A Rare Case of Reversible Pulmonary Hypertension Phenotype in a Child with Scurvy: Aetiologies Insights
Mattia Pasquinucci, Luisa Bonsembiante, Sofia Mezzalira, Martina Locallo, Davide Meneghesso

TL;DR
A child with scurvy showed reversible pulmonary hypertension, highlighting the link between vitamin C deficiency and vascular changes.
Contribution
This case reveals a novel connection between scurvy and reversible pulmonary arterial hypertension through metabolic dysregulation.
Findings
Vitamin C and iron deficiencies may trigger a pseudohypoxic state leading to pulmonary hypertension.
Pulmonary pressures in scurvy-related PAH can normalize rapidly with nutritional supplementation.
Metabolic dysregulation involving ascorbic acid, iron, and folate disrupts vascular homeostasis.
Abstract
Background and Clinical Significance: Scurvy, caused by chronic vitamin C deficiency, is re-emerging in Western countries, particularly among pediatric patients with highly selective diets. While its musculoskeletal and mucocutaneous manifestations are well-known, its association with pulmonary arterial hypertension (PAH) is rare and poorly understood. Ascorbic acid and iron are essential cofactors for prolyl hydroxylases (PHD), which regulate Hypoxia-Inducible Factors. Their combined deficiency may trigger a “pseudohypoxic” state, leading to pulmonary vascular remodeling and vasoconstriction. Case Presentation: A 30-month-old female presented with a one-month history of limping, lower limb pain, and gingival hypertrophy. Dietary history revealed an almost exclusive cow’s milk-based intake. Physical examination showed diffuse petechiae, pallor, and right knee edema. Laboratory findings…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1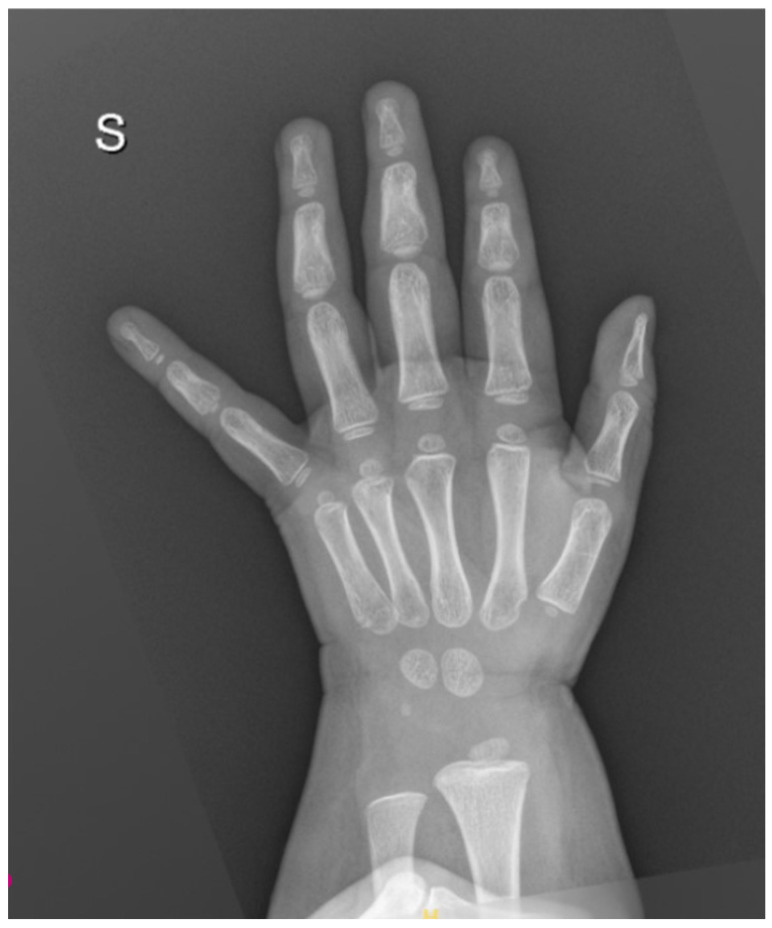 Figure 2
Figure 2 Figure 3
Figure 3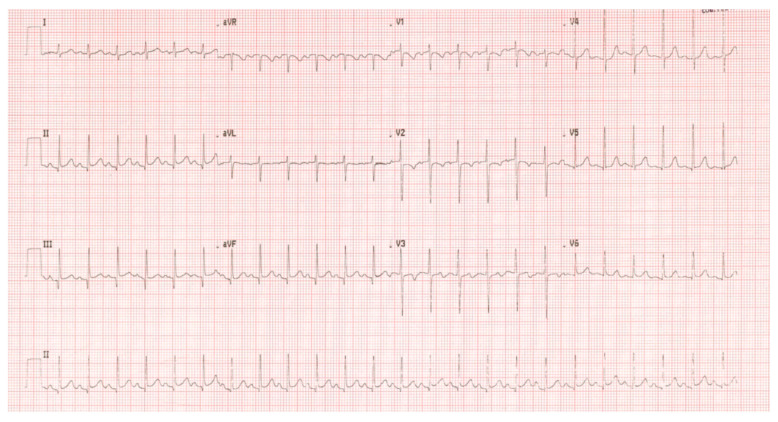 Figure 4
