Left Atrial Myxoma as a Rare Cause of Acute Coronary Syndrome: A Case Report
Ismail Mousati, Paul Vermeersch, Nathalie Meyten

TL;DR
A rare heart tumor caused chest pain and heart attack symptoms, but normal heart arteries; echocardiography helped diagnose and guide surgery for a full recovery.
Contribution
Highlights left atrial myxoma as a rare cause of acute coronary syndrome and emphasizes the role of echocardiography in diagnosis.
Findings
Atrial myxoma can present as acute coronary syndrome with normal coronary angiography.
Echocardiography is crucial for identifying atrial myxomas.
Early surgical resection leads to excellent prognosis.
Abstract
Background and Clinical Significance: Atrial myxomas are rare, benign cardiac tumors, most commonly originating in the left atrium, with potential for serious embolic and obstructive complications. Case Presentation: We report a 67-year-old woman presenting with acute chest pain and NSTEMI whose coronary angiography results were normal. Echocardiography revealed a large, heterogeneous, stalk-attached left atrial mass, confirmed by transesophageal imaging. Surgical resection was performed two days after diagnosis, and histopathology confirmed it was an atrial myxoma. Postoperative recovery was uneventful, with reassuring follow-up echocardiography. Conclusions: Echocardiography remains an invaluable tool for the identification of atrial myxomas and early surgical excision is critical, as they have an excellent prognosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
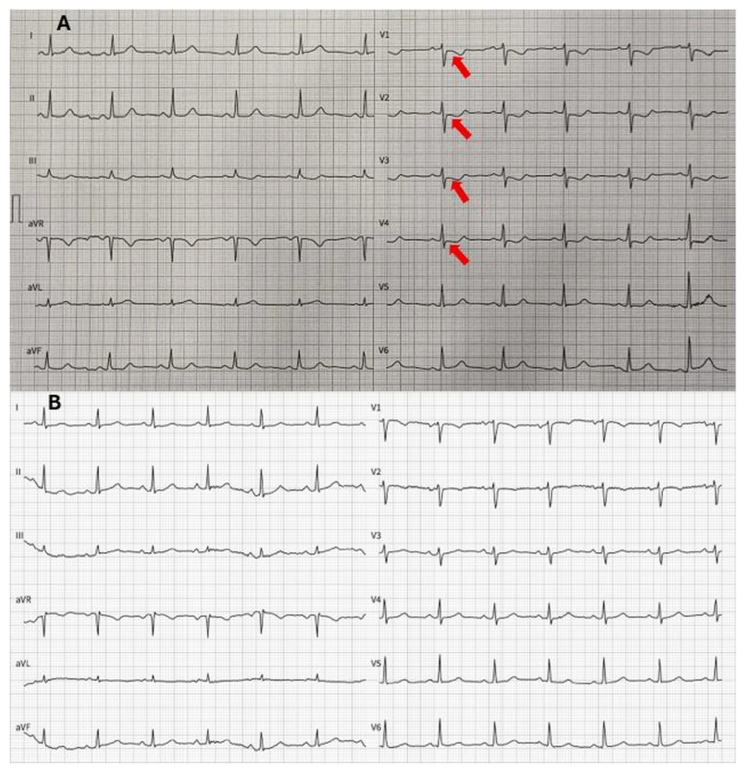 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Coronary Artery Anomalies · Vascular anomalies and interventions
1. Introduction and Clinical Significance
Cardiac myxomas are rare, benign primary cardiac tumors, yet they are of substantial clinical importance due to their potential to cause serious and life-threatening complications [1,2].
Although histologically benign, myxomas can lead to systemic embolization, intracardiac obstruction, and constitutional symptoms, resulting in diverse clinical manifestations such as ischemic stroke, syncope, heart failure, and, more rarely, acute coronary syndrome (ACS) [1,2,3].
Atrial myxomas are the most common primary cardiac tumors in adults, accounting for approximately half of all cases, and most frequently arise from the left atrium, typically originating from the interatrial septum near the fossa ovalis [3]. They most often present in middle-aged adults and show a female predominance [4]. While embolic events are well-recognized complications, coronary artery embolization leading to ACS remains an exceptionally rare presentation due to the protective anatomy of the coronary ostia and the typically larger size of embolic fragments [4].
