Successful Remission of Refractory Oral Ulcers Treated with Low-Dose Thalidomide and Colchicine: A Case Report
Shun-Yu Kan, Yu-Kai Sung, Chia-Lu Hsu, Kuo-Chou Chiu

TL;DR
A patient with persistent oral ulcers showed full remission after treatment with low-dose thalidomide and colchicine when other therapies failed.
Contribution
Demonstrates successful remission of refractory oral ulcers using a novel combination of low-dose thalidomide and colchicine.
Findings
Low-dose thalidomide and colchicine achieved complete remission of refractory oral ulcers.
The combination therapy was effective when conventional treatments, including corticosteroids, failed.
Remission was sustained for over six months without recurrence.
Abstract
Background and Clinical Significance: Oral ulcers are a common disease for dental practitioners. The policy of treating oral ulcers includes removing etiology and medication. Standard management of oral ulcers includes elimination of etiologic factors and pharmacologic therapy. Topical corticosteroids are the most commonly used medicine for oral ulcers. Exclude possible etiologies related to ulcers; refractory ulcers need systemic evaluation and precise medication use to improve patients’ quality and satisfaction. Case Presentation: We present a case of refractory oral ulcers resistant to multiple conventional treatments, which were found to be ineffective. These ulcers significantly impact patient quality of life. We prescribed a series of oral ulcer treatments following the removal of cause factors, such as rounding the teeth and making a soft occlusal bite plate to reduce traumatic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
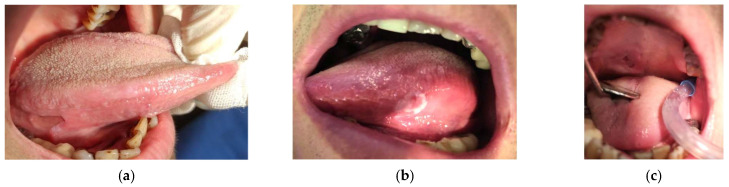 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3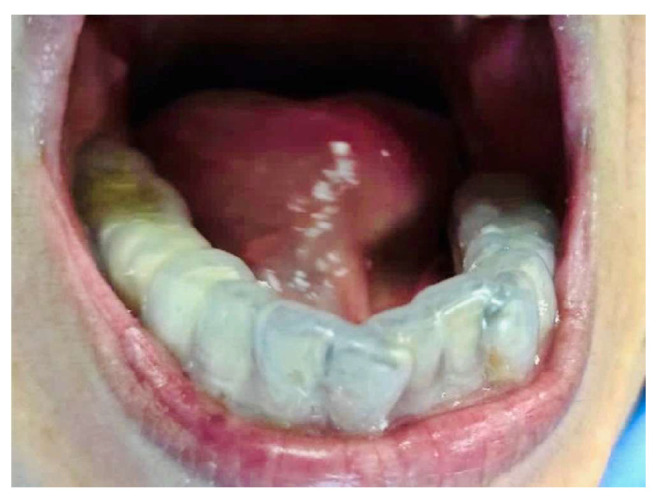 Figure 4
Figure 4 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7 Figure 8
Figure 8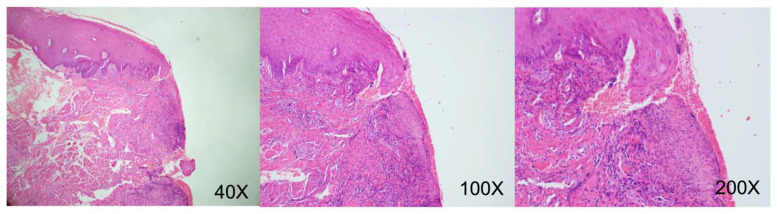 Figure 9
Figure 9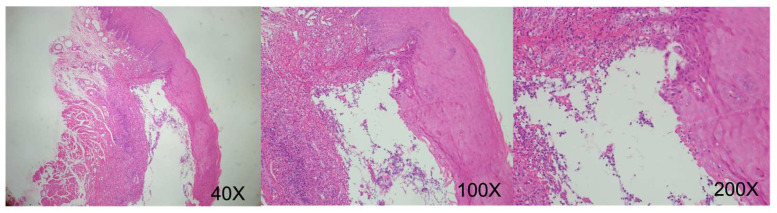 Figure 10
Figure 10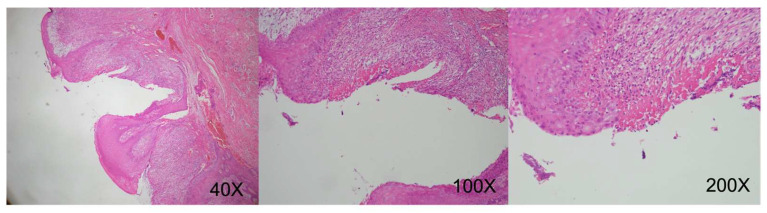 Figure 11
Figure 11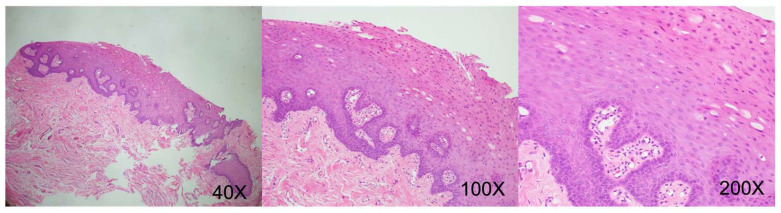 Figure 12
Figure 12- —Taichung Armed Forces Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOral Health Pathology and Treatment · Oral health in cancer treatment · Oral and Craniofacial Lesions