Figure 4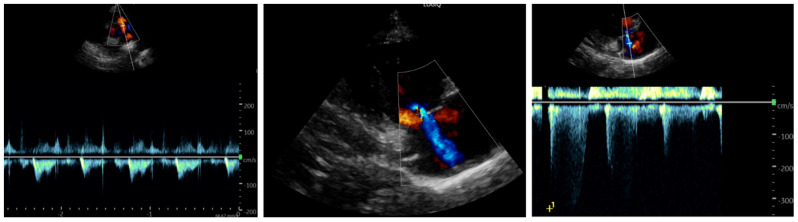 Figure 5
Figure 5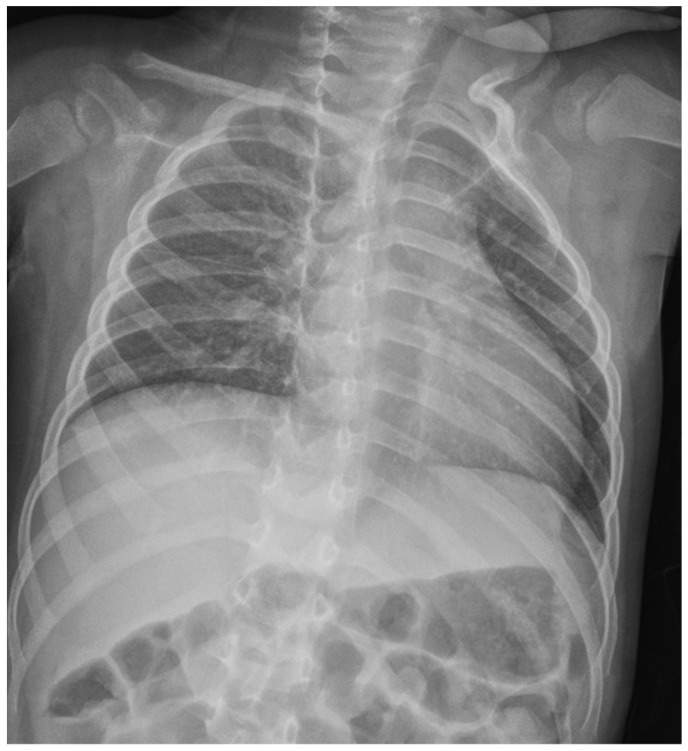 Figure 6
Figure 6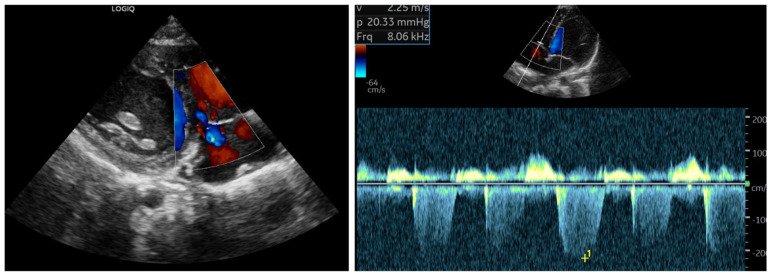 Figure 7
Figure 7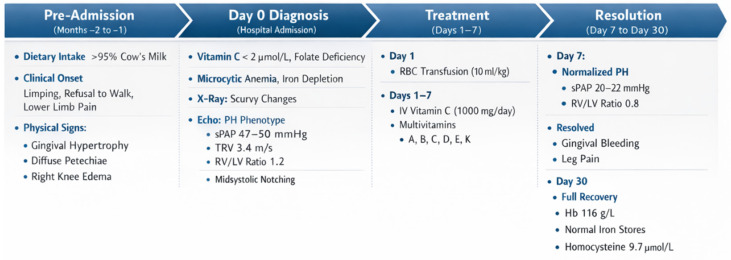 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin C and Antioxidants Research · Vitamin K Research Studies · Alcoholism and Thiamine Deficiency
1. Introduction and Clinical Significance
Scurvy is a disease of historical significance, traditionally known as “the disease of sailors.” It results from chronic ascorbic acid deficiency and remains relatively frequent, though underdiagnosed, in developing countries where access to a balanced diet is limited. However, its incidence has been increasing in Western countries in recent years [1]. While it can affect adults, the pediatric population is generally more susceptible. It typically presents with cutaneous, mucosal, and musculoskeletal signs; early diagnostic markers include gingival hypertrophy with bleeding, limping or refusal to walk, and lower limb pain [2]. In cases of malabsorption, global malnutrition, or highly selective diets, scurvy is often associated with other micronutrient deficiencies [3]. Historically, there was no established link between scurvy and cardiovascular manifestations.
Clinical Significance: Recently, however, increasing attention has been paid to this correlation, and associated pulmonary arterial hypertension (PAH) has been rarely reported [4,5,6,7]. Nevertheless, its true incidence in patients with scurvy and its exact etiology remains incompletely understood.
2. Case Presentation
A 30-month-old female presented to our Emergency Department following several visits to other centers for a one-month history of monoarticular swelling, limping, and lower limb pain. The patient had sustained a fall approximately two weeks prior to the onset of symptoms. Clinical evaluation revealed periarticular edema and rubor of the right knee, a maculopapular rash on the same limb, diffuse petechiae, haemorrhagic gingival hypertrophy, and pallor (Figure 1).
