Role of the Pharmacist in Supporting the Use of Connected Health Devices: Example of Connected Watches
Cordélia Salomez-Ihl, Léa Liaigre, Wiceme Dala, Ambre Davat, Maud Barbado, Sébastien Chanoine, Philippe Py, Delphine Schmitt, Pascal Defaye, Pierrick Bedouch

TL;DR
This study explores how pharmacists can support patients using connected health devices like smartwatches in managing heart conditions.
Contribution
The paper identifies the potential role of pharmacists in supporting patients with connected health devices, particularly in electrophysiology.
Findings
Specialist physicians expressed a need for clinical pharmacist support in helping patients use connected watches.
Patients showed high confidence in pharmacists' ability to assist with connected health devices.
Challenges include integrating pharmacist support into pharmacy practice and organizing collaboration with hospital specialists.
Abstract
The use of Connected Medical Devices (CMDs) is growing significantly throughout the world. Although they are not dispensed in pharmacies and are not part of the pharmacy-only drug dispensing system, clinical pharmacists must be able to support patients in the use of these new technologies, which are central to their care. The aim of this study is to identify the role of the community pharmacist in supporting patients who use CMDs, using the case of connected watches in electrophysiology. Semi-structured interviews were conducted between 15 February and 20 April 2024 by a pharmacy student. The questionnaires were drafted in collaboration with a pharmacist, a cardiac electrophysiologist, a methodologist specializing in the evaluation of medical devices, and an ethical philosopher specializing in the support and acceptability of new technologies. The aim of these questionnaires was to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
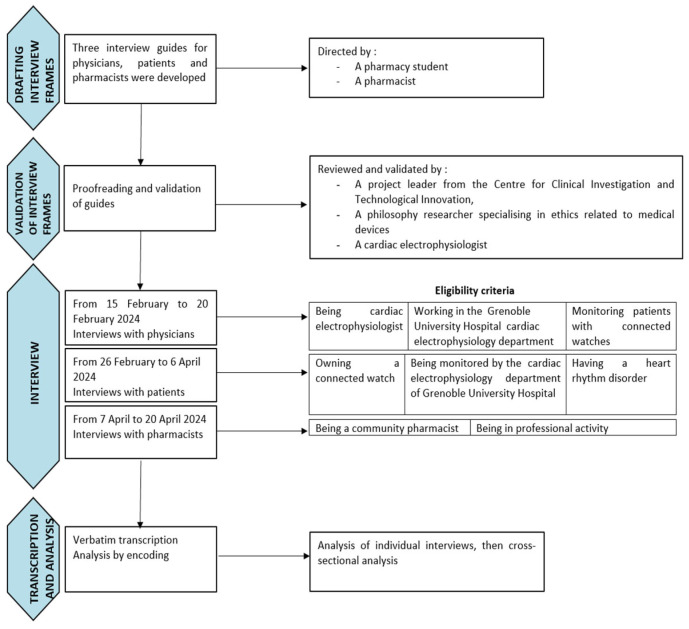 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedication Adherence and Compliance · Pharmaceutical Practices and Patient Outcomes · Electronic Health Records Systems
1. Introduction
E-health is defined by the World Health Organization as the use of Information and Communication Technologies (ICTs) for health [1]. This practice is developing significantly, as is the use of Connected Health Objects (CHOs) [2] and, more specifically, Connected Medical Devices (CMDs) [3,4,5]. Although CMDs are fully fledged healthcare products, they are not under the pharmacy-only drug dispensing system. A CMD is a CHO for which there is a medical claim. This claim may be therapeutic or diagnostic, for example. Once a CHO becomes a CMD, it must comply with the regulations in force concerning medical device (MD) status. This usage is even more prominent in a healthcare system faced with an aging population [6,7] and an increasing prevalence of chronic diseases [8,9]. Indeed, CMDs provide healthcare professionals and patients with chronic conditions the ability to remotely monitor and interpret medical data [10,11,12].
CMDs are used in numerous therapeutic areas. In the context of cardiovascular diseases, the most commonly used CMDs are aimed at diagnosing and monitoring conditions, such as connected blood pressure monitors for hypertension and smartwatches for rhythm disorders. Some CMDs are also implantable, particularly for treatment, monitoring, and remote surveillance, such as pacemakers and automatic defibrillators [13,14]. The proper use of these CMDs relies on patient support by healthcare professionals. Community pharmacists already play a key role in supporting patients with chronic diseases, notably through therapeutic education [15,16,17]. They hold an essential role in the healthcare system as they are in close proximity to patients and serve as first-line providers [18]. Therefore, their involvement in supporting patients using CMDs is crucial [19].