1. Introduction and Clinical Significance
Oral ulcers, a common condition in oral mucosal pathology, include recurrent aphthous stomatitis (RAS) and traumatic ulcers as the primary types. While most ulcers heal naturally, refractory cases significantly impact patient comfort and life quality. Standard management involves removing related cause factors and prescribing topical or systemic corticosteroids. In challenging cases, subcutaneous corticosteroid injections have been recommended [1,2]. However, anecdotal studies have suggested that dapsone, pentoxifylline, colchicine, and thalidomide may have a role in refractory cases [3,4,5]. These studies often involved single-dose medication for refractory ulcers. Accurate diagnosis and eliminating potential cause factors are crucial initial steps in managing oral ulcers. Biopsy of prolonged unhealed oral ulcers is advised to rule out possible malignancies. Here, we report a case of refractory oral ulcers managed with combination therapy using low-dose thalidomide and colchicine, aiming to provide clinical insight in a refractory setting.
2. Case Presentation
A 66-year-old female presented to our clinic with persistent painful oral ulcerations lasting more than two weeks. Her medical history included Sjögren’s syndrome, systemic lupus erythematosus (SLE), rheumatoid arthritis, Parkinson’s disease, and impaired liver function. The patient denied smoking, alcohol consumption, or betel nut chewing. Given the presence of multiple systemic autoimmune diseases, these conditions were considered potential confounding factors in both disease severity and treatment response. Clinical examination revealed three distinct ulcerations located on the right lateral tongue (2.5 × 1 cm, Figure 1a), left lateral tongue (1.5 × 1 cm, Figure 1b), and soft palate (1 × 1 cm, Figure 1c). Sharp tooth structures over lower bilateral molar areas with Xerostomia were also noted (Figure 2). Generalized gingival swelling with plaque accumulation was also observed (Figure 3). Baseline pain intensity was retrospectively assessed using a visual analog scale (VAS, 0–10) and was estimated to be 8, reflecting severe pain interfering with oral intake and speech.
