Anaplastic Thyroid Carcinoma and High-Grade Tall Cell Papillary Thyroid Carcinoma: Case Report of a Rare Association
Catalin-Bogdan Satala, Alina-Mihaela Gurau, Gabriela Patrichi, Daniela Mihalache

TL;DR
This case report describes a rare instance where an aggressive thyroid cancer (anaplastic carcinoma) developed alongside a high-grade variant of papillary thyroid cancer.
Contribution
The paper presents a rare clinical case linking high-grade tall cell papillary thyroid carcinoma with anaplastic thyroid carcinoma.
Findings
A 67-year-old man had a thyroid tumor with both high-grade tall cell papillary and anaplastic components.
The anaplastic component showed pleomorphism, loss of thyroid markers, and high ki67 proliferation.
Multinucleated giant cells showed CD68 expression but no proliferative activity.
Abstract
Background and Clinical Significance: Anaplastic thyroid carcinoma (ATC) is a highly aggressive malignancy that may arise through dedifferentiation from pre-existing differentiated thyroid carcinomas. The tall cell subtype of papillary thyroid carcinoma (TC-PTC) represents an aggressive variant that has been involved in this tumor progression pathway. Case Presentation: We report on a rare case of ATC developed in association with a high-grade TC-PTC. A 67-year-old man presented with an enlarging anterior cervical mass. Imaging identified a suspicious nodule in the right thyroid lobe, and total thyroidectomy was performed. Histologic examination revealed a biphasic tumor composed of a nodular TC-PTC with high-grade features, contiguous with an infiltrative anaplastic carcinoma component. The anaplastic component showed marked pleomorphism, loss of thyroid differentiation markers, and an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
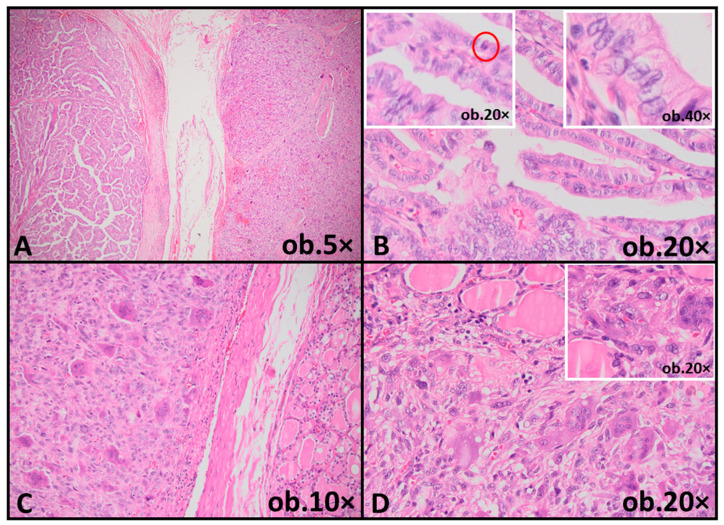 Figure 1
Figure 1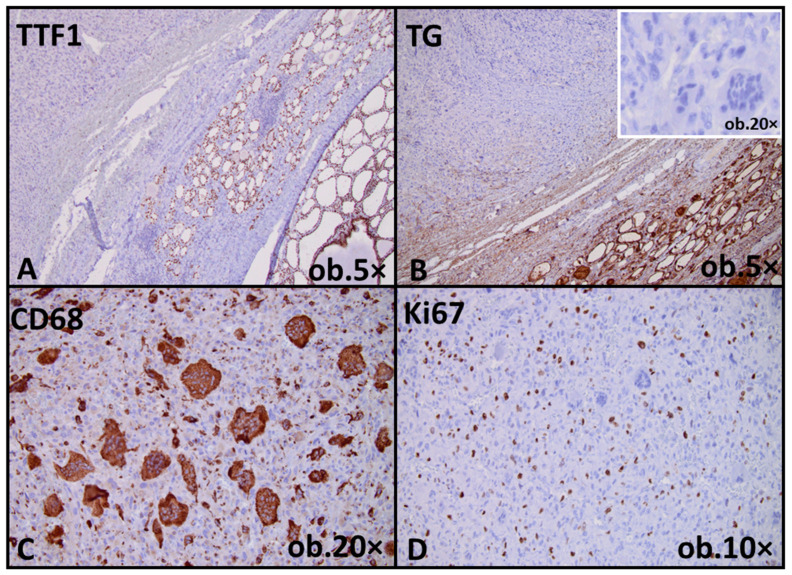 Figure 2
Figure 2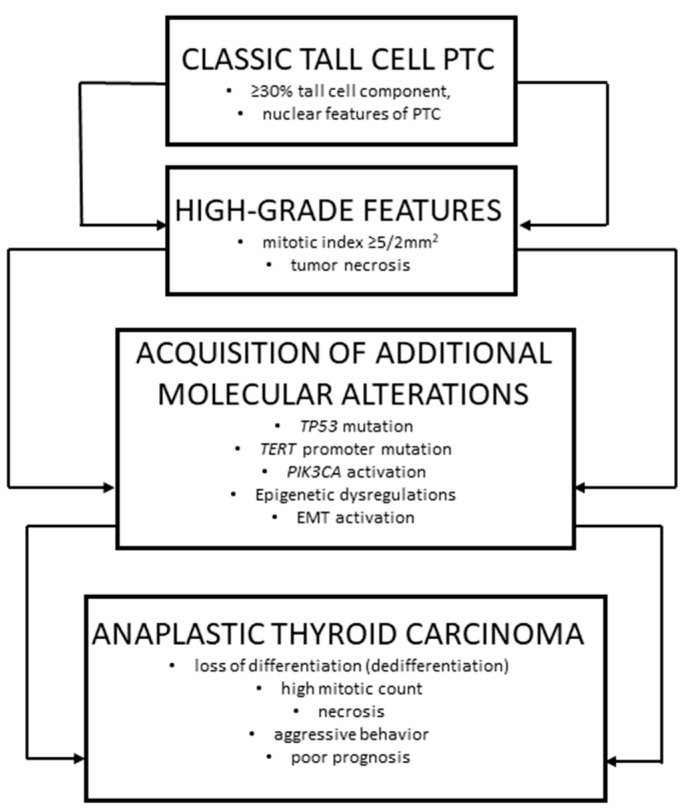 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Thyroid Disorders and Treatments · Thyroid and Parathyroid Surgery
