Postoperative Pain Management Strategies Without Regional Analgesia in Knee Surgeries: A Scoping Review
Melissa Joo Young, Kevin Heebøll Nygaard, Gunhild Kjærgaard-Andersen, Christina Frøslev-Friis, Gayani Ranasinghe, Thomas Strøm, Rajesh Prabhakar Bhavsar

TL;DR
This review summarizes non-regional pain management strategies for knee surgeries when regional blocks are not possible, highlighting gaps in evidence and the need for standardized approaches.
Contribution
The study provides a comprehensive overview of non-regional analgesia strategies for knee surgeries, identifying key gaps and areas for future research.
Findings
Multimodal approaches combining systemic and local analgesics are commonly used but show limited evidence on functional recovery.
There is substantial heterogeneity in study designs and outcomes across different knee surgery types.
Few studies focus on tibial plateau or distal femoral fractures, and evidence is largely limited to inpatient outcomes.
Abstract
Background/Objectives: Intensive postoperative pain is a common challenge after knee surgeries such as total knee arthroplasty, arthroscopy, cruciate ligament or meniscus repair, and fixation of tibial plateau or distal femoral fractures. This scoping review mapped and summarized non-regional postoperative analgesia strategies to provide an overview of available approaches when regional blocks or neuraxial anesthesia are not feasible. Methods: We followed established methodological guidance for scoping reviews and report the data in accordance with the PRISMA-ScR checklist. We searched PubMed/MEDLINE, EMBASE, Scopus, and ClinicalTrials.gov in January 2025. Eligible designs included randomized controlled trials, non-randomized trials, observational studies, case series, and pilot studies. Results: We screened 3390 records and assessed 332 in full text. A total of 43 studies met the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
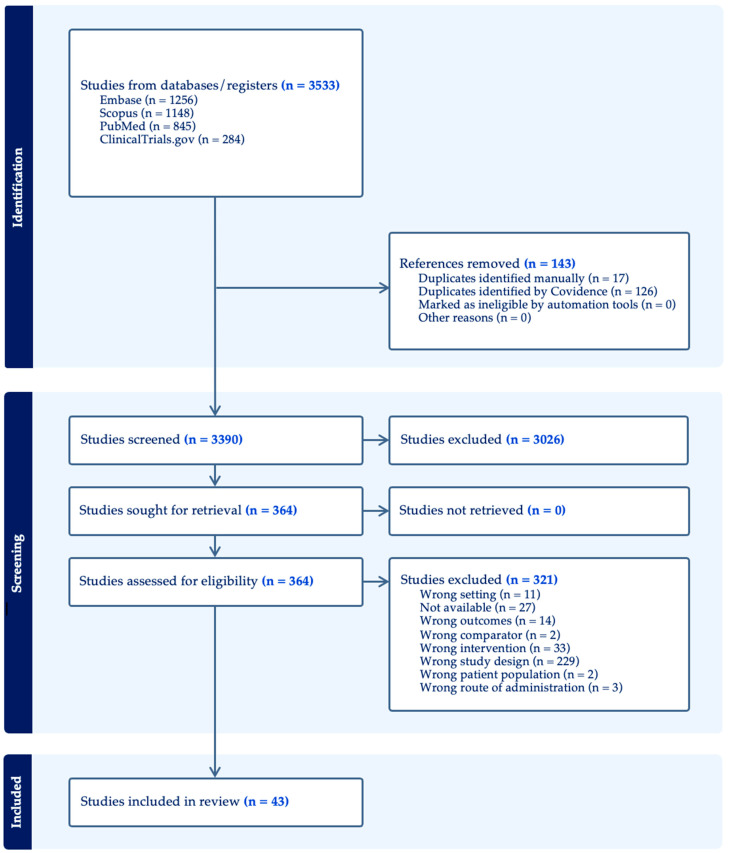 Figure 1
Figure 1| Study | Country | Design |
| Mean Age | Intervention | Comparator | Pain Management System | Mobilization Assessed | Primary Outcome | Secondary Outcomes | Headline Results | Conclusion | Authors Suggestions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Motamed et al. 2000 [ | France | Randomized, double-blind, placebo- and active-controlled | 37 | IV (pre-emptive morphine vs. M-6-G) | Placebo and active | Morphine PCA 24 h | No | Morphine consumption 24 h | Pain VAS; time to first PCA; AEs | Pre-emptive morphine ↓ early pain and 24 h morphine; M-6-G ineffective | Pre-emptive IV morphine beneficial; M-6-G not | Consider timing; avoid M-6-G | |
| Wadhwa et al. 2001 [ | Australia | Randomized, double-blind, placebo-controlled | 66 | Oral (dextromethorphan) | Placebo | Morphine PCA 24 h; CPM for 24 h | Yes (CPM tolerance) | 24 h morphine use | Pain during CPM; side effects | ↓ morphine ~29%; no pain benefit; ↑ nausea | Not clinically useful despite opioid sparing | Avoid routine dextromethorphan | |
| Zippel & Wagenitz 2006 [ | EU | Multicenter RCT, double-blind, equivalence | 252 | 60 | IV (dexketoprofen vs. ketoprofen) | Active comparator | Rescue morphine/paracetamol/propacetamol | No | SAPID 0–8 h (VAS) | PID; rescue use; AEs | Equivalent analgesia; trend fewer AEs with dexketoprofen | Either NSAID acceptable; tolerability may favor dexketoprofen | Consider dexketoprofen for tolerability |