Echocardiography plays a central role in the evaluation of suspected intracardiac masses and is the cornerstone of diagnosis for cardiac myxomas. It enables accurate assessment of tumor morphology, size, mobility, and attachment site, as well as the identification of associated hemodynamic consequences, including valvular obstruction or regurgitation [5]. Transesophageal echocardiography offers superior spatial resolution and is particularly valuable in cases where transthoracic imaging is inconclusive or when detailed anatomical characterization is required [3,4,5].
The recognition of atrial myxoma as an uncommon etiology of ACS is clinically significant, as the corresponding management strategies differ substantially from those for atherosclerotic coronary disease. Failure to identify the underlying cardiac source may result in recurrent embolic events with potentially fatal consequences. This case report highlights atrial myxoma as a rare cause of ACS and underscores the importance of comprehensive cardiac evaluation, including echocardiography, in patients presenting with myocardial infarction in the absence of traditional cardiovascular risk factors or angiographic evidence of coronary atherosclerosis.
2. Case Presentation
A 67-year-old woman presented to the emergency department with acute-onset chest pain. She had no significant medical history and no known cardiovascular risk factors. On initial evaluation, the patient was hemodynamically stable, and physical examination revealed no cardiac murmurs or signs of heart failure. The admission electrocardiogram (ECG) revealed mild anteroseptal ST-segment depression, raising concern for myocardial ischemia (Figure 1).
Initial laboratory testing showed an elevated high-sensitivity cardiac troponin level of 2.3 ng/L, which increased to 23.8 ng/L on repeat measurement one hour later, consistent with ongoing myocardial injury. Based on the clinical presentation, ECG findings, and dynamic troponin rise, a diagnosis of non-ST-segment elevation myocardial infarction (NSTEMI) was made. The patient was treated according to the standard NSTEMI protocol, and semi-urgent coronary angiography was performed to scan for coronary artery disease.
Coronary angiography revealed normal coronary arteries without evidence of atherosclerotic disease, thrombosis, or dissection (Figure 2, Videos S1–S3), prompting further investigation into an alternative etiology for the myocardial infarction. Subsequent transthoracic echocardiography revealed a mobile, protruding mass within the left atrium. It appeared to originate from the lateral wall. Moreover, there were no regional wall motion abnormalities. To further characterize the lesion, transesophageal echocardiography was performed, which revealed a heterogeneous, irregularly shaped mass measuring approximately 3 cm × 2 cm. The mass was attached to the lateral wall of the left atrium by a stalk and showed no evidence of internal vascularization, findings highly suggestive of an atrial myxoma (Figure 2, Videos S4–S8).
Given the risk of systemic embolization, including cerebral events, a cerebral computed tomography scan was conducted to exclude acute ischemic stroke; the results were reassuring. After multidisciplinary discussion, the patient was referred for semi-urgent surgical intervention. Surgical excision of the left atrial mass was performed two days after diagnosis without complications.
Histopathological examination of the resected specimen revealed fragments originating from the atrial wall, predominantly composed of muscle fibers. The tumoral mass consisted of myxoid stroma and neoplastic cells. The cells were polygonal with lightly eosinophilic cytoplasm and indistinct cell borders. The nuclei were ovoid and displayed an open chromatin pattern, with inconspicuous nucleoli. Focal inflammatory cells and hemosiderin deposition were present within the stroma. There was no evidence of necrosis or mitotic activity. These histopathological findings confirmed the diagnosis of an atrial myxoma. The postoperative course was uneventful, and the patient was extubated shortly after surgery. She was transferred from the intensive care unit to the general ward on postoperative day one. Follow-up ECG after surgery revealed normalization of the ST depression (Figure 1). Follow-up transthoracic echocardiography performed three days after surgery revealed normal cardiac function without residual intracardiac mass or valvular abnormalities.
After a total hospital stay of nine days from initial presentation, the patient was discharged in good clinical condition, and she was completely asymptomatic at the time of discharge.
3. Discussion
Primary cardiac tumors are exceedingly rare, with myxomas representing the most common type [3,5]. Advances in multimodality imaging have led to more frequent antemortem diagnosis of cardiac masses in recent years [6]. The classic symptom triad includes systemic embolic events; intracardiac obstructive manifestations such as dyspnea upon exertion, pulmonary edema, and right-sided heart failure; and constitutional symptoms, including fever, weight loss, and myalgia [5,6].
Our patient presented with a non-ST-segment elevation myocardial infarction caused by coronary artery embolization from a left atrial myxoma. ECG abnormalities, including those resembling ischemia (ST-segment deviation, both depression and elevation, and a negative T-wave), are prevalent in cardiac tumors [7]. After surgery, the ST-segment depression resolved in our patient.