Vital signs showed tachycardia and a systemic blood pressure of 90/55 mmHg (below normal limits). Dietary history disclosed a selective cow’s milk-based intake, accounting for over 95% of the child’s caloric intake.
Laboratory findings revealed severe hypochromic microcytic anemia without thrombocytopenia but with severe iron deficiency, along with mild coagulation abnormalities (increased Antithrombin III). Renal and hepatic functions were within normal limits, while electrolytes showed mild hyponatremia (Na^+^ 132 mmol/L). The metabolic–nutritional profile indicated global malnutrition with low triglycerides and HDL cholesterol and reduced prealbumin; blood glucose was normal. The initial differential diagnosis included malignant lymphoproliferative disease, which was reasonably excluded via peripheral blood smear; the latter instead showed neutrophil hypersegmentation (consistent with malnutrition/folate deficiency). Further biochemical analysis revealed low folate levels and increased homocysteine. High levels of D-dimer, copper, and vitamin B12 were also noted, initially interpreted as markers of systemic hyperinflammation (Table 1).
The absence of significant lactic acidosis rendered a concomitant Thiamine deficiency less likely. Celiac disease was ruled out. Vitamin C was undetectable, confirming the diagnosis of scurvy. X-rays of the wrist showed slightly delayed bone age (Figure 2), while knee X-rays revealed typical skeletal changes pathognomonic for scurvy (Figure 3).
Given the severity of the malnutrition, a cardiological evaluation was performed to rule out malnutrition-related cardiomyopathy before initiating high-volume fluids. Electrocardiography (ECG) showed diffuse repolarization abnormalities (Figure 4).