1. Introduction and Clinical Significance
Anaplastic thyroid carcinoma (ATC) is considered one of the most aggressive malignancies, accounting for less than 2% of all thyroid cancers, but responsible for a disproportionate number of thyroid cancer-related deaths [1]. For many years, ATC was regarded as a de novo undifferentiated carcinoma; however, accumulating morphologic and molecular data have demonstrated that a substantial subset of cases develops through progressive dedifferentiation from pre-existing differentiated thyroid carcinomas [2].
Papillary thyroid carcinoma (PTC), the commonest form of differentiated thyroid cancer, encompasses multiple histologic subtypes with distinct clinicopathologic profiles [3]. Among these, the tall cell subtype (TC-PTC) has long been associated with aggressive behavior, including advanced stage at diagnosis, increased recurrence risk, and low survival rates [4]. Despite these well-recognized observations, previous classification systems did not incorporate objective histologic criteria to formally define high-grade behavior within differentiated thyroid carcinomas [3,4].
A significant conceptual shift occurred with the publication of the latest edition of the World Health Organization (WHO) Classification of Tumors of Endocrine Organs, which introduced the category of differentiated high-grade thyroid carcinoma (DHGTC) [5]. This entity is defined by increased mitotic activity and/or tumor necrosis in follicular-derived carcinomas that otherwise retain the architectural and cytologic features of differentiation, providing a framework for recognizing aggressive behavior prior to overt loss of differentiation [6,7].
The coexistence of TC-PTC with high-grade histologic features and ATC within the same lesion is exceedingly rare [4]. This case report documents such an occurrence and underscores the importance of identifying and reporting high-grade histologic features in differentiated thyroid carcinomas, in order to support accurate classification and diagnostic interpretation [8].
