LCX: left circumflex artery, LDH: lactate dehydrogenase, LVEF: left ventricular ejection fraction, mref: mildly reduced ejection fraction, NOAC: non-vitamin K antagonist anticoagulant, NSTEMI: Non-ST-elevation myocardial infarction, NT-proBNP: N-terminal prohormone of brain natriuretic peptide, PCI: percutaneous coronary intervention, pEF: preserved ejection fraction, RCA: right coronary artery, rEF: reduced ejection fraction, STEMI: ST-elevation myocardial infarction, uAP: unstable anginaPatientsOverall(n = 882)Non-cancer(n = 441)Cancer(n = 441)p-valueAge [years] (mean ± SD)80.1 ± 11.480.1 ± 11.580.2 ± 11.30.9433Male sex (%)592 (67.1%)293 (66.4%)299 (67.8%)0.667Medical history Arterial hypertension614 (69.6%)311 (70.5%)303 (68.7%)0.558 Diabetes250 (28.3%)124 (28.1%)126 (28.6%)0.881 Atrial fibrillation128 (14.5%)60 (13.6%)68 (15.4%)0.444 Heart failure119 (13.5%)52 (11.8%)67 (15.2%)0.139 COPD88 (10%)34 (7.7%)54 (12.2%)0.025 Stroke75 (8.5%)28 (6.3%)47 (10.7%)0.022Cancer history Time difference cancer diagnosis to ACS years6.8 ± 7.136.8 ± 7.13 Melanoma12 (1.4%)12 (2.7%) Squamous cell tumor21 (2.4%)21 (4.8%) Basal cell tumor52 (5.9%)52 (11.8%) Other skin tumor5 (0.6%)5 (1.1%) Gastrointestinal tumor69 (7.8%)69 (15.6%) Prostate cancer53 (6%)53 (12%) Breast cancer38 (4.3%)38 (8.6%) Lung cancer32 (3.6%)32 (7.3%) Lymphoma30 (3.4%)30 (6.8%) Leukemia24 (0.3%)24 (5.4%) Kidney tumor13 (1.5%)13 (2.9%) Soft tissue tumor12 (1.4%)12 (2.7%) Other tumor80 (9.1%)80 (18.1%) Known metastatic disease22 (2.5%)22 (5%)Known oncologic therapy Active therapy52 (5.9%)52 (11.8%) Chemotherapy73 (4.3%)73 (16.6%) Radiotherapy139 (15.8%)139 (31.5%) Operation102 (11.6%)102 (23.1%) Stemcell transplantation3 (0.3%)3 (0.7%) Other therapy30 (3.4%)30 (6.8%)LVEF pEF171 (19.4%)89 (20.2%)82 (18.6%)0.551 mrEF193 (21.9%)108 (24.5%)85 (19.3%)0.061 rEF421 (47.7%)193 (43.8%)228 (51.7%)0.021 CAD (any stenosis ≥ 50%)740 (83.9%)374 (84.8%)366 (83%)0.464Proximal coronary stenoses (≥ 90%) High-grade stenosis (LCA, main stem)31 (3.5%)16 (3.6%)15 (3.4%)0.855 High-grade stenosis (LAD)77 (8.7%)42 (9.5%)35 (7.9%)0.404 High-grade stenosis (LCX)49 (5.6%)27 (6.1%)22 (5%)0.462 High-grade stenosis (RCA)102 (11.6%)50 (11.3%)52 (11.8%)0.833Lab. results (mean ± SD) Hb [mg/dl]12.4 ± 2.3 (n = 860)12.9 ± 2.1 ( n = 434)11.8 ± 2.3 (n = 426)< 0.0001 Leukocytes [number/nl]11 ± 7 (n = 844)11 ± 5 (n = 432)12 ± 9 (n = 412)0.579 Platelets [number/nl]248 ± 110 (n = 858)243 ± 84 (n = 434)253 ± 131 (n = 424)0.1606 GFR [ml/min]66.3 ± 25,9 (n = 869)68.7 ± 25.3 (n = 438)63.9 ± 26.3 (n = 431)0.0007 C-reactive protein [mg/dl]55 ± 63.5 (n = 678)46 ± 57.9 (n = 330)64 ± 67.3 (n = 348)0.0002 LDH [U/l]269.2 ± 93.9 (n = 118)255.1 ± 85.2 (n = 45)278 ± 98.5 (n = 73)0.1886 Hs-cTnT [ng/l]2998.1 ± 7236.3 (n = 528)3423.2 ± 8708 (n = 238)2649 ± 5747.3 (n = 290)0.24 NT-proBNP [ng/l]7385 ± 14233.1 (n = 252)6074 ± 10727.3 (n = 142)9078 ± 17677.9 (n = 110)0.1179ACS