Planetary Health Diet Adherence and Medication Use in Older Adults with Chronic Kidney Disease: A Cross-Sectional Study
Luca Soraci, Guido Gembillo, Maria Elsa Gambuzza, Edlin Villalta Savedra, Chiara Chinigò, Elvira Filicetti, Mara Volpentesta, Giada Ida Greco, Domenico Santoro, Andrea Corsonello

TL;DR
A plant-based diet called the Planetary Health Diet is linked to fewer medications in older adults with kidney disease.
Contribution
This study is the first to show that higher adherence to the Planetary Health Diet is associated with reduced medication burden in older adults with chronic kidney disease.
Findings
Each 10-point increase in PHDI score was associated with 3% fewer medications.
Higher PHDI scores were linked to lower odds of proton pump inhibitor and nonsteroidal anti-inflammatory drug use.
Participants in the highest PHDI tertile had 8% fewer medications compared to those in the lowest tertile.
Abstract
Background/Objectives: Chronic kidney disease (CKD) in older adults is frequently accompanied by substantial medication burden, increasing risks of adverse drug events and poor adherence. The Planetary Health Diet Index (PHDI), emphasizing plant-based foods and sustainable dietary patterns, may improve cardiometabolic health and reduce medication requirements. This study examined the association between PHD adherence as measured by the PHDI and medication burden among older adults with CKD. Methods: We analyzed cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) 2003–2018 cycles. Older individuals aged ≥ 65 years with CKD (estimated glomerular filtration rate < 60 mL/min/1.73 m2 or albumin-to-creatinine ratio > 30 mg/g) at the baseline visit were included (n = 3161). PHDI scores (0–150) were calculated from two consecutive 24 h dietary recalls.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
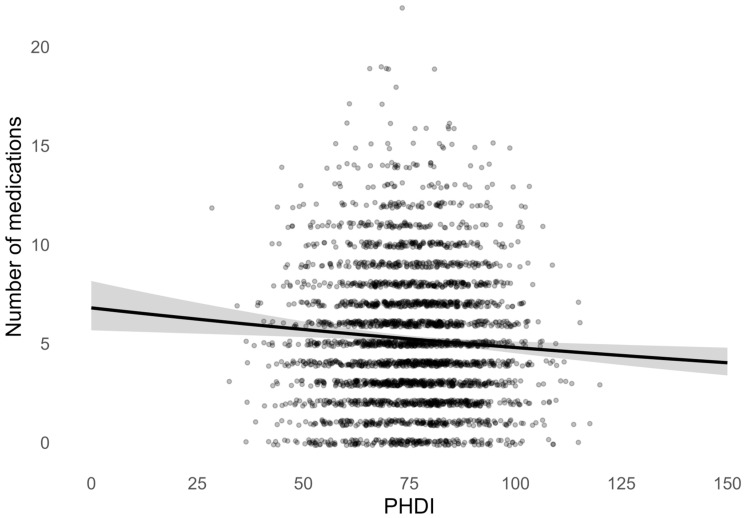 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNutritional Studies and Diet · Agriculture Sustainability and Environmental Impact · Sodium Intake and Health
1. Introduction
Chronic kidney disease (CKD) affects approximately 15% of adults worldwide [1], with prevalence exceeding 40% among individuals aged 70 years and older [2]. CKD patients experience extremely high rates of comorbid conditions, including hypertension, diabetes, anemia, and cardiovascular diseases, which substantially increase mortality and complicate treatment [3,4,5]. A multidisciplinary approach is needed to manage overlapping pharmacologic risks [3]. Older adults with CKD commonly experience polypharmacy, defined as the concurrent use of five or more medications, with some patients requiring 10 or more daily prescriptions [6,7]. This medication burden is associated with increased risks of adverse drug reactions, drug–drug interactions, falls, cognitive impairment, poor medication adherence, and greater healthcare costs [8,9]. The medication classes commonly prescribed to CKD patients include antihypertensives (particularly renin-angiotensin-aldosterone system inhibitors), diuretics, phosphate binders, erythropoiesis-stimulating agents, iron supplements, vitamin D analogs, sodium bicarbonate for metabolic acidosis, statins, antiplatelet agents, and hypoglycemic medications [3,10]. Each additional medication increases the complexity of disease management and the potential for treatment-related complications, particularly in the geriatric population where altered pharmacokinetics and pharmacodynamics further complicate therapeutic decision-making [11,12].