| Sıvrıkoz et al. 2014 [ | Turkey | Randomized, double-blind, placebo-controlled | 118 | 60 | IV (dexketoprofen vs. lornoxicam) | Placebo | Morphine PCA 24 h | No | VAS rest/move | Morphine use; PCA boluses | Both ↓ pain/opioids; dexketoprofen superior | Prefer dexketoprofen among tested NSAIDs | Use IV dexketoprofen 12-hourly |
| Chen et al. 2015 [ | Taiwan | RCT | 30 | 68 | Music (audio) | Usual care | Standard GA; opioids PRN | No | Physiologic parameters; postop VAS | Opioid dose | BP stabilization; no pain/opioid difference | Music may modulate stress, not analgesia | Further research; feasible low-risk adjunct |
| Ban et al. 2017 [ | China | Prospective randomized (single-blind) | 110 | 64 | Periarticular multimodal injection | Saline | Sufentanil PCA + celecoxib | Yes (ROM and activity) | NRS pain; NSAID use; WOMAC; LOS | Satisfaction; AEs | Lower pain; better ROM; shorter LOS | Periarticular injection improves early recovery | Adopt LIA routinely |
| Politi et al. 2017 [ | USA | Prospective randomized | 120 | IV vs. PO (acetaminophen) | Route comparison | Multimodal; hydromorphone/oxycodone | No | 24 h VAS; hydromorphone use | Early 0–4 h VAS; cost | Equivalent 24 h pain/opioids; small early benefit IV | Prefer PO due to cost; IV limited role | Use oral acetaminophen routinely | |
| Hickman et al. 2018 [ | USA | Randomized, double-blind, placebo-controlled equivalence | 486 | IV vs. Oral (acetaminophen) | Equivalence (IV vs. PO) | Standardized multimodal | Yes (time to walk 10 ft) | 24 h opioid MME | Pain; PONV; PACU; LOS; time to ambulation | Oral equivalent to IV | Use oral as cost-effective | Prefer oral route | |
| Xiao et al. 2018 [ | China | Retrospective cohort | 300 | 62.05.00 | IV (flurbiprofen axetil) vs. Oral (celecoxib) vs. None | FA vs. CX vs. placebo | Morphine PCA | Yes (ROM) | VAS rest/move | Morphine use; ROM; LOS; AEs | FA best early pain/↓opioids; both shortened LOS | FA and CX beneficial; FA > CX early | Prefer FA when available; otherwise CX |
| Kim et al. 2019 [ | South Korea | Prospective RCT, double-blind | 67 | 66 | IV (dexmedetomidine infusion) | Saline | Fentanyl PCA 48 h | No | Inflammation markers (IL-6, TNF-α) | Pain scores; PCA use; hemodynamics | Lower pain at 12–48 h; no opioid/LOS benefit | Dexo reduces pain/inflammation without opioid sparing | Potential adjunct for pain; monitor HR |
| Shao et al. 2020 [ | China | RCT | 196 | 68.05.00 | Oral (meloxicam) | Preop vs. postop timing | Fentanyl+tramadol PCA 48 h | Yes (HSS at 3 mo) | VAS rest/flexion; PCA use | PGA; HSS 3 mo; AEs | Preop dosing ↓ early pain and PCA use | Prefer preop meloxicam timing | Administer meloxicam preop |
| Peng et al. 2021 [ | China | Within-patient RCT (bilateral TKA) | 60 | 65.01.00 | Periarticular cocktail ± steroid | Cocktail without steroid | Morphine PCA 3 days; NSAIDs | Yes (ROM; HSS) | VAS rest/move | ROM; swelling; temp; preference; AEs | No added benefit from steroid | Steroid unnecessary in robust LIA | Use LIA without steroid routinely |
| Coviello et al. 2022 [ | Italy | Prospective randomized case–control | 100 | 71 | Device (continuous cold flow) | Gel ice packs | Standard multimodal; tramadol rescue | Yes (ROM) | VAS pain (T0–day5) | Tramadol use; ROM; transfusions; satisfaction | Lower 24 h VAS and less tramadol; better ROM early | CCF safer/more effective than gel packs for early recovery | Adopt CCF for pain control after TKA |