2.1. Initial Management and Etiologic Control
Initially, bilateral tongue ulcers were attributed to mechanical trauma from sharp teeth combined with Xerostomia. In contrast, the palatal ulcer was considered to be associated with her underlying autoimmune condition. Our treatment plan was comprehensive, beginning with the meticulous task of smoothing sharp tooth edges and the precise application of dexamethasone (1 mg/g) oral base topically. However, after two weeks, the ulcers demonstrated minimal improvement. Considering Parkinson’s disease-related tongue movements and persistent Xerostomia, we made a soft occlusal bite splint and prescribed oral balance gel for mucosal lubrication (Figure 4). Concurrently, we prescribed topical dexamethasone (1 mg/g) oral base, benzydamine oral spray (3 mg/mL), and tramadol (375 mg twice daily) for symptomatic relief. Routine scaling was performed regularly, yet the ulcers persisted with limited improvement after four weeks. VAS scores during this period remained high (VAS 7–8), with no meaningful reduction in ulcer size.
2.2. Histopathological Evaluation and Systemic Therapy
An excisional biopsy from the left lateral tongue was conducted at the six-week follow-up to rule out malignancy. The pathological report shows epithelial hyperplasia with no malignant transformation. Subsequent management included systemic prednisolone (initially 20 mg/day for 1 week, then reduced to 10 mg/day) with nystatin mouth rinse (100,000 I.U./c.c, thrice daily) to manage pseudomembranous candidiasis (Figure 5). Steroid resistance was clinically defined as the persistence of ulcer size and pain despite adequate courses of topical and systemic corticosteroids. The patient had a history of intermittent systemic corticosteroid exposure related to her autoimmune diseases, although she was not receiving continuous long-term steroid therapy at presentation. Despite the initial treatment not yielding the expected results, the patient’s resilience was evident as the ulcer on the right soft palate showed minimal improvement, measuring 2.3 × 2.3 cm (Figure 6). Even after the addition of thalidomide (50 mg/day) combined with prednisolone (10 mg/day), the ulcer on the right soft palate showed minimal improvement, measuring 2.3 × 2.3 cm after one-week follow-up (Figure 6). With VAS remaining approximately 7. The short duration of monotherapy was not intended to establish definitive drug inefficacy but rather served as an exploratory assessment of early clinical responsiveness and tolerability in the setting of severe symptoms and multiple systemic comorbidities.
2.3. Escalation and Combination Therapy
Colchicine (0.5 mg twice daily) was introduced to replace thalidomide temporarily, and the prednisolone dose was raised to 15 mg the following week; however, ulcer progression was limited, with persistent pain and stable lesion size (VAS ~6–7). A combination treatment regimen involving thalidomide (50 mg/day), colchicine (1.5 mg/day), and low-dose prednisolone (2.5 mg/day) was subsequently initiated. Within two weeks, notable pain reduction was observed (VAS decreased from 7 to approximately 3), accompanied by progressive reduction in ulcer size (Figure 7 and Figure 8). During brief discontinuation of either thalidomide or colchicine due to clinical considerations, ulcer pain and mucosal breakdown recurred within several days, with VAS increasing to approximately 6, and improvement was again observed after resumption of combination therapy. Optimizing the regimen with thalidomide (50 mg/day), colchicine (1.5 mg/day), and prednisolone (2.5 mg/day) achieved sustained ulcer control for the following two weeks. Prednisolone was subsequently discontinued, while thalidomide and colchicine were continued. No ulcer recurrence or pain exacerbation (VAS ≤1) was observed during the subsequent six weeks. A final maintenance regimen combining thalidomide (50 mg/day) with colchicine (1.5 mg/day) resulted in complete remission, which was maintained throughout a six-month follow-up period without recurrence or discomfort.
2.4. Histopathological Follow-Up
Biopsies were performed at four follow-up periods to exclude malignant transformation during the disease course.
These repeated biopsies were performed for surveillance rather than to guide therapeutic escalation.