Dietary interventions represent a potentially modifiable factor that could improve health outcomes and reduce medication requirements in CKD. Traditional renal diets have emphasized restriction of protein, sodium, potassium, and phosphorus; however, these restrictive approaches may contribute to malnutrition and poor dietary quality in older adults [13]. The Planetary Health Diet (PHD), developed by the EAT-Lancet Commission on Food, Planet, and Health, proposes an alternative framework emphasizing whole grains, fruits, vegetables, legumes, nuts, and unsaturated oils, with moderate amounts of fish and poultry and minimal red meat and processed foods [14]. The Planetary Health Diet Index (PHDI) quantifies adherence to PHD principles across 15 food components, with scores ranging from 0 to 150 [15,16]. Higher PHDI scores reflect greater consumption of health-promoting plant foods and lower intake of animal-based and processed products. Recent epidemiological studies have demonstrated associations between higher PHDI adherence and reduced risks of type 2 diabetes, cardiovascular disease, cancer, and all-cause mortality in general populations [17,18,19]. The mechanisms underlying these benefits likely involve improved glycemic control, blood pressure regulation, lipid profiles, anti-inflammatory effects, antioxidant capacity, and favorable modulation of the gut microbiome [20,21].
In the context of CKD, the PHDI may offer specific advantages [22]. In prospective cohort data, higher adherence to plant-based diet was associated with slower eGFR decline and decreased incidence of CKD [23,24]. More recently, PHDI-focused analyses in middle-aged/older adults have reported that greater adherence to a planetary health diet score is associated with lower CKD risk, supporting the kidney relevance of the PHDI construct [25]. Several mechanisms may explain these effects: high dietary fiber intake promotes production of short-chain fatty acids by gut bacteria, which may reduce generation of uremic toxins [26]. The alkaline ash of plant foods may help ameliorate metabolic acidosis, a recognized driver of tubulointerstitial injury and CKD progression; in a randomized trial, treatment with base-producing fruits and vegetables improved acid–base status and was associated with less eGFR decline compared with usual care, with additional cardiometabolic benefits [27]. Additionally, the cardiovascular and metabolic benefits of plant-predominant diets may translate into better blood pressure and glycemic control, both of which are important for slowing the progression of CKD [24].
Despite the theoretical rationale and emerging evidence for plant-based dietary patterns in CKD management, no studies have specifically examined the relationship between PHD adherence and medication burden in older adults with CKD. Given the unique vulnerabilities of this population to both CKD progression and medication-related adverse events, understanding whether dietary quality influences pharmacological complexity could inform clinical practice and public health recommendations.
Therefore, the objective of this study was to examine the association between PHD adherence and medication burden among older adults with CKD using nationally representative data from the National Health and Nutrition Examination Survey (NHANES) 2003–2018. We hypothesized that higher PHDI scores would be associated with lower medication counts, independent of traditional confounding factors. Secondary objectives included examining whether higher PHDI scores were associated with decreased prescription of specific medication classes commonly prescribed in CKD as well as potentially nephrotoxic medications, such as proton pump inhibitors (PPIs) and nonsteroidal anti-inflammatory drugs (NSAIDs).
2. Materials and Methods
2.1. Study Population and Design
This cross-sectional study utilized data from eight consecutive cycles of the National Health and Nutrition Examination Survey (NHANES): 2003–2018. NHANES is a nationally representative survey of the non-institutionalized civilian U.S. population conducted by the National Center for Health Statistics (NCHS) of the Centers for Disease Control and Prevention (CDC) [28]. The survey employs a complex, stratified, multistage probability sampling design to ensure national representation. All NHANES protocols were approved by the NCHS Research Ethics Review Board, and all participants provided written informed consent.