To ensure effective patient follow-up, community pharmacists face several challenges. Healthcare professionals need to be trained in the use of CMDs and in supporting patients who own them. Furthermore, most CMDs are not distributed in community pharmacies, and the support provided to patients using CMDs is currently not recognized as a pharmacist’s role, which explains the lack of associated remuneration. Lastly, not all CHOs are qualified as CMDs. Only objects with a medical claim can bear this designation, which comes with an EC (European Conformity) marking [20]. It is therefore important to precisely determine whether patients are using CMDs or CHOs in a landscape where an increasing number of technological innovations with various statuses coexist.
Connected watches represent a major advancement among CMDs in cardiac electrophysiology [21]. Equipped with sensors such as photoplethysmographs and sometimes integrated electrocardiograms (ECGs), they enable continuous and non-invasive monitoring of heart rate, rhythm, and other physiological parameters. These devices play a key role in the early detection of arrhythmias, particularly atrial fibrillation, thanks to advanced analysis algorithms validated by clinical studies, even in neonates [22]. In recent years, their use has revolutionized the diagnosis of intermittent atrial fibrillation, enabling the detection of events that would not previously have been seen with the usual diagnostic methods, in particular, the Holter ECG. Complementing traditional medical monitoring, smartwatches provide patients with greater autonomy and increased awareness of their health status while generating data usable by clinicians for personalized longitudinal follow-up. Their integration into rhythmological care opens promising perspectives but also raises challenges related to interoperability, data reliability, and security management.
The objective of this study was to identify the roles of community pharmacists in supporting patients using CMDs, using the example of connected watch usage in cardiac electrophysiology.
2. Materials and Methods
Semi-structured interviews were conducted with three study groups: patients, rhythmologists, and community pharmacists. Patients and physicians were interviewed between 15 February and 6 April 2024. Pharmacists were interviewed from 7 April to 20 April 2024. Figure 1 illustrates the study organization.
Initially, three interview frameworks were developed by a pharmacist and a pharmacy student (Appendixes A1 to A3). Each interview guide consisted of open-ended questions and follow-up prompts, arranged in a predefined sequence. The guides followed the same structure and were complementary. They were divided into two parts: the first aimed to collect data on the participant’s profile, while the second was organized around three themes: the device, patient support, and the role of the community pharmacist. Each section included sub-themes with an open-ended question and an associated follow-up prompt. The final section was dedicated to evaluating the interview itself, using a scale from 1 to 10 to assess factors such as the interview duration, methodology, topics covered, and the relevance of the questions.
The interview frameworks were reviewed and validated by a project coordinator from the Clinical Investigation and Technological Innovation Center, a philosophy researcher specializing in ethics related to medical devices, and a rhythmologist from the institution. The institution’s Clinical Research and Innovation Department was informed of the project and certified that this study did not require approval from an ethics committee. The questionnaires were tested and validated during an initial interview with a physician, a patient, and a pharmacist.
In line with French legislation for prospective studies using clinical data, participants were informed individually that their data could be used for research purposes. Those who objected to the use of their data were excluded from the study. Oral consent was obtained from patients, physicians, and pharmacists regarding the following points: the academic use of the data and the recording of conversations.
Participants were subsequently recruited. Interviews were offered to all rhythmologists in the team at the Grenoble Alpes University Hospital (GAUH). Patients were selected from the institution’s active cardiac electrophysiology patient database, specifically those monitored with connected watches, based on their availability and recent interactions with the medical team. The pharmacists were recruited following a random draw from an official list of retail pharmacies available at the Faculty of Pharmacy. Their views on the subject under study were not known prior to meeting them. No member of the team was able to influence the views of the pharmacists surveyed. Eligibility criteria are detailed in Figure 1.
All participants were contacted by email and interviews were conducted face to face. Interviews with physicians were conducted first, from 15 to 20 February 2024, followed by patients from 26 February to 6 April 2024, and finally pharmacists from 7 to 20 April 2024. Interviews were conducted by a community pharmacy student with prior experience in conducting interviews during shared medication review processes in community pharmacies. The interviews were supervised by a pharmacist, with the guide serving as a reference. Before each interview, participants were informed about anonymity, the time required, and complete transparency regarding the study’s objectives and the use of collected data.
Each interview was individually and fully transcribed and analyzed in an initial phase. Data were analyzed through coding, which involved identifying relevant text segments manually and assigning them appropriate codes. The codes were then grouped by theme to organize and facilitate interpretation. In the second phase, a cross-thematic analysis was performed, using tables to categorize themes and codes from interviews with physicians, patients, and pharmacists. The pharmacy student proposed a grouping, and a senior review validated the proposed thematic groupings (Appendixes B1 to B3).