| Yuan et al. 2022 [ | China | Prospective RCT, double-blind | 100 | 68 | Oral (duloxetine) | Placebo | Multimodal + LIA + PCA rescue | Yes (ROM) | rVAS and aVAS over 2 w | Opioid use; ROM; AEs | Lower pain; ↓ opioids; better early ROM; fewer N/V/constipation | Duloxetine effective adjunct | Add perioperative duloxetine selectively |
| Paulin et al. 2023 [ | India | Double-blind RCT | 49 | 22 | IV (ketamine bolus+infusion) | Saline | Morphine PCA 72 h | Yes (TUG, ROM) | TUG at 72 h | Pain; morphine use; ROM; discharge day; OKS | No significant improvement in TUG, pain, or opioids | Low-dose ketamine not beneficial in this setting | Avoid routine ketamine for oncologic TKA |
| Kraus et al. 2024 [ | USA | RCT | 76 | 66 | Genetics-guided prescribing (preop test) | Standard care | Multimodal incl. periarticular local anesthetic | No | OBAS at 24 h | VAS; opioid use; side effects; satisfaction | No benefit on pain or opioids | Routine pharmacogenomics not useful in standard-risk TKA | Do not adopt routinely for pain control |
| Sönmez Sağlam et al. 2025 [ | Türkiye | Prospective RCT (3-arm) | 76 | 65 | Cryotherapy device; IV tranexamic acid | Gel cold packs | Diclofenac IM + paracetamol IV | Yes (ROM) | Blood loss; VAS | ROM; complications | Cryo ↓ pain and preserved ROM; TXA ↓ blood loss | Both strategies enhance recovery (different domains) | Consider cryotherapy; use TXA for blood-sparing |
| Study | Country | Design |
| Mean Age | Procedure | Intervention | Comparator | Pain Management System | Mobilization Assessed | Primary Outcome | Secondary Outcomes | Headline Results | Conclusion | Authors Suggestions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Koinig et al. 1998 [ | Austria | Randomized double-blind placebo-controlled | 46 | Diagnostic/therapeutic AKS under TIVA | IV magnesium sulfate infusion | IV placebo | Propofol + fentanyl TIVA; postop fentanyl as needed | No | Intra- and postoperative fentanyl use | VAS 5–240 min; AEs | ↓ intra/postop fentanyl; VAS similar | Opioid-sparing without VAS change | Consider Mg for opioid reduction | |
| Reuben & Connelly 1999 [ | USA | Randomized double-blind (5-arm) | 50 | Outpatient meniscal arthroscopy | IA bupivacaine ± clonidine (or clonidine alone); SC clonidine variants | Multiple active comparators including IA saline group equivalence | Oral codeine–acetaminophen (Tylenol 3) | No | Time to first analgesic (duration) | VAS; opioid tablets; discharge time | IA bupivacaine + clonidine prolonged duration; fewer tablets | Add IA clonidine to bupivacaine | Use IA clonidine 1 µg/kg with bupivacaine | |
| Gentili et al. 2001 [ | France | Randomized, double-blind, 6-arm | 84 | Meniscus repair (ambulatory) | IA clonidine and/or IA neostigmine (± SC counterpart) | IA + SC saline | Rescue paracetamol 1 g PO (no opioids) | No (but VAS during knee flexion) | VAS rest and mobilization 1–24 h | Time to first paracetamol; total doses; AEs | All active IA regimens ↓ VAS vs. placebo; clonidine ↑ hypo/brady | IA clonidine/neostigmine effective; combination not superior | Choose agent mindful of clonidine hypotension | |
| Vranken et al. 2001 [ | Netherlands/Belgium | Randomized double-blind (3-arm) | 60 | 37 | Diagnostic day-case AKS | IA sufentanil (5 or 10 µg) vs. IV 5 µg | IV sufentanil | Paracetamol intraop; PO paracetamol postop | No | VAS T1–T4 | Paracetamol use; time to PACU discharge | IA sufentanil ↓ pain vs. IV; faster discharge eligibility | IA sufentanil 5 µg effective and safe | Prefer IA over IV sufentanil in day-case AKS |