Starting from 61,872 participants undergoing two consecutive 24 h dietary recall visits, we selected 3181 participants aged 65 years and older and with a diagnosis of CKD at the baseline visit. After removing 20 individuals with extreme caloric intake (having a total daily energy < 500 Kcal or ≥8000 Kcal), we obtained a final analytic sample of 3161 individuals to be included in the study.
2.2. PHDI
Dietary intake was assessed using two non-consecutive 24 h dietary recalls, collected by trained interviewers using the United States Department of Agriculture (USDA) Automated Multiple-Pass Method. Day 1 data were collected in person at the Mobile Examination Center; day 2 data were collected via telephone interviews 3–10 days later, according to methodology presented elsewhere [29]. The average of the two days was used to estimate daily intake of foods and nutrients and total energy intake (TEI) in Kcal/day. Dietary data were then linked to the Food Patterns Equivalents Database, which categorizes foods into the 37 USDA Food Pattern Components, using a food composition table [30]. Food patterns equivalents were then converted in grams/day according to standardized conversion units. Adherence to the PHD was then assessed using the PHDI scoring system proposed by the EAT-Lancet Commission [16] and further adapted to the US population [31]. The 15 PHDI components and criteria used to calculate PHDI are shown in Supplementary Table S1. In brief, each of the 15 food components was assigned a score ranging from 0 (lowest adherence) to 10 (highest adherence) based on recommended intake ranges. For example, a value of 10 was awarded when component intake met or exceeded the EAT-Lancet recommended minimum (for adequacy components) or stayed below the upper threshold (for moderation components). Partial points were proportionally assigned between minimum and maximum thresholds. The points of each of the 15 food components were then summed to obtain an overall PHDI score, ranging from 0 to 150, and representing adherence to the diet, with higher scores indicating greater alignment with the planetary health dietary model.
2.3. CKD Definition
Kidney function was assessed using two standard biomarkers: the estimated glomerular filtration rate (eGFR) and the urinary albumin-to-creatinine ratio (ACR). eGFR was calculated by using the race-free CKD-EPI 2021 equation [32], while ACR was determined from spot urine samples by measuring urinary albumin and creatinine concentrations. CKD was defined as the presence of eGFR < 60 mL/min/1.73 m^2^ or ACR > 30 mg/g [32]
2.4. Study Covariates
Demographic variables included age, sex, race/ethnicity, and poverty income ratio as a measure of socioeconomic status. Poverty income ratio represents the ratio of family income to the federal poverty threshold, with values < 1.0 indicating income below the poverty level [33].
Lifestyle factors included smoking status and alcohol consumption. Smoking status was assessed using standardized NHANES questionnaire items. Participants were classified as current smokers if they reported having smoked at least 100 cigarettes in their lifetime and answered either “every day” or “some days” to the question “Do you now smoke cigarettes?”. Participants who reported smoking at least 100 cigarettes in their lifetime, but who were not currently smoking, were classified as former smokers, while those who reported smoking fewer than 100 cigarettes in their lifetime were classified as never smokers. For the purpose of this analysis, current and former smokers were combined into a single smoking category. Alcohol consumption was defined as consuming ≥12 alcoholic drinks in the past year.
Comorbid conditions were assessed through self-report of physician diagnosis and included hypertension, diabetes mellitus, cardiovascular disease (congestive heart failure or coronary artery disease), stroke, cancer (any malignancy), and chronic obstructive pulmonary disease (COPD). Diabetes mellitus diagnosis was supplemented with use of laboratory glycated hemoglobin (HbA1c) ≥ 6.5%.
Other laboratory measurements included fasting glucose, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), C-reactive protein (CRP), and uric acid. All laboratory analyses were performed at standardized centers following NHANES protocols.