August 2019 (right lateral tongue): Squamous epithelial hyperplasia with low-grade dysplasia, focal ulceration. (CK-negative, increased Ki-67 proliferative activity) (Figure 9).December 2019 (left lateral tongue): Ulceration with granulation tissue formation. Deep submucosal inflammatory cell infiltration. (CK-negative) (Figure 10).October 2020 (oral mucosa): Squamous epithelial hyperplasia, focal low-grade dysplasia, chronic inflammation, submucosal congestion. (CK-negative) (Figure 11).April 2024 (right tongue): Mild squamous epithelial hyperplasia, parakeratosis, mild chronic inflammation. (CK-negative and basal Ki-67 proliferative activity) (Figure 12).
3. Discussion
Recurrent oral ulcers are classified into minor, major, and herpetiform categories based on size, number, shape, location, healing duration, and the presence or absence of scarring [1,2]. Depending on severity and recurrence frequency, they may also be differentiated into simple or complex aphthosis. Simple aphthosis typically involves smaller lesions associated with mild pain and infrequent recurrences. In contrast, complex aphthosis presents with larger, multiple, and overlapping lesions accompanied by severe pain, prolonged healing periods, and lesions often extending beyond the oral cavity [2]. The extensive and persistent ulcers observed in our patient met the severe and complex aphthosis criteria. The pathogenesis of recurrent oral ulcers remains incompletely understood but likely involves T-cell-mediated mucosal immune dysregulation, exacerbated by cytokine and neuropeptide activity. Although potential etiologies include infections, nutritional deficiencies, and systemic diseases such as Crohn’s disease or celiac disease, these are rarely the primary contributors to most cases [1]. Diagnosis, a process that relies on clinical evaluation and patient history, provides a reassuring framework, supplemented by biopsies when necessary to exclude malignancies and systemic conditions such as Crohn’s disease, systemic lupus erythematosus, Behçet’s disease, pemphigus, pemphigoid, cyclic neutropenia, or squamous cell carcinoma [1,2,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25].
Corticosteroids, notably prednisolone, are frequently prescribed for severe presentations, are initiated at 20–40 mg/day for approximately one week, and are gradually tapered down as the symptoms improve [1,7]. Although corticosteroids effectively promote acute healing, they do not reliably prevent recurrence and pose risks of systemic side effects, limiting their long-term usage [7]. For refractory cases, alternative pharmacological treatments, including thalidomide, colchicine, dapsone, pentoxifylline, and biological agents such as adalimumab, are recommended. However, most of the reports were single-dose use with no combination therapy [1,2,4,5,26,27,28]. Existing reports primarily describe monotherapy approaches, and evidence regarding combination strategies remains limited.
Thalidomide is considered an anti-angiogenic agent in tumor therapy and an immunomodulatory drug by its pharmacological properties of reducing tumor necrosis factor-alpha (TNF-α) levels to eliminate host inflammatory reactions and tissue damage [7]. Due to the anti-angiogenic properties in the fetuses, the teratogenicity side effects should be considered and avoided in pregnant women or women at puberty periods. Colchicine is an anti-inflammatory drug that disrupts microtubule assembly and reduces neutrophil activity to reduce host inflammatory reactions. Dapsone modulates neutrophil chemotaxis and lysosomal function and should not be prescribed in patients with glucose-6-phosphate dehydrogenase (G6PD) deficiencies or sulfa drug allergies. Pentoxifylline, a drug with the potential to enhance microcirculation and suppress TNF-α production, is an area of ongoing research due to its unclear mechanism [4]. Biological agents, such as adalimumab, have shown efficacy but with higher costs, and there is no oral prescription but only IV injections [29].
Clinical studies indicate that thalidomide at 100 mg/day substantially decreases ulcer frequency and severity; however, recurrence commonly occurs after discontinuation. Low maintenance doses (approximately 50 mg/day) result in promising remission rates but necessitate ongoing safety evaluations. Published clinical trials indicated that thalidomide is more effective in treating oral ulcers than dapsone, colchicine, and pentoxifylline [30,31,32]. Most clinical trials use a single dose of medicine to treat refractory ulcers. Reports evaluating combination immunomodulatory therapy remain scarce, and comparative evidence is limited. The present case provides an additional clinical observation of combination therapy using thalidomide and colchicine in a patient with refractory disease and limited response to corticosteroids. Initiation at lower doses with close monitoring may be considered to mitigate potential adverse effects; however, such strategies require further evaluation.