3. Results
Among the six rhythmologists contacted, four responded and participated in the study. All contacted patients (n = 10) and pharmacists (n = 6) participated. The characteristics of the interviewed population are summarized in Table 1.
The interviews conducted with the physicians highlighted the following themes: the device, added value, funding, support for physicians, usage by patients, and the role of the community pharmacist.
Table 2 illustrates the key results obtained from the interviews with the physicians.
All of the physicians interviewed used smartwatches to diagnose rhythm disorders in their daily practice. According to them, the watches provided a new, effective diagnostic tool by allowing recordings during symptoms for patients who had never recorded abnormalities with other diagnostic methods, such as Holter monitors, which could be less convenient and more restrictive.
For 75% of physicians, smartwatches were also useful for monitoring rhythm changes after surgery or medication adjustments (Table 2). Physicians recommended watches compatible with patients’ phones, with Apple Watch^®^, Withings^®^, and Samsung Ultra^®^ being common choices.
One physician opposed hospital investment in such devices, citing funding and management constraints. Patients were encouraged to record symptoms at home and share data with their rhythmologists. While 75% (n = 3) reported equal patient contact regardless of smartwatch use, one physician noted more frequent contact from smartwatch users.
One physician mentioned being more frequently contacted by patients who used watches.
Regarding the role of the community pharmacist, collaboration with community pharmacists was seen as beneficial by half of the physicians, especially for patients needing technical support. Pharmacists could assist with device usage and recordings, with secure messaging preferred for communication. However, one physician highlighted limitations, including the lack of financial incentives for pharmacists, as connected watches are not sold in pharmacies or covered by billable support activities.
Interviews with patients revealed themes including watch types, benefits, costs, physician support, usage, education, psychological effects, and the role of pharmacists. Patients used Withings (Withings, Issy-les-Moulineaux, France), Apple Watch^®^ (Apple Inc., Cupertino, CA, USA), Fitbit^®^ (Google LLC, San Francisco, CA, USA), and Samsung Ultra^®^ (Samsung Electronics Co., Ltd., Gyeonggi-do, Republic of Korea), all featuring MD-certified software.
A total of 80% of patients (n = 8) reported receiving a diagnosis via their watch, with three noting difficulty in obtaining a diagnosis previously. Watches were also used for monitoring, with 40% (n = 4) sending ECG traces to physicians only for severe symptoms. Daily or weekly use depended on patient stability after procedures like atrial fibrillation ablation.
A total of 40% (n = 4) found the watches expensive, but 80% (n = 8) valued their benefits. Choices were influenced by personal research, relatives, or physician recommendations. Most patients felt autonomous, though 60% (n = 6) initially needed help from relatives. Two-thirds of patients (n = 6) found the watches easy to use after the initial period.
Psychologically, all patients found the watches reassuring, though 30% (n = 3) felt pressure from over-monitoring. A total of 90% (n = 9) trusted their pharmacist, with 30% (n = 3) discussing their watches with them. All patients believed pharmacists could help with usage issues, with 50% suggesting pharmacists offer usage support and 20% expecting training in connected watches and ECGs (Table 3).
Patients appreciated pharmacist support but noted limitations. One was wary of pharmacists interpreting rare conditions, and another highlighted the lack of financial incentives for pharmacist involvement.
Pharmacists reported encountering blood glucose meters, blood pressure monitors (33%, n = 2), and transcutaneous neurostimulation devices. In cardiology, connected blood pressure monitors were the most mentioned CMD, while smartwatches, oximeters, and connected rings were each noted once.
All pharmacists agreed that CMDs enabled regular monitoring, improved treatment adherence, and supported patient autonomy. Examples included blood pressure self-monitoring for antihypertensive adjustments, real-time glucose monitoring for pregnant women, and glucose monitoring for chronic disease management. One pharmacist had no direct experience with CMD applications (Table 4).
Half of the pharmacists noted risks of over-monitoring, while 33% (n = 2) mentioned potential excessive autonomy, reducing professional consultations. Another third highlighted issues with devices purchased outside medical circuits, including insufficient information provided at purchase.
All pharmacists saw their role as reassuring and supporting patients with CMD use, advising on device operation and data response. Half suggested implementing consultations or appointments in pharmacies, though 33% found this challenging without compensation: “The product would need to be sold in pharmacies, or there should be payment to motivate us.”
For collaboration, 80% (n = 5) preferred secure messaging with physicians, and a third supported an emergency phone line.