and therapy NSTEMI488 (55.3%)220 (49.9%)268 (60.8%)0.001 STEMI312 (35.4%)181 (41%)131 (29.7%)< 0.001 uAP82 (9.3%)40 (9.1%)42 (9.5%)0.817 PCI455 (51.6%)228 (51.7%)227 (51.5%)0.946 CABG50 (5.7%)30 (6.8%)20 (4.5%)0.145Medication Aspirin694 (78.7%)363 (82.3%)331 (75.1%)0.009 Clopidogrel388 (44%)212 (48.1%)176 (39.9%)0.015 Ticagrelor158 (17.9%)71 (16.1%)87 (19.7%)0.16 Prasugrel26 (2.9%)19 (4.3%)7 (1.6%)0.015 Heparin188 (21.3%)87 (19.7%)101 (22.9%)0.25 Marcumar83 (9.4%)46 (10.4%)37 (8.4%)0.299 NOAC25 (2.8%)9 (2%)16 (3.6%)0.156 Beta-receptor blocker676 (76.6%)355 (80.5%)321 (72.8%)0.007 Statins659 (74.7%)351 (79.6%)308 (69.8%)0.001 ACE/AT1-Inhibitors643 (72.9%)346 (78.5%)297 (67.3%)< 0.001 Aldosterone antagonist134 (15.2%)70 (15.9%)64 (14.5%)0.574Outcome 5 year all-cause mortality391 (44,3%)148 (33,6%)243 (55,1%)< 0.001 Cardiac Readmission [5 years]569 (64.5%)254 (57.6%)315 (71.4%)< 0.001 Median survival [months] (median ± SD)13.5 ± 40.827 ± 46.98.5 ± 33.5< 0.0001
5-year overall survival is dependent on ACS classification
Survival analyses were performed in non-cancer and cancer patients according to ACS classification (uAP, NSTEMI and STEMI). The total 5-year OS was generally lower in cancer patients, whereas uAP patients showed the highest OS and NSTEMI patients the lowest OS in both non-cancer and cancer patients. Differences were particularly pronounced in cancer patients, with mortality rates differing significantly between STEMI and NSTEMI patients primarily in the cancer group (p < 0.001, log-rank test). While similar differences between STEMI and NSTEMI mortality were observed in non-cancer patients, they were less pronounced and did not reach statistical significance (p = 0.121, log-rank test; Fig. 2). The Kaplan-Meier analysis maintained the same pattern after adjusting for confounders (diabetes, aHT, age > 65 years, male sex, rEF (LVEF ≤ 40%), COPD and stroke (Suppl. Figure 4).
Fig. 2. Kaplan Meier survival analysis according to ACS classification (uAP, NSTEMI and STEMI) in (A) non-cancer and B cancer patients. P-values were calculated via the log-rank test
Cancer is relevant for the survival in ACS patients
Multivariable COX models for prediction of 5-year all-cause mortality including age, ACS type (NSTEMI, STEMI, uAP), kidney dysfunction (GFR < 30 ml/min), anemia (Hb < 10 g/dl), COPD, aHT, diabetes, atrial fibrillation (aFib), reduced ejection fraction (rEF), male sex and prior stroke were built in all patients, including cancer and non-cancer patients.
The diagnosis of cancer was found as an independent predictor (HR: 1.47, CI: 1.23-1.76, p < 0.001) of mortality in the ACS patient group. The HR of cancer is comparable to other well-established comorbidities of CAD patients, such as stroke (HR: 1.47, CI: 1.11-1.93, p = 0.007) and LVEF ≤ 40% (HR: 1.59, CI: 1.30-1.95, p < 0.001). Among the ACS types, NSTEMI was associates with the worst outcome (Fig. 3).