Clinically validated alternative treatments with broader applications include thalidomide, colchicine, dapsone, and pentoxifylline [4,5]. Revuz et al. demonstrated that nearly half of patients treated with thalidomide (100 mg/day) achieved complete remission within two months; however, ulcer recurrence averaged 19 days post discontinuation [31]. Hello et al. reported that maintenance therapy with low-dose thalidomide (median dose 50 mg/day) effectively maintains remission, yet the risk of recurrence after cessation remains notable, highlighting the need for continuous monitoring [32]. An open clinical trial by Mimura et al. further corroborated the superior effectiveness and tolerability of thalidomide compared with other treatments [5].
This report has several limitations. First, it describes a single patient without a controlled comparison, limiting causal inference. Second, outcome measures such as pain intensity and ulcer size were retrospectively estimated rather than prospectively standardized. Third, the presence of multiple systemic autoimmune diseases and prior corticosteroid exposure represents potential confounding factors. Fourth, although remission was maintained for six months, long-term safety and generalizability of combination therapy remain uncertain. Therefore, the findings should be interpreted cautiously and viewed as hypothesis-generating rather than practice-changing.
4. Conclusions
Although combination therapy with low-dose thalidomide and colchicine is not routine therapy with oral ulcers, the cost of combination therapy is ten times that compared with traditional corticosteroid therapy in Taiwan. The teratogenic side effects of using thalidomide should be considered. When considering combination therapy, individual patient factors—including systemic comorbidities, financial burden, and tolerance of potential adverse effects—should be carefully weighed. Overall, this case should be interpreted as hypothesis-generating and does not establish clinical recommendations or generalizable treatment efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Regezi J.A. Sciubba J. Jordan R.C. Oral Pathology: Clinical Pathologic Correlations Elsevier Health Sciences Amsterdam, The Netherlands 2016
- 2Neville B.W. Damm D.D. Allen C.M. Chi A.C. Oral and Maxillofacial Pathology Elsevier Health Sciences Amsterdam, The Netherlands 2015
- 3Alli B.Y. Erinoso O.A. Olawuyi A.B. Effect of sodium lauryl sulfate on recurrent aphthous stomatitis: A systematic review J Oral Pathol. Med.20194835836410.1111/jop.1284530839136 · doi ↗ · pubmed ↗
- 4Tarakji B. Gazal G. Al-Maweri S.A. Azzeghaiby S.N. Alaizari N. Guideline for the diagnosis and treatment of recurrent aphthous stomatitis for dental practitioners J. Int. Oral Health 2015774 PMC 444124526028911 · pubmed ↗
- 5Mimura M.A.M. Hirota S.K. Sugaya N.N. Sanches J.A.Jr. Migliari D.A. Systemic treatment in severe cases of recurrent aphthous stomatitis: An open trial Clinics 20096419319810.1590/S 1807-5932200900030000819330244 PMC 2666466 · doi ↗ · pubmed ↗
- 6Azevêdo A.B. Sobral A.P. Faria C.A. Sousa J.S. Silva W.R. Silveira M.M. Assessment of the prevalence of Behcet’s disease in recurrent aphthous ulceration worldwide: A systematic review Med. Oral Patol. Oral Cir. Bucal 202530 e 484e 49010.4317/medoral.2702340121688 PMC 12221144 · doi ↗ · pubmed ↗
- 7Shashy R.G. Ridley M.B. Aphthous ulcers: A difficult clinical entity Am. J. Otolaryngol.20002138939310.1053/ajot.2000.1887211115523 · doi ↗ · pubmed ↗
- 8Stavropoulos F. Katz J. Guelmann M. Bimstein E. Oral ulcerations as a sign of Crohn’s disease in a pediatric patient: A case report Pediatr. Dent.20042635535815344631 · pubmed ↗