| Ménigaux et al. 2005 [ | France | Randomized, double-blind, placebo-controlled | 40 | 32 | ACL repair (arthroscopic) | Oral (gabapentin) | Placebo | GA + PCA morphine 48 h; ketoprofen PRN | Yes (ROM days 1–2) | VAS pain; 0–48 h morphine | Anxiety VAS; AEs; early ROM | ↓ PACU pain; ↓ 48 h morphine by ~58%; ↑ ROM day 1–2 | Gabapentin enhances early recovery and opioid-sparing | Consider preop gabapentin 1200 mg |
| Arai et al. 2006 [ | Japan | Randomized controlled (single-blind) | 24 | 64 | Partial meniscectomy | IA warmed lidocaine vs. room-temp | Temperature comparison | Pentazocine premed; diclofenac PRN | No | Intraoperative pain VAS | Intraop pentazocine; postop diclofenac | Warmed lidocaine ↓ intraop pain and analgesic use | Temperature optimization improves IA local anesthetic effect | Warm IA lidocaine to ~40 °C |
| Jacobson et al. 2006 [ | Sweden | Prospective randomized (NSAID vs. coxib) | 122 | 48 | Outpatient AKS (meniscus/synovium/diagnostic) | Oral lornoxicam vs. rofecoxib | Coxib vs. NSAID | Paracetamol PACU; IA fentanyl + local portal infiltration; rescue dextropropoxyphene | No | Rescue need days 0–4 | VAS; side effects; satisfaction | No difference; many still need rescue | Conventional NSAID reasonable first choice | No added benefit of coxib in this setting |
| Tashjian et al. 2006 [ | USA | Randomized, double-blind (zolpidem vs. placebo) + open standard-care arm | 68 | 47 | Outpatient meniscus/loose bodies | Oral (zolpidem nights 1–7) | Placebo and standard care | Hydrocodone/acetaminophen + ibuprofen; standard rehab | No | Daily VAS pain 7 d; opioid tablets used | Fatigue VAS; AEs | ↓ pain and opioid tablets with zolpidem; ↓ fatigue | Improved sleep lowers pain/opioid use first week | Consider short zolpidem course post-arthroscopy |
| Hashemi et al. 2010 [ | Likely Iran | Randomized, double-blind (3-arm) | AKS (general) | IA pethidine (preemptive vs. preventive) | IA saline | Rescue systemic morphine PRN | No | VAS 1–24 h | Time to first morphine; 24 h morphine | Preemptive dosing best: ↓ VAS, ↓ morphine, delayed first dose | Timing matters; preemptive IA pethidine superior | If using IA opioid, give pre-incision | ||
| Sun et al. 2013 [ | China | Systematic review/meta-analysis of 7 RCTs | 230 | Arthroscopic knee surgery (mixed) | Intraarticular clonidine | IA placebo | Standard GA across RCTs | No | VAS 1–24 h | Rescue need; AEs (nausea ↓; hypotension ↑) | Small, short-lived VAS reduction ≤4 h; ↓ rescue; ↑ hypotension risk | Adjunct only; monitor BP | IA clonidine not standalone; consider as add-on | |
| Isik et al. 2014 [ | Türkiye | Randomized, double-blind, placebo-controlled (3-arm) | 60 | Partial meniscectomy | IA ketamine ± levobupivacaine | IA saline | Rescue tramadol IV as needed | No | VAS at 1–24 h | Rescue tramadol; side effects | IA ketamine improves early pain; ketamine+levobupivacaine best at 4–12 h; ↓ early tramadol | Adding local anesthetic augments IA ketamine effect | Consider IA ketamine + levobupivacaine | |
| Onda et al. 2016 [ | Japan | Randomized parallel-group (3-arm) | 160 | Second-look after ACL or meniscal procedures | Oral (celecoxib vs. loxoprofen vs. acetaminophen) | Three-way comparison | No routine opioids; pre-discharge IV flurbiprofen; rebamipide prophylaxis | Yes (daily activities allowed POD1 per pain) | VAS rest/movement to 48 h | Subjective global relief; AEs | Celecoxib < acetaminophen at 24–48 h; loxoprofen < acetaminophen at 48 h rest | COX-2/NSAID superior to acetaminophen early | Prefer celecoxib for AKS acute pain | |