Upon physical examination, a diastolic murmur over the mitral area is commonly audible due to left ventricular inflow obstruction, and a late diastolic tumor sound may be heard after the second heart sound when the mass prolapses into the left ventricle. In this case, only the late diastolic murmur was heard since there was no left ventricular inflow obstruction.
Transthoracic echocardiography is still the primary diagnostic modality, and it is an easy accessible diagnostic tool. Transesophageal echocardiography offers higher sensitivity and provides detailed information regarding the site of attachment, mobility, involvement of other cardiac chambers, and characteristic gross pathological features such as calcification, necrosis, and intratumoral hemorrhage. Multimodality imaging, including computed tomography (CT) and cardiac magnetic resonance (CMR), may further aid in assessing extracardiac extension and tissue characterization [5,8]. In this case, the absence of CMR represents a limitation, as the diagnosis of MINOCA cannot be definitively confirmed without tissue characterization. Another differential diagnosis to consider in this context is type 2 myocardial infarction. In this case, inflammatory markers were assessed and did not suggest a systemic inflammatory or infectious process. Hemodynamic parameters remained stable throughout hospitalization, and there was no evidence of severe anemia, hypoxia, or sepsis.
Surgical excision is the treatment of choice for atrial myxomas and should be performed as early as possible following diagnosis, particularly for symptomatic patients [1,2,3]. Complete resection is associated with an excellent prognosis and a low risk of recurrence [5,8].
4. Conclusions
Atrial myxomas may present with symptoms; however, they are often asymptomatic and often diagnosed incidentally during imaging. Echocardiography remains an invaluable tool for the early identification of intracardiac masses such as atrial myxomas, making it critical for preventing embolic events. The treatment of choice for atrial myxomas is surgical excision. The recommended timing of surgery is as early as possible after diagnosis, especially if the tumor is symptomatic. The prognosis is excellent after complete resection, with low recurrence rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liew D.D. Dharmaratne C. Atrial myxoma and posterior circulation stroke BMJ Case Rep.202518 e 26417210.1136/bcr-2024-26417240398905 · doi ↗ · pubmed ↗
- 2Chiarello G. Garzya M. Donateo M. Marazia S. Soldato N. Cucurachi M.R. Guaricci A.I. Colonna G. Giant left atrial myxoma causing acute ischemic stroke Future Cardiol.20231914915410.2217/fca-2022-010437140158 · doi ↗ · pubmed ↗
- 3Pinede L. Duhaut P. Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases Medicine 20018015917210.1097/00005792-200105000-0000211388092 · doi ↗ · pubmed ↗
- 4Keeling I.M. Oberwalder P. Anelli-Monti M. Schuchlenz H. Demel U. Tilz G.P. Rehak P. Rigler B. Cardiac myxomas: 24 years of experience in 49 patients Eur. J. Cardiothorac. Surg.20022297197710.1016/S 1010-7940(02)00592-412467822 · doi ↗ · pubmed ↗
- 5Dinesh Kumar U.S. Wali M. Shetty S.P. Sujay K.R. Left atrial myxoma—A tumor in transit Ann. Card Anaesth.20192243243410.4103/aca.ACA_232_1831621681 PMC 6813701 · doi ↗ · pubmed ↗
- 6Tyebally S. Chen D. Bhattacharyya S. Mughrabi A. Hussain Z. Manisty C. Westwood M. Ghosh A.K. Guha A. Cardiac Tumors: JACC Cardio Oncology State-of-the-Art Review JACC Cardio Oncol.2020229331110.1016/j.jaccao.2020.05.00934396236 PMC 8352246 · doi ↗ · pubmed ↗
- 7Angeli F. Bergamaschi L. Paolisso P. Armillotta M. Sansonetti A. Stefanizzi A. Canton L. Bodega F. Suma N. Amicone S. Spectrum of electrocardiographic abnormalities in a large cohort of cardiac masses Heart Rhythm 2025222402493890971810.1016/j.hrthm.2024.06.035 · doi ↗ · pubmed ↗
- 8Nepal S. Caicedo Murillo M.L. Ojha K. Lamichhane M. A Left Atrial Myxoma Masquerading As Acute Coronary Syndrome Cureus 202214 e 2930010.7759/cureus.2930036277524 PMC 9580039 · doi ↗ · pubmed ↗