Among the obstacles to implementing this support, a lack of knowledge was consistently mentioned, while the lack of time was highlighted in four out of six interviews.
Regarding the solutions discussed, the main lever mentioned in all interviews was training, whether through continuing professional development, university programs, or laboratory training.
4. Discussion
To our knowledge, this is among the first qualitative studies to explore the role of community pharmacists in supporting CMDs in the field of cardiac electrophysiology. It is also the first to gather the opinions of physicians, patient users, and community pharmacists on this topic concerning a specific type of connected device. Finally, it is the first to explore the role of the pharmacist in providing therapeutic support for CMDs.
The study reveals a generally positive opinion from physicians and patients regarding the use of connected watches in cardiac electrophysiology. All physicians confirmed that they used connected watches both for diagnosis and patient follow-up. All the connected watch models used by physicians and patients in this study have an EC marking for their rhythm disorder detection software. Thus, the software of the watches used in this study are CMDs and not CHOs. Since these devices have medical purposes, this confirms their legitimacy for diagnosis and patient follow-up.
These devices are now central to the therapeutic management of patients with rhythm disorders. While the patients and physicians interviewed emphasized the ease of use of connected watches, they also confirmed that some patients, particularly the elderly, could experience difficulties using these technologically advanced devices. Indeed, Eurostat’s metadata reveals that Internet use decreases with age in most European countries. In 2024, only 61% of people aged 65–74 used the Internet regularly, compared with over 9% in younger age groups [23]. The physicians interviewed indicated that they tended to offer these watches to patients they believed could easily use the technology. To expand the use of connected watches to a larger number of patients, additional support beyond the physicians would be necessary, according to them. In this regard, the community pharmacist serves as a local support resource. Indeed, the results show that both patients and physicians trust community pharmacists to provide support for using these devices, provided they are better trained. Community pharmacists play a vital role as accessible public health resources in local communities. Several studies have investigated the expanding role of pharmacists and demonstrated their contribution to patient acceptability of healthcare interventions such as vaccination. Their clinical expertise and role in medication management make them key players in the successful adoption of AI for the benefit of patients in collaboration with other healthcare professionals [24,25].
However, training needs were highlighted by patients, physicians, and pharmacists themselves. Currently, the initial training for pharmacists is not focused on medical devices, especially connected ones. Increasing the training offer would help pharmacists improve their knowledge. For future generations of pharmacists, incorporating specialized modules on medical devices (CMDs) in their university curriculum is crucial. For currently practicing pharmacists, continuing education related to CPDs is desirable.
Other challenges were also raised by pharmacists, such as lack of time, organization, and the absence of specific compensation. Regarding the integration of this new role into pharmacy practice, implementing support programs similar to those already existing, such as consultations for pregnant women or patients on anticoagulants, could serve as a model [26]. To address the compensation issue, implementing fee-for-service payment, as is already the case for consultations with pregnant women, would recognize and value pharmacists’ additional work [27].
Finally, to successfully carry out this role, close collaboration between pharmacists and rhythmologists is essential. This collaboration must be well structured to be effective. Secure messaging, already in place, seems to be the preferred communication method for this collaboration [28]. Indeed, collaboration between pharmacists and physicians, and coordination between the city and hospital is crucial in managing patients across all medical fields.
National-level changes must therefore be implemented to address training and compensation issues. This is particularly important given that this survey reveals significant motivation among community pharmacists to take on this new role, as well as a need from physician and trust from patients.
The topic of supporting CMDs and connected health remains underdocumented. A study on the perception of connected health in France, with 1000 participants, was conducted in April 2024. Among the concerns related to the increasing use of connected health, 23% of patients expressed that tracking their health daily was anxiety-inducing, a sentiment also shared by three patients in this study [29]. Regarding community pharmacists, a study conducted with 200 pharmacists in France in 2020 explored their perception of health apps. When asked “Would you be willing to use this data in monitoring your patients?”, 46.4% of pharmacists answered positively, with 50% believing it was an effective way to improve adherence. This low proportion can be explained by the lack of information available to community pharmacists on this topic and the recent evolution of their roles [30]. Indeed, since 2020, community pharmacists have officially been able to engage in new roles such as vaccination, chronic disease management, teleconsultation, and telemedicine, including transmitting prescriptions through communication technologies.