Echocardiography, performed under midazolam sedation due to psychomotor agitation (but with stable hemodynamics), showed findings suggestive of PAH, including midsystolic notching of the pulmonary artery flow, moderate tricuspid regurgitation, a measurable tricuspid regurgitant jet >2.8 m/s with an estimated systolic pulmonary artery pressure (sPAP) of approximately 47–50 mmHg, assuming tricuspid regurgitation velocity 42–45 mmHg and right atrial pressure 5 mmHg, and slight end-diastolic flattening of the interventricular septum (Figure 5). The left heart appeared hyperdynamic. Despite these findings, the patient remained hemodynamically stable with normal resting oxygen saturation.
Chest X-ray was performed to screen for pleuroparenchymal involvement or gross cardiomegaly (Figure 6). The exam revealed clear lung fields with normal vascular markings and a cardiac silhouette within the normal limits for age. These findings were instrumental in excluding primary lung diseases (Group 3 PH) and pulmonary venous congestion, thereby supporting the hypothesis of a functional, pre-capillary pulmonary hypertension phenotype.
Suspecting mixed malnutrition (deficiencies in vitamin C, vitamin K, and B-complex vitamins), intravenous vitamin C and multivitamin supplementation were initiated (Table 2).
Follow-up ECG and echocardiography demonstrated complete normalization of pulmonary pressures after one week (Figure 7), which was confirmed one month after discharge along with the resolution of laboratory abnormalities.
The rapid reversibility of the PAH phenotype was documented through sequential echocardiographic assessments. A comprehensive comparison of the hemodynamic and functional parameters from admission to the 7th day of treatment is provided in Table 3.
For a comprehensive overview of the clinical sequence—spanning from dietary habits and symptom onset to the resolution of the PH phenotype following treatment—please refer to the detailed timeline provided in Appendix A (Figure A1).
3. Discussion
PAH in scurvy has been rarely described, and it has been defined as pre-capillary (PVRi > 2 WU) in rare cases when cardiac cateterism was performed [8]. Table 4 summarizes the most frequent causes of PAH and their diagnostic tools that we used for differential diagnosis in the absence of a right heart cateterism.
Its pathophysiology in the context of scurvy is likely to be recognized as a multifactorial “perfect storm,” where acute vitamin C depletion acts as the final trigger on a pre-existing substrate of profound metabolic and nutritional derangement [9].
As established in previous reports, the most compelling mechanism involves the impairment of the endothelial–vascular homeostasis. Ascorbic acid and ferrous iron (Fe^2+^) are essential cofactors for prolyl hydroxylases (PHD), enzymes responsible for the degradation of Hypoxia-Inducible Factors (HIFs) [10,11]. In our patient, the simultaneous absence of vitamin C and severe iron deficiency (suggested by ferritin of 22 mcg/L and transferrin saturation of 5%) likely led to the pathological stabilization of HIF-1α and HIF-2α [12]. This “pseudohypoxia” state promotes pulmonary vasoconstriction and vascular remodeling, mimicking the effects of chronic altitude exposure despite normal oxygen saturation.
Building upon this established framework, we propose a further layer of complexity involving a disrupted iron-trafficking system. Although the C-reactive protein (CRP) was only mildly elevated (1.5 mg/dL), the scurvy-induced state of massive oxidative stress may have stimulated hepcidin production through non-canonical, ROS-dependent pathways. Elevated hepcidin levels, potentially reinforced by iron sequestration via lactoferrin in hypertrophic gingival tissues, would degrade ferroportin, leading to functional iron deficiency. In this framework, the observed elevation in serum copper (in the absence of significant systemic inflammation) becomes highly significant. It may reflect a compensatory, albeit futile, up-regulation of ceruloplasmin (a copper-dependent ferroxidase) in a desperate attempt to mobilize intracellular iron stores [13]. In our hypothesis, this “metabolic lock” would further starve the pulmonary vasculature of the iron necessary for PHD function, reinforcing the hypertensive cycle.