| Zhou et al. 2017 [ | China | Randomized, open-label (3-arm) | 182 | 36 | Meniscal arthroscopy | Oral celecoxib (−24 h vs. −1 h vs. +4 h) | Timing arms | Rescue pethidine 5 mg/kg | No | VAS at rest and 90° flexion 12–24 h | PGA; rescue use; AEs | Preop (−24 h/−1 h) < postop (+4 h) for pain; rescue trend ↓ | Preemptive celecoxib effective; −1 h optimal | Dose celecoxib preop (preferably −1 h) |
| Uribe et al. 2018 [ | USA | Randomized double-blind active-comparator pilot | 51 | 43,7 | Outpatient AKS (mixed) | IV ibuprofen (preop) vs. IV ketorolac (postop) | Active comparator | Standard GA; PACU hydromorphone rescue; home ibuprofen + oxy/APAP | No | PACU VAS | PACU opioids; 24 h opioids; time to first opioid | Preop ibuprofen ↓ arrival VAS & PACU opioids; effect fades by 2 h | Preemptive IV NSAID helpful for very early period | Use IV NSAID preop if IV route planned |
| El Baz & Farahat 2019 [ | Egypt | Randomized double-blind (3-arm) | 90 | 27,5 | Diagnostic/therapeutic AKS | IA levobupivacaine ± dexmedetomidine | IA saline | Rescue meperidine IV | No | VAS 0.5–24 h | Time to first rescue; total meperidine; AEs | Adding dexmedetomidine ↓ VAS and opioids markedly | α2 augmentation of IA local anesthetic is effective | Consider IA dexmedetomidine adjuvant |
| Hou et al. 2019 [ | China | Randomized, non-blinded | 296 | 37,5 | AKS (mixed procedures) | Oral meloxicam (pre vs. post) | Postoperative dosing | Rescue pethidine | No (3-mo function only) | VAS rest/flexion; PGA | Rescue pethidine; ROM/IKDC/Lysholm 3 mo | Preop dosing ↓ early (≤12 h) pain & PGA; ↓ rescue | Preemptive meloxicam beneficial early | Give meloxicam preoperatively |
| Sağır et al. 2020 [ | Türkiye | Randomized, double-blind (3-arm) | 75 | 46,7 | Arthroscopic meniscectomy | Intraarticular ketamine (0.5 vs. 1 mg/kg) + periarticular bupivacaine | Intraarticular saline + bupivacaine | PCA morphine in PACU; GA with fentanyl | No | VAS rest/move; time to first analgesic | Morphine use; discharge time; AEs | 1 mg/kg reduced early morphine; no 24 h total or discharge time effect | IA ketamine provides early opioid-sparing only | If used, 1 mg/kg offers best early benefit |
| Liu et al. 2021 [ | China | Randomized, controlled (parallel) | 232 | 43 | AKS (mixed procedures) | Oral oxycodone/acetaminophen vs. oral celecoxib | Celecoxib | Rescue pethidine PRN | No | VAS rest/motion 6–72 h | Rescue use; satisfaction; AEs | OPT better ≤24 h; ↓ rescue pethidine; similar AEs | OPT superior for early pain | Prefer OPT when regional not used |
| Study | Country | Design |
| Mean Age | Procedure | Intervention | Comparator | Pain Management System | Mobilization Assessed | Primary Outcome | Secondary Outcomes | Headline Results | Conclusion | Authors Suggestions |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Barber & Gladu 1998 [ | USA | Double-blind randomized multicenter | 125 | 29 | ACLR (patellar-tendon autograft) | Oral ketorolac vs. hydrocodone + APAP (after parenteral loading for ketorolac) | Opioid combo | Uniform GA; CPM; local infiltration | No (CPM used uniformly) | SPID/TOTPAR at 3–4 h post dose | Global ratings; AEs | In outpatients (early dosing) ketorolac > hydrocodone+APAP | NSAID strategy effective early with loading dose | Use oral ketorolac post-ACLR with prior parenteral dose |