2. Case Presentation
2.1. Clinical History and Presentation
A 67-year-old male patient presented with a progressively enlarging anterior cervical mass, noted over several months, with no significant compressive symptoms, dysphagia, dyspnea, or dysphonia. His medical history was notable for well-controlled arterial hypertension, with no prior history of thyroid disease, radiation exposure to the head and neck region, or autoimmune disorders. The patient reported no personal history of malignancy. Family history was also unremarkable for thyroid cancer or other endocrine neoplasms. On physical examination, a firm, poorly mobile mass was palpated in the anterior cervical region, corresponding to the thyroid gland. No clinically palpable cervical lymphadenopathy was identified. No fine-needle aspiration cytology (FNAC) or fine-needle aspiration biopsy (FNAB) was performed prior to surgery, and the diagnostic evaluation proceeded directly to surgical management based on clinical and imaging findings.
2.2. Laboratory Findings
Laboratory investigations revealed thyroid function tests within normal limits, including serum thyroid-stimulating hormone (TSH), free thyroxine (fT4), and triiodothyronine (T3). Serum thyroglobulin levels were not elevated, and anti-thyroid antibodies, including anti-thyroglobulin (anti-TG) and anti-thyroid peroxidase (ATPO) antibodies, were negative. Routine hematologic and biochemical parameters were within normal reference ranges.
2.3. Imaging Studies
Thyroid ultrasound demonstrated a large, solid nodule occupying the right thyroid lobe, measuring 5.2 cm in maximum diameter. The lesion was predominantly hypoechoic, with a heterogeneous internal echotexture and irregular, poorly defined margins. Doppler examination revealed increased internal and peripheral vascularity, raising suspicion for malignancy. No suspicious lymph nodes were identified on preoperative imaging. The patient was initially evaluated in another medical center, and only the written ultrasound report was available for review, as the original imaging files were not provided to our institution.
2.4. Surgical Findings
The patient subsequently underwent total thyroidectomy. On gross examination, the right thyroid lobe contained a nodular, relatively well-demarcated tumor measuring 5.3 cm in greatest dimension, with a firm, gray-white cut surface. Adjacent to this nodular area, an ill-defined infiltrative component was identified, extending into the surrounding thyroid parenchyma of the right lobe. The tumor was confined to the thyroid gland and did not involve the surgical resection margins. The left thyroid lobe was unremarkable on gross inspection. The surgical procedure and gross examination of the thyroidectomy specimen were performed at the referring institution. The paraffin blocks were submitted to our department for microscopic evaluation and immunohistochemical profiling, in order to confirm the diagnosis and address the differential diagnostic considerations. Consequently, no macroscopic photographs were available, and the gross features were documented exclusively based on the description provided in the original pathology report.
2.5. Histopathological Findings
Microscopic examination revealed a biphasic tumor composed of two distinct but contiguous components. The nodular area corresponded to a papillary and trabecular architectural pattern lined by elongated tumor cells measuring at least three times taller than wide. These cells exhibited abundant eosinophilic cytoplasm and classic nuclear features of papillary thyroid carcinoma, including nuclear enlargement, chromatin clearing, nuclear grooves and occasional intranuclear pseudoinclusions. Increased mitotic activity (6 mitoses/2 mm^2^) was identified within this component, consistent with high-grade histologic features. In contrast, the infiltrative component displayed features of anaplastic thyroid carcinoma (ATC). This area was composed of markedly pleomorphic tumor cells arranged in solid sheets, including epithelioid and multinucleated giant cells. Brisk mitotic activity was present (Figure 1).
2.6. Immunohistochemical Findings
The immunohistochemical panel was selected to assess thyroid lineage differentiation, proliferative activity, and potential histiocytic or mesenchymal differentiation, as well as to support the differential diagnosis between differentiated high-grade carcinoma and anaplastic thyroid carcinoma. Immunohistochemical analysis demonstrated loss of thyroid differentiation markers in the anaplastic component, which was negative for thyroglobulin (TG) and thyroid transcription factor 1 (TTF1). Multinucleated giant cells showed strong CD68 immunoreactivity. The Ki67 proliferation index was elevated in the anaplastic component, reaching approximately 25%, while the CD68-positive multinucleated giant cells did not exhibit Ki67 labeling. Overall, the morphologic and immunophenotypic findings supported the diagnosis of anaplastic thyroid carcinoma arising in association with tall cell papillary thyroid carcinoma exhibiting high-grade nuclear features (Figure 2).