A different explanation may lie beyond systemic inflammation. The observed hypercupremia may be interpreted through the lens of impaired copper trafficking. As suggested by Harris et al., ascorbic acid is essential for labilizing copper bound to ceruloplasmin and facilitating its trans-membrane transport. In a state of profound scurvy, the absence of vitamin C may lead to a paradoxical accumulation of copper in the vascular compartment due to impaired cellular uptake, potentially exacerbating the functional iron deficiency and the subsequent HIF-mediated pulmonary vasoconstriction [14].
The finding of homocysteine levels twice the upper limit of normal serves as a crucial metabolic marker of this global derangement. While primarily interpreted as a signature of folate deficiency (consistent with the high RDW of 30% and neutrophil hypersegmentation), we suggest that hyperhomocysteinemia may have acted as a direct vascular toxin [15]. By impairing nitric oxide bioavailability and inducing oxidative stress, it likely narrowed the vasodilatory reserve of the pulmonary bed, making it more susceptible to the hemodynamic stress of an anemia-induced high-output state.
4. Conclusions
The rapid normalization of pulmonary pressures within one week of multivitamin supplementation, well before the correction of anemia or iron stores, strongly suggests that the recovery of ascorbate-dependent nitric oxide production and the resetting of the PHD/HIF axis were the primary drivers of resolution. This case highlights that PAH phenotype in scurvy might be considered not as a fixed structural disease but as a reversible metabolic disruption of the pulmonary vascular tone. Clinicians should consider scurvy in the differential diagnosis of unexplained echo-suspected PAH in children with selective diets, emphasizing that the cure lies not in vasodilators, but in targeted nutritional restoration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Di Nora A. Finocchiaro M.C. Pizzo F. Gian Luca T. Cucuzza M.E. Di Stefano A. Spampinato S. Marino S. Ruggieri M. Pavone P. Scurvy, a not obsolete disorder: Clinical report in eight young children and literature review Open Med.2025202024108610.1515/med-2024-108641041521 PMC 12487768 · doi ↗ · pubmed ↗
- 2Ayyad M. Tran L. Ansari S. Levy D. Matassa D. Forgotten Deficiency: A Case Series Highlighting Atypical Presentations of Scurvy in the 21st Century Case Rep. Med.20252025211890710.1155/carm/211890740589921 PMC 12208746 · doi ↗ · pubmed ↗
- 3Toscano F. Zirilli G. Foti Randazzese S. Carlino M. Gallizzi R. Wasniewska M. Valenzise M. Scurvy, all the faces you can see: Our experience and review of the literature Ital. J. Pediatr.20255115910.1186/s 13052-025-02014-740437614 PMC 12121052 · doi ↗ · pubmed ↗
- 4HemiläH. de Man A.M.E. Vitamin C deficiency can lead to pulmonary hypertension: A systematic review of case reports BMC Pulm. Med.20242414010.1186/s 12890-024-02941-x 38504249 PMC 10949735 · doi ↗ · pubmed ↗
- 5Berra G. Genecand L. Juillet A. Deux J.F. Prada P. Müller H. Roffi M. Beghetti M. Reversible pulmonary hypertension in a patient diagnosed with scurvy BMJ Case Rep.202518 e 26614310.1136/bcr-2025-26614341360493 PMC 12683649 · doi ↗ · pubmed ↗
- 6Silberkasten M. San Martin E. Cuello J.V. Britto M.V. Andrés M.E. Pulmonary hypertension secondary to vitamin C deficiency: A case report Arch. Argent. Pediatr.2025123 e 202510643(In English)10.5546/aap.2025-10643.eng 40526584 · doi ↗ · pubmed ↗
- 7Flanagan L.S. Sadek A. Oliveros E. Vitamin C Deficiency as a Readily Reversible Cause of Pulmonary Hypertension JACC Case Rep.20253010342410.1016/j.jaccas.2025.10342440447367 PMC 12235451 · doi ↗ · pubmed ↗
- 8Satawiriya M. Khongphatthanayothin A. Limsuwan A. Reversible severe pulmonary hypertension related to scurvy in children BMC Cardiovasc. Disord.2024242410.1186/s 12872-023-03629-638172747 PMC 10765653 · doi ↗ · pubmed ↗