The main limitations of this study are its monocentric nature for physicians and patients and the small number of participants. The low number of participants recruited, the lack of demographic data collection, and the fact that the patients interviewed were already ‘chronic’ users of smartwatches limit the external validity of the study. However, the diversity of the participants’ profiles contributes to the robustness of the study’s results. The patients interviewed were selected from those already using connected watches, which introduces a selection bias. It would have been interesting to speak with patients for whom this technology was not suitable. According to the clinical research unit’s opinion, patients’ ages could not be collected, due to confidentiality concerns. This parameter would have been useful, particularly to assess whether usability difficulties or differing perceptions were age-related.
The semi-structured interview framework ensured the consistency and quality of the data collected. It also allowed key themes to be addressed systematically, minimizing the roles or reformulations that could affect data comparability. The diversity of profiles that contributed to the development of the questionnaire was a definite asset in choosing and formulating the questions.
Future work should focus on implementing solutions to the various challenges previously mentioned, such as training, pharmacist compensation, integrating this new role into pharmacy practice, or setting up physician–pharmacist collaborations for this support.
While this study focuses on connected watches, it would also be relevant to examine other CMDs in different therapeutic fields, particularly in diabetology with diabetes monitoring [31], or in neurology with monitoring of sleep [32], mental health [33], or symptoms of epilepsy [34] or Parkinson’s disease [35]. A larger number of patients, physicians, and pharmacists could be surveyed through a quantitative study.
5. Conclusions
This study sought to understand the role of pharmacists in supporting the use of innovative health products outside the pharmaceutical monopoly, specifically in relation to CHOs like connected watches among physicians, patients, and community pharmacists. Interviews were conducted to characterize the use of these watches, patient support, and the expectations of each group regarding pharmacist-led support. This study highlights the crucial role of community pharmacists, whose therapeutic support and patient follow-up skills are essential in patient care. The challenges identified are pharmacist training and compensation for this service, the lack of time for in-depth consultations, and the need for clear and coordinated communication between healthcare providers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1e Health World Health Organization 2025 Available online: https://www.emro.who.int/health-topics/ehealth/(accessed on 20 November 2025)
- 2Chen S. Li M. Chen Y. Zhang Y. Li Y. Tai X. Zhang X. Exploring the evolution of e Health in disease management: A bibliometric analysis from 1999 to 2023 Digit. Health 2024102055207624128864710.1177/2055207624128864739484646 PMC 11526411 · doi ↗ · pubmed ↗
- 3Touillaud M. Fournier B. Pérol O. Delrieu L. Maire A. Belladame E. Pérol D. Perrier L. Preau M. Leroy T. Connected device and therapeutic patient education to promote physical activity among women with localised breast cancer (DISCO trial): Protocol for a multicentre 2 × 2 factorial randomised controlled trial BMJ Open 202111 e 04544810.1136/bmjopen-2020-045448 PMC 843882634518245 · doi ↗ · pubmed ↗
- 4Daibert-Nido M. Pyatova Y. Cheung K.G. Reginald A. Garcia-Giler E. Bouffet E. Markowitz S.N. Reber M. An Audiovisual 3D-Immersive Stimulation Program in Hemianopia Using a Connected Device Am. J. Case Rep.202122 e 93107910.12659/AJCR.93107934106907 PMC 8202419 · doi ↗ · pubmed ↗
- 5Rech J.S. Postel-Vinay N. Vercamer V. de Villèle P. Steichen O. User engagement with home blood pressure monitoring: A multinational cohort using real-world data collected with a connected device J. Hypertens.202543909710.1097/HJH.000000000000386139315540 PMC 11608629 · doi ↗ · pubmed ↗
- 6Amos J.G. Zheng L. Eramudugolla R. Parekh D. Huque M.H. Delbaere K. Lautenschlager N. Anstey K.J. My COACH (C Onnected Advice for Cognitive Health): A digitally delivered multidomain intervention for cognitive decline and risk of dementia in adults with mild cognitive impairment or subjective cognitive decline-study protocol for a randomised controlled trial BMJ Open 202313 e 07501510.1136/bmjopen-2023-075015 PMC 1061910137903606 · doi ↗ · pubmed ↗
- 7Simons M. Reijnders J. Janssens M. Lataster J. Jacobs N. Staying connected in old age: Associations between bonding social capital, loneliness and well-being and the value of digital media Aging Ment. Health 20232714715510.1080/13607863.2022.203694735156860 · doi ↗ · pubmed ↗
- 8Delhougne N. Monin L. Vieujean S. Van Kemseke C. Reenaers C. Warling O. Louis E. Evaluation of the adherence of patients with chronic inflammatory bowel diseases to a PRO telemonitoring using connected devices: A prospective monocentric study Acta Gastroenterol. Belg.20248745746710.51821/87.4.1344939745032 · doi ↗ · pubmed ↗