2.7. Clinical Outcome and Follow-Up
Following surgery, the patient was referred for further oncologic management. Subsequent treatment was performed at a medical center in another country. As the patient was lost to follow-up after leaving the country, no additional clinical, therapeutic, or survival data were available for evaluation.
3. Discussion
The tall cell subtype of papillary thyroid carcinoma (TC-PTC) was first recognized in 1976 as a morphologically distinct form of papillary thyroid carcinoma (PTC) [9]. Characterized by elongated tumor cells (at least three times taller than wide), with abundant eosinophilic cytoplasm and nuclei displaying the classical features of PTC, TC-PTC was initially identified primarily on qualitative grounds. Despite these observations, the diagnostic definition of TC-PTC remained inconsistent for decades, with variable thresholds for the proportion of tall cells required for diagnosis and without formal incorporation of histologic grading criteria [9,10]. Over time, larger cohort studies confirmed that TC-PTC represents a biologically aggressive form of differentiated thyroid carcinoma, consistently associated with worse disease-specific outcomes, compared to classic PTC [11]. These findings reinforced the concept that tall cell morphology is not merely a histologic particular aspect, but reflects an underlying aggressive tumor biology. Nevertheless, until recently, mitotic activity and tumor necrosis, features traditionally associated with poorly differentiated thyroid carcinoma (PDTC), were not systematically integrated into the classification of PTC [12].
ATC, in contrast, has long been recognized as one of the most aggressive malignancies, characterized by rapid growth, extensive local invasion, early metastasis, and an almost uniformly poor prognosis [13,14,15]. Historically, ATC was considered a de novo undifferentiated carcinoma [16]; however, accumulating morphologic and molecular evidence has demonstrated that a substantial proportion of ATCs arise through dedifferentiation from pre-existing differentiated thyroid carcinomas, including papillary carcinoma, and, notably, the tall cell subtype (Figure 3) [17,18,19,20,21].
The evolution of diagnostic criteria over past decades reflects a gradual recognition of a morphologic and biologic continuum in thyroid tumor progression. The introduction of the Turin Criteria in 2007 provided a framework for identifying PDTC based on architectural patterns and high-grade features, such as increased mitotic activity and tumor necrosis. However, this system excluded papillary carcinomas by definition, leaving a subset of differentiated tumors with high-grade features unclassified from a grading standpoint [22].
In the 4th edition of the World Health Organization (WHO) Classification of Tumors of Endocrine Organs, the tall cell subtype (formerly ‘variant’) was defined as a PTC containing at least 30% tall cells (height at least two–three times larger compared to their width) and exhibiting classic nuclear features of PTC, while ATC and PDTC were recognized as distinct entities [23]. Although this classification acknowledged the aggressive nature of TC-PTC, it did not provide a mechanism for grading differentiated carcinomas based on mitotic activity or necrosis. As a result, papillary carcinomas exhibiting this architecture continued to be classified as differentiated, potentially underestimating their clinical risk.
The 5th edition of the WHO Classification, published in 2022, addressed this limitation through the introduction of differentiated high-grade thyroid carcinoma (DHGTC). This category encompasses follicular-derived tumors, including all their histologic subtypes, that retain architectural and cytologic differentiation but exhibit objective high-grade features, defined as a mitotic count of ≥5/2 mm^2^ and/or the presence of tumor necrosis [24]. Importantly, TC-PTC can now be classified as high grade when these criteria are met, providing a formal diagnostic bridge between differentiated carcinoma and ATC (Table 1).
In current case, the papillary carcinoma component exhibited tall cell morphology accompanied by increased mitotic activity, fulfilling criteria for DHGTC.
An additional noteworthy finding in the anaplastic component of the current case was the presence of multinucleated giant cells showing strong cytoplasmic CD68 immunoreactivity, in the absence of expression of thyroid differentiation markers such as TG and TTF1. Importantly, these CD68-positive giant cells did not exhibit Ki67 labeling, suggesting that they do not represent the actively proliferating tumor population. Similar findings have been described in ATC with giant cell morphology, in which multinucleated tumor cells are considered terminally differentiated or degenerative elements rather than the active clonal proliferative compartment [25,26,27]. Aberrant CD68 expression in this setting is widely regarded as a manifestation of extreme dedifferentiation and phenotypic switch, rather than evidence of true histiocytic differentiation [26]. The absence of proliferative activity within giant cell population, together with the elevated Ki67 index in the remaining anaplastic component, supports a model in which tumor progression is driven by highly proliferative undifferentiated cells, while multinucleated CD68-positive cells reflect end-stage cellular transformation. This immunophenotypic profile further emphasizes the profound loss of thyroid-specific differentiation associated with anaplastic transformation [25,26].