Fig. 3. Forest plots representing Cox multivariable logistic regression model for 5-year all-cause mortality in the total ACS group (n = 879) including age, ACS type (NSTEMI, STEMI, uAP), GFR < 30 ml/min, Hb < 10 mg/dl, COPD, arterial hypertension (aHT), diabetes, atrial fibrillation (aFib), reduced ejection fraction (rEF), male sex and prior stroke. CI: confidence interval, COPD: chronic obstructive pulmonary disease, GFR: glomerular filtration rate, HR: Hazard ratio, LVEF: left ventricular ejection fraction, rEF: reduced ejection fraction
Predictive value of cardiac comorbidity is preserved in cancer patients with ACS
The same COX model was calculated in the cancer group. We found a preserved predictive value of age (HR: 1.02, CI: 1.01–1.04, p = 0.001), GFR < 30 ml/min (HR: 2.14, CI: 1.50–3.01, p < 0.001), Hb < 10 g/dl (HR: 2.08, CI: 1.59–2.72, p < 0.001), LVEF ≤ 40% (HR: 1.43, CI: 1.09–1.87, p = 0.01) and stroke (HR: 2.01, CI: 1.43–2.83, p < 0.001).
In the propensity score matched non-cancer group, we found a significant predictive value of age (HR: 1.06, CI: 1.05–1.08, p < 0.001), GFR < 30 ml/min (HR: 3.38, CI: 2.12–5.39, p < 0.001), COPD (HR: 2.46, CI: 1.62–3.74, p < 0.001) and LVEF ≤ 40% (HR: 1.96, CI: 1.43–2.68, p < 0.001; Suppl. Figure 5). Apart from prior stroke and anemia, the impact of classical cardiovascular comorbidities, risk factors and cardiac diseases on mortality, reflected in HRs, was higher in the non-cancer group.
Cardiac readmission is higher in cancer patients
The rate of rehospitalization to a cardiological ward was higher in cancer patients within five years after ACS (71.4% in cancer and 57.6% in non-cancer patients, p < 0.001). Compared to STEMI, there was a tendency towards higher readmission rates with NSTEMI in cancer patients (p = 0.273, log-rank test) that was not seen in non-cancer patients (p = 0.925, log-rank test, Fig. 4A-B). Evaluating the predictive factors influencing cardiac readmission in competing risk analysis of ACM, again we found cancer (HR: 1.54, CI: 1.24–1.91, p < 0.001) as an independent determinant, indicating its role in cardiac comorbidity independent of generally higher mortality rates in cancer patients.
Fig. 4. Kaplan Meier plots representing multivariate, competing risk analysis of readmission to a cardiological ward, adjusted to 5-year all-cause mortality (ACM) in (A) non-cancer and B cancer patients. C Forest plot of a multivariate model for cardiological readmission with the competing risk of ACM including age, ACS type (NSTEMI, STEMI, uAP), GFR < 30 ml/min, Hb < 10 mg/dl, COPD, arterial hypertension (aHT), diabetes, atrial fibrillation (aFib), reduced ejection fraction (rEF), male sex and prior stroke. COPD: chronic obstructive pulmonary disease, GFR: glomerular filtration rate, HR: Hazard ratio, LVEF: left ventricular ejection fraction, rEF: reduced ejection fraction
Next to cancer, age (HR: 1.03, CI: 1.02–1.04, p < 0.001), GFR < 30 ml/min (HR: 1.65, CI: 1.24–2.19, p < 0.001), Hb < 10 g/dl (HR: 1.51, CI: 1.18–1.93, p = 0.001) and LVEF ≤ 40% (HR: 1.36, CI: 1.08–1.70, p = 0.008) were significantly associated with higher readmission rates (Fig. 4C). The same model was calculated in the two groups separately. Kidney dysfunction (HR: 2.47, CI: 1.52–4.01, p < 0.001) and rEF (LVEF ≤ 40%) was significantly associated with higher hospitalization only in non-cancer (HR: 1.53: CI: 1.06–2.2, p = 0.024). Anemia was only seen in cancer patients with a significant association to readmission (HR: 1.57, CI: 1.18–2.10, p = 0.002, Suppl. Figure 6).