2.5. Medication Assessment
Prescription medication data were collected during the household interview, as previously reported [34]. Participants were asked to show the interviewer all prescription medications taken in the past 30 days. Interviewers recorded the name of each medication from the container. Medication names were matched to their therapeutic class using the Lexicon Plus database, a proprietary database of Cerner Multum, Inc. Total medication count was defined as the number of unique prescription medications currently used. Polypharmacy was defined as the concurrent use of five or more prescription medications. Specific medication classes of interest included angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARBs), beta-blockers, calcium channel blockers (CCBs), statins, glucose-lowering medications, urate-lowering medications, antiplatelet medications, and phosphate binders. Potentially nephrotoxic medications assessed included PPIs and NSAIDs.
2.6. Statistical Analysis
All analyses incorporated NHANES survey weights to account for the complex survey design, including stratification, clustering, and non-response, ensuring nationally representative estimates. Because dietary exposure was derived from two 24 h dietary recalls, all analyses were conducted using the NHANES dietary two-day sample weights, which are specifically designed for participants with complete two-day dietary recall data. As the present analysis combined eight consecutive NHANES cycles (2003–2018), the original two-day sample weights were divided by eight, in accordance with National Center for Health Statistics analytic guidelines, to obtain appropriate nationally representative estimates across the pooled survey period.
Survey-weighted descriptive statistics were calculated for baseline characteristics overall and stratified by PHDI tertiles. PHDI tertiles were defined according to the weighted distribution of the score, with T1 representing the lowest adherence, T2 intermediate adherence, and T3 the highest adherence to the PHD. Continuous variables were presented as means with standard deviations (SD) or medians with interquartile ranges (IQR), as appropriate. Categorical variables were expressed as frequencies and weighted percentages. Comparisons across PHDI tertiles were conducted using survey-weighted one-way ANOVA for normally distributed continuous variables, survey-weighted Kruskal–Wallis test for non-normally distributed continuous variables, and Rao-Scott adjusted chi-square test for categorical variables.
The association between PHDI and medication burden was examined using survey-weighted Poisson regression models with robust variance estimation, given the count nature of medication number with overdispersion. PHDI was analyzed both as a continuous variable (per 10-point increase) and categorically (tertiles). Two sequential models were constructed: Model A adjusted for age, sex, race/ethnicity, and poverty income ratio; Model B additionally adjusted for smoking status, alcohol consumption, hypertension, diabetes mellitus, cardiovascular disease, stroke, COPD, cancer, eGFR, and ACR.
Survey-weighted multivariable logistic regression models were used to assess associations between PHDI and use of specific medication classes, including PPIs and NSAIDs. Models were adjusted for the same covariates as Model B in the Poisson regression analyses, with additional mutual adjustment for PPI use when examining NSAIDs, and vice versa.
All statistical tests were two-sided, with p < 0.05 considered statistically significant. Analyses were performed using R software version 4.3.0 (R Foundation for Statistical Computing, Vienna, Austria), incorporating the survey package for complex survey design adjustments.
3. Results
3.1. Baseline Characteristics of the Study Population
The final analytical sample included 3161 older adults with CKD, representative of the U.S. population. Baseline characteristics of the study population, overall and stratified by PHDI tertiles, are shown in Table 1.
Overall, the mean (SD) age was 75.0 (5.5) years, and 56.4% of participants were women. The majority were white (80.3%), and the mean (SD) poverty income ratio was 2.7 (1.5). The mean (SD) PHDI score was 76.6 (12.9). Across increasing PHDI tertiles, defined as T1 (lowest PHDI adherence), T2 (intermediate PHDI adherence), and T3 (highest PHDI adherence), participants differed significantly in several sociodemographic and lifestyle characteristics. Individuals in the highest PHDI score tertile were slightly older and were more likely to be female compared with those in the lowest tertile (65.6% vs. 46.3%, p < 0.001). Higher PHDI adherence was also associated with a more favorable socio-economic condition, represented by higher poverty income ratios (p < 0.001) and a lower prevalence of smoking (45.2% in T3 vs. 61.4% in T1, p < 0.001). Alcohol consumption did not differ significantly across tertiles (p = 0.126).