| Al-Metwalli et al. 2008 [ | Saudi Arabia | Randomized, double-blind, placebo-controlled | 60 | 38 | Partial meniscectomy | IA dexmedetomidine 1 µg/kg vs. IV vs. placebo | IV dEX; IA saline | Diclofenac IV primary; tramadol PRN | No | VAS 1–24 h | Time to first analgesic; diclofenac use; haemodynamics; sedation | IA dEX ↓ VAS up to 6 h; delayed first analgesic; ↓ diclofenac; fewer systemic effects vs. IV | IA dexmedetomidine effective and safe adjunct | Prefer IA over IV dEX for AKS |
| Armellin et al. 2008 [ | Italy | Randomized, double-blind controlled | 120 | 30 | Outpatient ACL reconstruction | IA ropivacaine + clonidine ± sufentanil 5 µg | Without sufentanil | Preemptive ketorolac; postop APAP+ketoprofen; cryotherapy | No | VAS 1–24 h | Rescue sufentanil; discharge timing; AEs | Pain low both; fewer rescues with IA sufentanil in 1st hour | Opioid add-on not necessary with robust LIA | Ropivacaine + clonidine sufficient for routine cases |
| Elseify et al. 2011 [ | Qatar/Egypt | Randomized, double-blind, 3-arm | 60 | 31.5 | Primary ACL reconstruction | IV paracetamol vs. IV parecoxib vs. both | Active comparators | Rescue IV morphine to VAS ≤3 | No | VAS rest/movement (PACU, 2 h, 8 h) | Morphine totals to 8 h; PACU time; satisfaction | Combo ↓ movement pain early; ↓ morphine; shorter PACU time | Paracetamol+parecoxib best for early ACLR pain | Combine IV paracetamol + parecoxib |
| Mardani-Kivi et al. 2013 [ | Iran | Triple-blind randomized placebo-controlled | 117 | 26 | ACLR or partial meniscectomy | Celecoxib 400 mg PO −2 h (single dose) | Placebo | Rescue pethidine 0.5 mg/kg IV | No | VAS 6 h and 24 h | Pethidine consumption; AEs | Celecoxib ↓ VAS and pethidine at 6 and 24 h | Effective preemptive COX-2 for AKS | Use celecoxib 400 mg preop |
| Ma et al. 2021 [ | China (multicentre) | Randomized controlled trial | 464 | 41 | AKS (ligament recon, meniscectomy, synovectomy, IAFR) | Preop NSAIDs (celecoxib/meloxicam/rofecoxib) vs. postop | Preop vs. postop dosing | Standard GA; rescue pethidine | No | VAS rest and passive movement | Rescue pethidine; satisfaction; AEs | Preop dosing ↓ early (≤24 h) pain and rescue opioids | Preemptive NSAIDs superior early | Give NSAID ~2 h preop |
| Wang et al. 2021 [ | China/ | Retrospective comparative cohort | 716 | 40 | Single-bundle ACL reconstruction (non-acute) | No irrigation vs. 1 L vs. 3 L; 23 °C vs. 36 °C vs. 4 °C | Different irrigation volume/temperature | NSAIDs, cold compresses; early rehab from POD2 | Yes (rehab started POD2; no quantitative endpoint) | VAS pain; swelling; skin temperature | CRP, IL-1/6/10 | No differences in pain, swelling, or inflammatory markers | Irrigation volume/temperature had no clinical effect | Standardize; choose based on practicality |
| Alipour et al. 2023 [ | Iran | Randomized, double-blind, placebo-controlled | 60 | 32.7 | Meniscectomy ( | Intraarticular remifentanil 200 µg | IA saline placebo | GA (propofol/sevo); postop meperidine 25 mg if VAS ≥4 | No | VAS 1–24 h | Analgesic requests, time to first dose, total meperidine | Large ↓ in VAS at all times; median 0 mg meperidine vs. 100 mg control | IA remifentanil markedly reduces pain and opioid use | Consider IA remifentanil (cartilage safety to consider) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnesthesia and Pain Management · Cancer, Stress, Anesthesia, and Immune Response · Total Knee Arthroplasty Outcomes
1. Introduction
Knee surgeries such as total knee arthroplasty (TKA), knee arthroscopies, cruciate ligament or meniscus repair (CLMR), and fixation of tibial plateau or distal femoral fractures are standard procedures frequently associated with intense postoperative pain [1,2].