Cardiac biomarkers in risk stratification of ACS patients with cancer
In the clinical routine hs-cTnT was assessed in 528/882 patients and NT-proBNP in 252/882 patients. The clinical characteristics of the patients with available biomarker measurements are shown in Suppl. Tables 1 and 2. Hs-cTnT and NT-proBNP levels are higher in NSTEMI and STEMI patients in line with higher mortality rates compared to uAP patients in the non-cancer and cancer group (Suppl. Figure 7). The predictive value of hs-cTnT and NT-proBNP on 5-year ACM in a subgroup of the patients, where biomarker values were available, was tested. We found a significant association for NT-proBNP with ACM in cancer and non-cancer patients (non-cancer: univariate HR: 1.99, CI: 1.59–2.5, p < 0.001; cancer: univariate HR: 1.28, CI: 1.14–1.44, p < 0.001), whereas hs-cTnT showed no predictive character in cancer patients with minor effects in the non-cancer group (non-cancer: univariate HR: 1.16, CI: 1.06–1.27, p = 0.001, cancer: univariate HR: 1.02, CI: 0.96–1.08, p = 0.52). The predictive character of NT-proBNP was preserved when the COX model was adjusted to hs-cTnT (model 1), hs-cTnT and creatinine (model 2), hs-cTnT and rEF (LVEF ≤ 40%) (model 3), hs-cTnT, male sex, age > 65 years, diabetes and aHT (model 4) or hs-cTnT, NSTEMI and STEMI (model 5) in cancer and non-cancer patients (Table 2).
Table 2. Univariate and multivariable model evaluating prediction of 5-year all-cause mortality using cardiac biomarkerNon-cancerCancerUnivariateVariablenEventHR [CI]p-valueVariablenEventHR [CI]p-valuelog2(hs-cTnT)238831.158 [1.06–1.265]0.00117log2(hs-cTnT)2901581.02 [0.961–1.083]0.521log2(NT-proBNP)142351.993 [1.588–2.501]< 0.0001log2(NT-proBNP)110561.28 [1.141–1.435]< 0.0001MultivariableModel1log2(hs-cTnT)101260.986 [0.842–1.156]0.866log2(hs-cTnT)91450.906 [0.797–1.029]0.130log2(NT-proBNP)101262.73 [1.952–3.818]< 0.0001log2(NT-proBNP)91451.311 [1.15–1.495]< 0.0001Model2log2(hs-cTnT)100251.024 [0.857–1.222]0.7972log2(hs-cTnT)77350.917 [0.779–1.078]0.2939log2(NT-proBNP)100252.341 [1.662–3.299]< 0.0001log2(NT-proBNP)77351.197 [1.018–1.409]0.0298Creatinine100251.542 [1.108–2.146]0.0103Creatinine77352.025 [1.064–3.855]0.0317Model3log2(hs-cTnT)101261.007 [0.851–1.192]0.934log2(hs-cTnT)91450.903 [0.795–1.026]0.118582log2(NT-proBNP)101262.846 [2.006–4.038]< 0.0001log2(NT-proBNP)91451.288 [1.121–1.478]0.000336rEF (LVEF ≤ 40%)101260.665 [0.286–1.546]0.343rEF (LVEF ≤ 40%)91451.313 [0.696–2.478]0.400225Model4log2(hs-cTnT)101261.015 [0.857–1.202]0.8648log2(hs-cTnT)91450.91 [0.794–1.042]0.170800log2(NT-proBNP)101262.762 [1.919–3.975]< 0.0001log2(NT-proBNP)91451.267 [1.1-1.458]0.000999Male sex101261.283 [0.542–3.035]0.5709Male sex91450.909 [0.474–1.746]0.775485Age > 65 years101260.751 [0.082–6.878]0.8001Age > 65 years91452.304 [0.523–10.141]0.269737Diabetes101262.915 [1.226–6.934]0.0155Diabetes91451.123 [0.592–2.131]0.722043Hypertension101260.886 [0.385–2.041]0.7765Hypertension91451.134 [0.57–2.259]0.719879Model5log2(hs-cTnT)101260.9 [0.708–1.144]0.388log2(hs-cTnT)91450.939 [0.809–1.089]0.404log2(NT-proBNP)101262.764 [1.985–3.849]< 0.0001log2(NT-proBNP)91451.312 [1.148–1.501]< 0.0001NSTEMI10126111467323.131 [0-Inf]0.997NSTEMI91450.74 [0.259–2.114]0.574STEMI10126105269425.782 [0-Inf]0.997STEMI91450.51 [0.139–1.866]0.309Hs-cTnT High-sensitivity cardiac troponin T, LVEF Left ventricular ejection fraction, NSTEMI Non-ST-elevation myocardial infarction, NT-proBNP N-terminal prohormone of brain natriuretic peptide, STEMI ST-elevation myocardial infarction
Discussion
Although the cardiological care of oncological patients has gained more attention in the recent years, the prognostic relevance of ACS in patients with cancer remains insufficiently described.