With respect to comorbidities, the prevalence of hypertension, diabetes, cardiovascular disease, stroke, and cancer was high in this older CKD population but did not differ significantly across PHDI tertiles (all p > 0.05). Mean (SD) eGFR was 58.3 (18.7) mL/min/1.73 m^2^ and was comparable across tertiles (p = 0.160). Similarly, median ACR did not vary significantly by PHDI adherence (p = 0.769).
Several metabolic and biochemical markers differed across tertiles. Higher PHDI adherence was associated with lower mean fasting glucose levels (p = 0.017) and lower serum uric acid concentrations (p = 0.004). Participants in the highest PHDI tertile also exhibited a more favorable lipid profile, with significantly higher HDL-cholesterol levels compared with those in the lowest tertile (57.1 vs. 51.0 mg/dL, p < 0.001). Mean HbA1c showed a borderline decreasing trend across tertiles (p = 0.058), while LDL-cholesterol and C-reactive protein concentrations did not differ significantly by PHDI tertile.
Table 2 summarizes medication burden and patterns of medication use in the overall study population and across PHDI tertiles.
Overall, participants used a mean (SD) of 5.2 (3.3) medications, and 53.9% met criteria for polypharmacy. The average number of medications differed significantly across PHDI tertiles, with participants in the highest PHDI tertile using fewer medications compared with those in the lowest tertile (4.9 vs. 5.4 medications; p = 0.025). The prevalence of polypharmacy decreased across increasing PHDI tertiles, although this trend was not statistically significant.
With respect to cardiovascular medications, the use of ACEi, ARBs, beta blockers, CCBs, and statins was common but did not vary significantly by PHDI tertile (all p > 0.05). Similarly, no significant differences across tertiles were observed for the use of glucose-lowering agents, urate-lowering agents, antiplatelet agents, or phosphate binders, the latter being infrequently used in the overall population.
In contrast, the use of selected medication classes differed across PHDI tertiles. In particular, PPI use was significantly lower among participants in the highest PHDI tertile compared with those in the lower tertiles (16.7% in T3 vs. 21.5% in T1; p = 0.007). Similarly, the prevalence of NSAID use decreased across increasing PHDI tertiles, with the lowest use observed in the highest tertile (5.2% in T3 vs. 8.5% in T1; p = 0.003).
3.2. Association Between PHDI Score and Number of Medications
As shown in Figure 1, higher PHDI scores were associated with a lower medication burden. The survey-weighted unadjusted Poisson regression curve demonstrates a gradual inverse relationship between PHDI score and the expected number of medications, with the predicted mean number of drugs decreasing steadily across the observed range of PHDI values. This association was evident despite substantial inter-individual variability in medication counts, particularly at lower PHDI scores. Each 10-point increase in PHDI score (PHDI-10) was associated with a relative 4% reduction in the number of medications, supporting a dose–response relationship between diet quality and medication burden (RR, 95% CI: 0.96, 0.94–0.99, p = 0.004).
These preliminary findings were confirmed in survey-weighted multivariate Poisson regression models (Table 3).
When PHDI was modeled as a continuous variable (per 10-point increase), PHDI-10 was associated with a 3% lower number of medications in both models. This association was statistically significant in the minimally adjusted model (Model A: RR = 0.97, 95% CI 0.94–0.99; p = 0.002) and remained significant after further adjustment for additional covariates in Model B (RR = 0.97, 95% CI 0.96–0.99; p = 0.011), indicating robustness to confounding.
When PHDI was analyzed in tertiles, participants in the highest tertile (T3) had a significantly lower number of medications compared with those in the lowest tertile (T1). In Model A, membership in T3 was associated with a 10% lower medication count (RR = 0.90, 95% CI 0.83–0.96; p = 0.003), and this association persisted after full adjustment in Model B (RR = 0.92, 95% CI 0.87–0.98; p = 0.013). In contrast, no significant difference in medication burden was observed between the middle tertile (T2) and the lowest tertile in either model.
Taken together, these findings suggest a graded inverse association between diet quality and medication burden, driven primarily by individuals with the highest PHDI adherence, and consistent across alternative model specifications.