Severe postoperative pain complicates physiotherapy and early ambulation. Delayed mobilization increases length of stay (LOS) and healthcare costs [3,4]. Lack of early mobilization affects the surgical outcome because it increases the risk of joint stiffness, contractures, and muscle atrophy [5,6]. Insufficient pain management, high opioid consumption, and immobility caused by motor-blocking regional techniques may also increase the risk of adverse events such as deep venous thrombosis, pneumonia, and ileus [7,8,9]. In contrast, patients with well-managed postoperative pain have higher satisfaction scores, shorter hospital stays, improved early ambulation, and fewer postoperative complications [10,11].
Multimodal analgesic strategies have been introduced because they combine synergistic pharmacological effects with non-pharmacological mechanisms to improve pain control. These strategies include neuraxial anesthesia, regional nerve blocks, systemic analgesics, and local infiltration anesthesia [12]. Multimodal strategies may reduce opioid consumption and may limit adverse effects such as nausea, constipation, respiratory depression, and opioid-induced hyperalgesia [11,13,14,15]. Regional and neuraxial techniques are effective; however, the implementation of regional anesthesia is not resource-neutral, as it typically requires additional trained personnel, dedicated equipment (e.g., ultrasound), and non-trivial procedural time. In contemporary workflow analyses and service-implementation studies, these added inputs are explicitly highlighted (including the need for additional staffing/equipment and operating room time considerations), as, e.g., continuous peripheral nerve blocks have been reported to require approximately 10 min longer than single-injection blocks, with correspondingly higher estimated physician-time cost, thus also limiting their universal applicability [16,17]. In addition, side effects such as quadriceps weakness that may increase fall risk, are often seen in regional anesthesia [18]. As surgical techniques evolve, clinicians have explored non-regional strategies to provide adequate analgesia without relying on nerve blocks or spinal anesthesia.
Although multimodal pain management is widely used, the available literature is fragmented across procedures, drug classes, and study designs. No review has mapped non-regional postoperative strategies across the full range of knee surgeries. The absence of an overview makes it challenging to understand which systemic, local, or non-pharmacological strategies are available and where essential knowledge gaps remain. The literature also varies in age groups, functional demands, and rehabilitation trajectories, especially when comparing arthroplasty, arthroscopy, ligament reconstruction, and fracture surgery. These populations differ markedly in invasiveness and postoperative pain profiles, but all require adequate non-regional analgesia when regional techniques are not feasible.
This scoping review aimed to map the available non-regional postoperative analgesia strategies for knee surgery and to identify knowledge gaps that may inform future clinical trials and systematic reviews.
2. Materials and Methods
2.1. Study Design
We conducted a scoping review to systematically map and describe non-regional pain management strategies used in knee surgery. The review followed established methodological guidance and framework for scoping reviews from Arksey and O’Malley, and adhered to the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-analysis Guidelines Extension for Scoping Reviews). The protocol was developed a priori and registered at the Open Science Framework (https://doi.org/10.17605/OSF.IO/DVSRF (accessed on 24 December 2025)).
Given the exploratory nature of scoping reviews, heterogeneous surgical procedures were intentionally included to allow for comprehensive mapping of strategies potentially transferable across clinical contexts. Because the objective was descriptive rather than comparative, no formal meta-analysis was conducted.
The PCC framework (Table 1) was used to help define the research question and map the scope of this review.
Eligible study designs included randomized controlled trials, non-randomized trials, observational studies, case series, and pilot studies, with interventions initiated from admission for surgery until discharge. The focus of our review is perioperative pain management strategies, as many pain management strategies which influence postoperative pain include a combination of both pre-, intra- and postoperative interventions whose effects cannot be clearly distinguished from one another. Therefore, to preserve a broad study selection, we included studies with interventions starting from admission for surgery to postoperative discharge.
2.2. Exclusion Criteria
Studies evaluating regional or neuraxial techniques, also in combination with non-regional pain management techniques.Surgical technique modifications, in which the surgical procedure itself was intentionally altered in a way likely to independently affect postoperative pain or functional recovery (e.g., minimally invasive or muscle-sparing approaches, navigation- or robotic-assisted techniques, altered tourniquet strategies, or the incorporation of periarticular local infiltration analgesia as part of the surgical technique rather than the anesthetic regimen).Non-eligible designs (editorials, letters, reviews, protocols).Studies reporting only long-term pain outcomes defined as time post-discharge.Studies including pediatric populations.