Our findings indicate that NSTEMI in particular is a risk factor that predisposes for increased ACM rates, especially in cancer patients. We performed propensity score matching according to risk factors, which resulted in comparable groups regarding the coronary status and cardiac function. Nevertheless, cancer patients exhibit a more extensive burden of co-morbidities, such as prior stroke or COPD.
Still, cancer was found to be a relevant, independent predictor for 5-year mortality in all ACS patients that were analyzed. The independent impact of cancer on survival was comparable to other cardiovascular risk factors, such as renal dysfunction, diabetes or heart failure. We observed similar results in terms of readmission due to cardiac events, indicating higher cardiac morbidity in the cancer group. The readmission rate is independent of the generally higher overall mortality observed in cancer patients. The use of cardiac biomarkers for risk stratification was limited in the study patients, but NT-proBNP demonstrated a predictive value in cancer patients.
Little is known about the interaction of ACS and cancer, particularly regarding its impact on long-term survival. Prior studies mostly described in-hospital mortality [22] or short observational periods up to one year [14, 16, 23]. As reported earlier by others, we found as well higher rates of NSTEMI in the cancer group [23]. This may correlate with the higher burden of comorbidities and history of chronic diseases in the cancer group, NSTEMI patients are also known for [24].
Frailty, comorbidities, and increased bleeding risks may lead to less invasive treatments in cancer patients and question the impact of ACS on the patients’ outcome. Undertreatment of ACS, especially NSTEMI, has been consistently reported in cancer patients [14, 16, 25].
Of note, invasive treatments including PCI (non-cancer: 51.7%, cancer: 51.5%) and CABG (non-cancer: 6.8%, cancer: 4.5%) were comparable in our cancer and non-cancer groups.
In line with data from non-cancer patients, patients with NSTEMI showed the highest mortality [26, 27]. The higher mortality in the NSTEMI group may further be due to less stringent recommendations for immediate invasive diagnostics compared to STEMI and delayed therapies [13]. On the other hand, only approximately 50% of the NSTEMI patients showed a significant coronary stenosis with the need for revascularization.
Interestingly, we found fewer medical treatments, e.g., in terms of antiplatelet treatments, beta-receptor blocker, ACE/AT1-inhibitor and statin use in the cancer group. These drugs are known to be highly relevant for the patients’ mortality [28–30]. Recently, it was shown that the medical therapy could also improve the morbidity and daily life management in terminal cancer patients [31]. The medical undertreatment may be an additional factor next to the higher accumulation of comorbidities that may explain worse outcome of the cancer patients.
Apart from the comorbidity status, we asked if the cardiac biomarkers hs-cTnT and NT-proBNP may predict the outcome in cancer patients with ACS. The two markers have increasing relevance for risk stratification in cancer patients before and during systemic oncological therapies in stable patients [8, 10, 32–34]. Several studies in non-cancer populations have demonstrated a predictive role of NT-proBNP in ACS, particularly in cases of unstable angina (uAP) and NSTEMI [35–38].
In the present study, we found NT-proBNP to be predictive for ACM in the non-cancer and cancer group. This finding was maintained by several adjustments to creatinine, hs-cTnT, risk factors, cardiac function and ACS classifications. The predictive role of NT-proBNP in our cancer group may be further explained by the comorbidity burden, including COPD [39]. Hs-cTnT showed a minor predictive value in the present study and only in the non-cancer group. This might be explained by a selection bias of hs-cTnT assessments in only a subset of the patients.
Conclusions
This study provides the first evaluation of the long-term outcomes in patients with ACS and concomitant cancer. Our findings highlight that ACS, particularly NSTEMI, is associated with reduced survival and increased rehospitalization in cancer patients. Although we could not find evidence for undertreatment in terms of invasive therapies between cancer and non-cancer patients, the high mortality of NSTEMI in general demands precaution in handling these patients.