3.3. Association Between PHDI Score and Prescription of PPIs and NSAIDs
The descriptive association between PHD adherence and decreased consumption of potentially nephrotoxic medications, such as PPIs and NSAIDs, was also investigated through multivariate survey-weighted logistic regression models shown in Table 4.
When PHDI was analyzed as a continuous variable, each 10-point increase in PHDI was associated with significantly lower odds of both PPI and NSAID use. Specifically, higher PHD adherence was associated with 14% lower odds of PPI prescription (OR 0.86, 95% CI 0.79–0.94) and a similarly reduced odds of NSAID use (OR 0.86, 95% CI 0.76–0.97), independent of sociodemographic factors, lifestyle behaviors, comorbidities, kidney function, and albuminuria.
When PHDI was modeled in tertiles, distinct patterns emerged. Compared with participants in the lowest tertile (T1), those in the highest tertile (T3) had substantially lower odds of PPI use (OR 0.66, 95% CI 0.49–0.89). A similar inverse association was observed for NSAID use in T3, although the confidence interval crossed unity (OR 0.67, 95% CI 0.40–1.11). In contrast, individuals in the middle tertile (T2) showed no significant difference in PPI use compared with T1, but exhibited higher odds of NSAID prescription (OR 1.56, 95% CI 1.02–2.40).
Overall, these findings suggest a non-linear relationship between diet quality and the use of potentially nephrotoxic medications, with the most favorable prescribing profile observed among individuals with the highest PHD adherence.
4. Discussion
This nationally representative cross-sectional study of older adults with CKD demonstrates that higher adherence to the PHD is independently associated with lower medication burden. Participants in the highest PHDI tertile used approximately 8% fewer medications compared to those in the lowest tertile, even after comprehensive adjustment for sociodemographic factors, lifestyle behaviors, and comorbidities. Each 10-point increase in PHDI score was associated with a 3% reduction in medication count. Importantly, higher PHD adherence was specifically associated with reduced use of potentially nephrotoxic medications, including PPIs and NSAIDs, suggesting that dietary quality may influence medication needs in clinically relevant ways. To our knowledge, this is the first study to examine the relationship between adherence to a sustainable, plant-based dietary pattern and medication burden in older adults with CKD. The findings contribute to growing evidence that dietary interventions may serve as important adjuncts to pharmacological management in CKD, potentially reducing medication complexity and associated risks in vulnerable older populations [13,24].
A central finding of this study was the strong inverse association between PHDI adherence and use of potentially nephrotoxic medications, specifically PPIs and NSAIDs. These two medication classes represented the only significant associations observed in our multivariable analyses, with each 10-point increase in PHDI associated with 14% lower odds of PPI use (OR: 0.86, 95% CI: 0.79–0.94) and 14% lower odds of NSAID use (OR: 0.86, 95% CI: 0.76–0.97). When examined categorically, participants in the highest PHDI tertile demonstrated 34% lower odds of PPI use (OR: 0.66, 95% CI: 0.49–0.89) compared to those in the lowest tertile.
PPIs represent one of the most widely prescribed medication classes globally, with utilization rates particularly high among older adults [35]. In our CKD cohort, overall PPI use was 20.6%, with greater PPI use in the lowest score tertile (21.5%) and the lowest usage in the highest score tertile (16.7%, p = 0.007). The association between higher PHD adherence and reduced PPI use likely reflects multiple interconnected pathways related to gastrointestinal health and dietary composition. First, plant-based dietary patterns may directly reduce gastroesophageal reflux symptoms [36]. High consumption of fruits and vegetables provides dietary fiber, which has been associated with lower prevalence of gastroesophageal reflux disease (GERD) in observational studies [36,37]. Additionally, limiting processed foods, red meat, and high-fat items may reduce postprandial gastric acid secretion and lower esophageal sphincter relaxation, key mechanisms underlying GERD pathophysiology. Second, the anti-inflammatory properties of plant-predominant diets may ameliorate underlying gastrointestinal inflammation that contributes to dyspeptic symptoms and reflux [38]. Participants with higher PHDI scores in our cohort exhibited better overall metabolic health, including lower glucose levels and improved HDL-C, suggesting reduced systemic inflammation despite no significant differences in C-reactive protein. Chronic low-grade inflammation has been implicated in functional dyspepsia and may drive PPI prescribing beyond frank GERD [39]. Third, a recent study in a NHANES subcohort has shown that increased PHD adherence is associated with healthier body composition and decreased visceral adiposity [40], the latter being a major risk factor for GERD through increased intra-abdominal pressure and mechanical disruption of the gastroesophageal junction. In any case, the clinical significance of reduced PPI use in CKD populations cannot be overstated. Chronic PPI therapy has been associated with increased risks of acute kidney injury, accelerated CKD progression, electrolyte disturbances (particularly hypomagnesemia), and increased susceptibility to enteric infections, including Clostridioides difficile [35,41].