From a diagnostic standpoint, the main differential diagnosis considered in this case was poorly differentiated thyroid carcinoma (PDTC), particularly given the presence of solid growth areas and increased mitotic activity. However, several histologic and immunophenotypic features argued against this diagnosis, including the marked cellular pleomorphism, the prominent multinucleated giant cell component, brisk and atypical mitotic figures, an infiltrative growth pattern, and the complete loss of thyroid differentiation markers, such as thyroglobulin and TTF1. Taken together, these findings are more consistent with an anaplastic thyroid carcinoma, in accordance with the diagnostic criteria outlined in the WHO 2022 classification [24].
An additional diagnostic challenge in the present case was the distinction between differentiated high-grade thyroid carcinoma and early anaplastic transformation, particularly in the context of intratumoral heterogeneity. In this case, the tall cell papillary carcinoma component retained the architectural and nuclear features of differentiation, despite the presence of increased mitotic activity, fulfilling the criteria for differentiated high-grade thyroid carcinoma. In contrast, the adjacent component showed abrupt morphologic transition to marked cytologic pleomorphism, loss of follicular architecture, infiltrative growth, and complete loss of thyroid differentiation markers, supporting a diagnosis of overt anaplastic thyroid carcinoma rather than early or incipient dedifferentiation.
Molecular studies provide further insights into the pathways that may drive this progression. TC-PTC is frequently associated with BRAF V600E mutation, which activates the MAPK signaling pathway and contributes to tumor proliferation and aggressiveness [28,29]. As tumor progress, additional genetic alterations, including TP53 mutations, TERT promoter mutations, and PIK3CA activation, are frequently acquired, conferring genomic instability and facilitating dedifferentiation [30,31,32]. These alterations are particularly prevalent in ATC and are thought to represent key molecular drivers of progression from differentiated to dedifferentiated tumors. Although these molecular alterations are well documented in the progression from differentiated to anaplastic thyroid carcinoma, molecular genetic testing was not performed in the present case, as the specimen was referred to our institution exclusively for histopathological second opinion and immunohistochemical evaluation.
Beyond genetic changes, epigenetic dysregulation and alterations in the tumor microenvironment may further contribute to tumor evolution [33]. Epigenetic modifications affecting gene expression, dysregulation of cell-cycle checkpoints and activation of epithelial–mesenchymal transition (EMT) have all been involved in the loss of differentiation and acquisition of highly invasive behavior [34,35]. Tumor necrosis, a defining feature of high-grade disease, may also reflect hypoxia and ischemia within the tumor microenvironment, conditions that promote selection of more aggressive tumor clones. From a diagnostic standpoint, the distinction between DHGTC and early anaplastic transformation can be challenging, particularly in limited biopsy material. Tumors may display striking intratumor heterogeneity, with well-differentiated areas co-existing alongside regions of high-grade morphology or overt anaplasia [36]. This underscores the importance of thorough sampling and careful histologic evaluation of thyroidectomy specimens, especially in tumor exhibiting tall cell features.
Clinically, recognition of high-grade features in TC-PTC has important implications for patient management. DHGTC may demonstrate reduced responsiveness to radioactive iodine therapy and may require more aggressive surgical management, closer surveillance, or consideration of alternative therapeutic strategies [37]. Clear reporting of mitotic activity and tumor necrosis facilitates communication between pathologists and clinicians and allows for accurate risk stratification. From a clinical perspective, the recognition of differentiated high-grade thyroid carcinoma has important prognostic and therapeutic implications. Tumors classified as high-grade may exhibit more aggressive behavior, reduced responsiveness to radioactive iodine therapy, and an increased risk of progression compared to conventional differentiated carcinomas. Therefore, accurate identification and reporting of high-grade features may influence clinical decision-making, postoperative surveillance strategies, and consideration of alternative therapeutic approaches.