Despite its retrospective design, the study provides evidence supporting a more thorough evaluation of comorbidities in this patient population, as well as the assessment of cardiac biomarkers, particularly NT-proBNP. Special considerations should be taken, if withholding optimized medical treatments in cancer patients with ACS. Further prospective studies need to warrant these findings.
Study limitations
There are several limitations of the present study that need to be acknowledged. This is a monocentric, retrospective case control study, which may have led to a selection bias, e.g., the selection of patients in both groups that were subjected to the invasive therapies in the first place. Due to the retrospective nature of the study, there may be also limitations in the homogeneity of the selected data. Cardiac catheterizations of the study patients were performed over a period of eleven years. During this time, there may have been slight differences in the catheterization procedure, even though standardized methods were used at the institution. Some data, such as biomarker measurements (hs-cTnT, NT-proBNP) were not available for every patient. The mean age of the study patients in both, the cancer and non-cancer group, was relatively high in comparison to other clinical studies. This may alter the applicability of the results to other cohorts. There was a lack of data concerning some cardiac risk factors, such as smoking and lipid profiles. We had access to reliable data of ACM and hospitalization, but scarce data on the cause of death, e.g., due to cardiovascular or oncological causes.
Supplementary Information
Supplementary Material 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lenneman CG, Sawyer DB. Cardio-Oncology: an update on cardiotoxicity of Cancer-Related treatment. Circ Res. 2016;118(6):1008–20. https://doi.org/10.1161/CIRCRESAHA.115.303633.10.1161/CIRCRESAHA.115.30363326987914 · doi ↗ · pubmed ↗
- 2Lin EP, Hsu CY, Berry L, Bunn P, Shyr Y. Analysis of cancer survival associated with immune checkpoint inhibitors after statistical adjustment: A systematic review and Meta-analyses. JAMA Netw Open. 2022;5(8):e 2227211. https://doi.org/10.1001/jamanetworkopen.2022.27211.10.1001/jamanetworkopen.2022.27211 PMC 938654335976648 · doi ↗ · pubmed ↗
- 3Pottier C, Fresnais M, Gilon M, Jerusalem G, Longuespee R, Sounni NE. Tyrosine kinase inhibitors in cancer: breakthrough and challenges of targeted therapy. Cancers (Basel). 2020;12(3). 10.3390/cancers 12030731.10.3390/cancers 12030731 PMC 714009332244867 · doi ↗ · pubmed ↗
- 4Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, Chambers CE, Ellis SG, Guyton RA, Hollenberg SM, Khot UN, Lange RA, Mauri L, Mehran R, Moussa ID, Mukherjee D, Nallamothu BK, Ting HH. F. American College of Cardiology, G. American Heart Association Task Force on Practice, A. Society for Cardiovascular, and Interventions, 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention. A report of the American College of Cardiology Foundation/American Heart Association Task · doi ↗ · pubmed ↗
- 5CKDWG, Kidney Disease: Improving Global Outcomes. Kidney Int. 2024;105(4S):S 117–314. 10.1016/j.kint.2023.10.018. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease.10.1016/j.kint.2023.10.01838490803 · doi ↗ · pubmed ↗
- 6Nowak MM, Niemczyk M, Florczyk M, Kurzyna M, Paczek L. Effect of Statins on All-Cause mortality in adults: A systematic review and Meta-Analysis of propensity Score-Matched studies. J Clin Med. 2022;1119. 10.3390/jcm 11195643.10.3390/jcm 11195643 PMC 957273436233511 · doi ↗ · pubmed ↗
- 7Abi Khalil C, Al Habib KF, Singh R, Asaad N, Alfaleh H, Alsheikh-Ali AA, Sulaiman K, Alshamiri M, Alshaer F, Al Mahmeed W. Al Suwaidi, beta-Blocker therapy prior to admission for acute coronary syndrome in patients without heart failure or left ventricular dysfunction improves In-Hospital and 12-Month outcome: results from the GULF-RACE 2 (Gulf registry of acute coronary Events-2). J Am Heart Assoc. 2017;6(12). 10.1161/JAHA.117.007631.10.1161/JAHA.117.007631 PMC 577905929263035 · doi ↗ · pubmed ↗