The inverse association between PHD adherence and NSAID use represents an equally important finding with significant nephrotoxic implications. Overall NSAID use was 8.3% in our cohort, with greater consumption in the lower PHDI score tertile (8.5%) and a lower use in the highest tertile (5.2%, p = 0.003). NSAIDs represent a major modifiable risk factor for acute kidney injury, CKD progression, and adverse cardiovascular events, particularly in older adults and those with pre-existing renal impairment [42,43]. Several mechanisms may explain reduced NSAID requirements among individuals with higher PHD adherence. Plant-based dietary patterns possess well-documented anti-inflammatory properties mediated through multiple bioactive compounds, including polyphenols, flavonoids, carotenoids, and omega-3 fatty acids from plant sources. These compounds modulate inflammatory pathways by reducing production of pro-inflammatory cytokines (interleukin-6, tumor necrosis factor-alpha), decreasing oxidative stress, and inhibiting cyclooxygenase and lipoxygenase enzymes, the same enzymatic targets of NSAIDs [44,45]. Consequently, plant-predominant diets may provide natural anti-inflammatory effects that reduce pain and inflammation, thereby decreasing analgesic medication requirements. In this regard, observational studies have demonstrated associations between plant-based dietary patterns and lower prevalence of chronic pain conditions, including osteoarthritis, rheumatoid arthritis, and fibromyalgia [46,47,48]. Additionally, improved metabolic health associated with higher PHD adherence, including better glycemic control and reduced uric acid levels observed in our cohort, may independently reduce inflammatory burden and pain. Hyperglycemia and hyperuricemia both contribute to systemic inflammation and oxidative stress, potentially amplifying pain perception and increasing analgesic requirements. The significant metabolic improvements observed across PHDI tertiles may therefore translate into reduced pain and inflammation, decreasing the clinical indications for NSAID prescribing.
The specificity of associations observed in our study, represented by significant reductions in PPIs and NSAIDs but not in guideline-directed cardiovascular or metabolic therapies, provides important mechanistic insights. This pattern suggests that dietary quality influences medication burden primarily by reducing the need for symptomatic treatments and potentially harmful medications rather than by eliminating evidence-based chronic disease therapies. The convergence of reduced PPI and NSAID use represents a particularly favorable safety profile for older adults with CKD. Both medication classes are frequently prescribed inappropriately or continued unnecessarily beyond initial clinical indications, contributing substantially to the polypharmacy burden. The American Geriatrics Society Beers Criteria identify both chronic PPI use (without documented indication) and NSAIDs as potentially inappropriate medications in older adults, particularly those with CKD [49]. Dietary interventions that reduce reliance on these agents align with deprescribing initiatives and may improve both kidney and overall health outcomes.
Importantly, the observed associations persisted after comprehensive adjustment for comorbidities, kidney function, and other confounders, suggesting that dietary effects on PPI and NSAID use operate through pathways beyond simple correlation with overall health status. Dietary interventions targeting improved diet quality may offer a complementary approach to reducing pharmacological burden while providing additional benefits for overall health and sustainability.