It is important to emphasize that the concept of a stepwise progression from differentiated to anaplastic thyroid carcinoma remains a theoretical and clinicopathologic construct rather than a universally established biological sequence. The recently introduced category of differentiated high-grade thyroid carcinoma in the WHO 2022 [24] classification provides a diagnostic framework for recognizing aggressive histologic features within otherwise differentiated tumors, but its clinicobiological significance is still being elucidated. In this context, the present case does not aim to establish causality or progression, but rather to illustrate morphologic patterns that are consistent with concepts currently discussed in the literature.
4. Conclusions
This case illustrates the rare but significant occurrence of ATC arising in association with a pre-existing TC-PTC with high-grade features. It highlights the importance of recognizing and reporting high-grade histologic features in TC-PTC, as these findings are relevant for accurate classification and diagnostic interpretation within the framework of the WHO 5th edition. The integration of morphologic grading systems, as formalized in the WHO 5th edition, with molecular insights provides a more comprehensive framework for understanding thyroid tumor progression and guiding clinical decision-making. This case report has several limitations that should be acknowledged. These include the unavailability of original ultrasound images and macroscopic photographs of the surgical specimen, as the patient was initially evaluated and surgically treated at another institution, and only descriptive clinical and pathology reports were accessible. In addition, molecular genetic testing was not performed, as the specimen was referred to our institution exclusively for histopathological second opinion and immunohistochemical evaluation. Furthermore, long-term clinical follow-up data were not available, as the patient continued postoperative management in another country and was subsequently lost to follow-up.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Juhlin C.C. Mete O. Baloch Z.W. The 2022 WHO classification of thyroid tumors: Novel concepts in nomenclature and grading Endocr. Relat. Cancer 202230 e 22029310.1530/ERC-22-029336445235 · doi ↗ · pubmed ↗
- 2Baloch Z.W. Asa S.L. Barletta J.A. Ghossein R.A. Juhlin C.C. Jung C.K. Li Volsi V.A. Papotti M.G. Sobrinho-Simões M. Tallini G. Overview of the 2022 WHO Classification of Thyroid Neoplasms Endocr. Pathol.202233276310.1007/s 12022-022-09707-335288841 · doi ↗ · pubmed ↗
- 3Lebrun L. Salmon I. Pathology and new insights in thyroid neoplasms in the 2022 WHO classification Curr. Opin. Oncol.202436132110.1097/CCO.000000000000101237975316 PMC 10715705 · doi ↗ · pubmed ↗
- 4Ghossein R. Katabi N. Dogan S. Shaha A.R. Tuttle R.M. Fagin J.A. Ganly I. Xu B. Papillary thyroid carcinoma tall cell subtype (PTC-TC) and high-grade differentiated thyroid carcinoma tall cell phenotype (HGDTC-TC) have different clinical behaviour: A retrospective study of 1456 patients Histopathology 2024841130113810.1111/his.1515738528726 PMC 11827125 · doi ↗ · pubmed ↗
- 5Jung C.K. Bychkov A. Kakudo K. Update from the 2022 World Health Organization Classification of Thyroid Tumors: A Standardized Diagnostic Approach Endocrinol. Metab.20223770371810.3803/En M.2022.155336193717 PMC 9633223 · doi ↗ · pubmed ↗
- 6Basolo F. Macerola E. Poma A.M. Torregrossa L. The 5th edition of WHO classification of tumors of endocrine organs: Changes in the diagnosis of follicular-derived thyroid carcinoma Endocrine 20238047047610.1007/s 12020-023-03336-436964880 PMC 10199828 · doi ↗ · pubmed ↗
- 7Poma A.M. Macerola E. Ghossein R.A. Tallini G. Basolo F. Prevalence of Differentiated High-Grade Thyroid Carcinoma Among Well-Differentiated Tumors: A Systematic Review and Meta-Analysis Thyroid 20243431432310.1089/thy.2023.035038115626 PMC 10951568 · doi ↗ · pubmed ↗
- 8Goswami P. Patel T. Dave R. Singh G. Singh A. Kalonia T. WHO 2022 updates on follicular cell and c-cell derived thyroid neoplasm J. Med. Life 202417152310.25122/jml-2023-027038737660 PMC 11080517 · doi ↗ · pubmed ↗