This study has several notable strengths. First, we analyzed data from NHANES, a large, nationally representative survey with rigorous data collection protocols, enhancing generalizability to the broader U.S. population of older adults with CKD. Second, dietary intake was assessed using two 24 h dietary recalls, which provide more detailed information than food frequency questionnaires. Third, medication data were collected through direct observation of medication containers, reducing recall bias. Fourth, we adjusted for numerous potential confounders, including socioeconomic factors, lifestyle behaviors, and comorbidities, strengthening causal inference.
However, important limitations must be acknowledged. The cross-sectional design precludes the establishment of temporal relationships or causality. Reverse causation remains possible; individuals with fewer comorbidities and medications may find it easier to adhere to healthy dietary patterns. Residual confounding cannot be excluded despite comprehensive covariate adjustment. Dietary assessment based on two 24 h recalls may not fully capture long-term dietary patterns and is subject to measurement error and recall bias. Misclassification of medication use and CKD status is possible, although the use of standardized protocols likely minimized such errors. CKD was defined based on single measurements of eGFR and ACR rather than the standard 3-month confirmation period, potentially overestimating CKD prevalence. Finally, our findings may not generalize to non-U.S. populations or to younger adults with CKD.
5. Conclusions
In this nationally representative cross-sectional study of U.S. older adults with CKD, higher adherence to the PHD was independently associated with lower medication burden, including reduced use of potentially nephrotoxic medications, such as PPIs and NSAIDs. These findings suggest that plant-based, sustainable dietary patterns may serve as valuable adjuncts to pharmacological management in CKD, potentially reducing medication complexity and associated risks in vulnerable older populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1GBD Chronic Kidney Disease Collaborators Global, regional, and national burden of chronic kidney disease in adults, 1990–2023, and its attributable risk factors: A systematic analysis for the Global Burden of Disease Study 2023 Lancet 20254062461248210.1016/S 0140-6736(25)01853-741213283 · doi ↗ · pubmed ↗
- 2Kovesdy C.P. Epidemiology of chronic kidney disease: An update 2022 Kidney Int. Suppl.20221271110.1016/j.kisu.2021.11.003PMC 907322235529086 · doi ↗ · pubmed ↗
- 3Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group KDIGO 2024 clinical practice guideline for the evaluation and management of chronic kidney disease Kidney Int.2024105 S 117S 31410.1016/j.kint.2023.10.01838490803 · doi ↗ · pubmed ↗
- 4Marx-Schütt K. Cherney D.Z.I. Jankowski J. Matsushita K. Nardone M. Marx N. Cardiovascular disease in chronic kidney disease Eur. Heart J.2025462148216010.1093/eurheartj/ehaf 16740196891 PMC 12167664 · doi ↗ · pubmed ↗
- 5Rashid A.M. Khan M.S. Cherney D.Z.I. Mehta A. Rangaswami J. Shafi T. Butler J. Rapid and Simultaneous Initiation of Guideline-Directed Kidney Therapies in Patients with CKD and Type 2 Diabetes J. Am. Soc. Nephrol.2025362061207610.1681/ASN.000000075240327845 PMC 12499624 · doi ↗ · pubmed ↗
- 6Naseralallah L. Khatib M. Al-Khulaifi A. Danjuma M. Prevalence and global trends of polypharmacy in patients with chronic kidney disease: A systematic review and meta-analysis Front. Pharmacol.202314112289810.3389/fphar.2023.112289836843919 PMC 9950938 · doi ↗ · pubmed ↗
- 7Zhang B. Wang J. Liu N. Liu W. Xi R. Wang P. Association between polypharmacy and chronic kidney disease among community-dwelling older people: A longitudinal study in southern China BMC Nephrol.20242516910.1186/s 12882-024-03606-x 38760750 PMC 11100214 · doi ↗ · pubmed ↗
- 8Oosting I.J. Colombijn J.M.T. Kaasenbrood L. Liabeuf S. Laville S.M. Hooft L. Bots M.L. Verhaar M.C. Vernooij R.W. Polypharmacy in patients with CKD: A systematic review and meta-analysis Kidney 3602024584185010.34067/KID.000000000000044738661553 PMC 11219116 · doi ↗ · pubmed ↗