2.3. Information Sources and Search Strategy
We searched PubMed/MEDLINE, Embase, Scopus, and ClinicalTrials.gov in January 2025. Reference lists of included studies were screened for additional eligible literature.
Search strategies combined three core concepts: postoperative pain management, knee surgery, and exclusion of regional anesthesia. The review team developed the search strategy, which was externally peer-reviewed by an experienced medical librarian in accordance with the Peer Review of Electronic Search Strategies (PRESS) recommendations. Full search strings are provided in File S1.
2.4. Study Selection
All records were managed in Covidence, (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at: www.covidence.org, 26 January 2025) where duplicates were removed. Two reviewers independently screened titles and abstracts, followed by full-text screening of potentially eligible studies. Discrepancies were resolved by consensus or consultation with a third reviewer. Reasons for full-text exclusion were documented.
2.5. Data Extraction
Data from included studies were extracted using a pre-piloted form capturing study characteristics, population, surgical procedure, anesthesia technique, co-analgesics, intervention, comparator details, acute postoperative pain outcomes, and adverse events.
2.6. Data Synthesis
The extracted data were synthesized using a descriptive, iterative approach appropriate for scoping reviews. We first grouped studies according to the class of systemic analgesic intervention evaluated (e.g., opioids, acetaminophen, NSAIDs/COX-2 inhibitors, gabapentin, ketamine, intravenous lidocaine, alpha-2 agonists, corticosteroids, magnesium, nefopam, duloxetine). Within each class, findings were further stratified by surgery type (arthroplasty, arthroscopy, ligament reconstruction) and study design. Key outcome domains (pain intensity scores, opioid consumption, time to mobilization, length of stay, and adverse events) were tabulated to allow visual comparison across interventions and study types. Narrative synthesis was then used to summarize trends, highlight consistencies or discrepancies between studies, and identify evidence gaps. Meta-analysis was not planned a priori but was considered only if ≥3 sufficiently homogeneous RCTs were available for a specific intervention and outcome.
3. Results
A total of 3533 records were identified through database searches (Embase = 1256; Scopus = 1148; PubMed = 845; ClinicalTrials.gov = 284). After removal of 143 duplicates (17 manually and 126 via Covidence), 3390 unique records remained for title and abstract screening. Of these, 3026 were excluded as clearly irrelevant. The remaining 364 full-text articles were assessed for eligibility, and 320 were subsequently excluded, primarily due to unsuitable study design (n = 229), wrong intervention (n = 33), unavailable full text (n = 27), wrong setting (n = 11), non-matching outcomes (n = 14), or other ineligibility criteria such as wrong comparator, population, or route of administration. No studies were excluded due to retrieval failure. Ultimately, 43 studies met the inclusion criteria and were included in this scoping review (Figure 1).
The included studies represented a geographically diverse sample, with the most considerable contributions from China (n = 9) and the United States (n = 6). European countries accounted for a substantial proportion of the evidence base, with France (n = 3), Belgium (n = 2), and Italy (n = 2) leading, and others with a single publication each. Only a few studies originated from the Middle East or Asia outside China, reflecting uneven global research activity (File S2).
These studies collectively examined a broad spectrum of non-regional analgesic and non-pharmacological strategies used in knee surgery, representing diverse surgical contexts, pharmacological regimens, and study designs. To facilitate comparison, the included studies were categorized into three surgical groups based on procedure type and clinical context: total knee arthroplasty (TKA), arthroscopic procedures and cruciate ligament or meniscus repair (CLMR). We found no focused literature on non-regional analgesic and non-pharmacological strategies used in tibial plateau or femoral fracture surgery, and no data was grouped for this category.
The following sections present detailed findings for each group, describing patient demographics, intervention types, mobilization outcomes, and patterns of multimodal pain management. These subgroup summaries are then synthesized for comparison to highlight overarching trends, knowledge gaps, and evolving clinical directions across all knee surgery populations.
3.1. Total Knee Arthroplasty (TKA) Set: Table 2
A total of seventeen studies, including 2243 participants, were analyzed. The mean of reported mean ages was approximately 62.0 years (median of means 65.1 years), sex was reported in 12 studies accounting for 1513 participants, and the average proportion of males was about 32%. Mobilization outcomes were assessed in 10 of the 17 studies, typically using range of motion (ROM), timed up-and-go (TUG), time-to-walk, or continuous passive motion (CPM) tolerance. However, many trials did not include functional endpoints. Interventions were predominantly pharmacological (12 studies), with two non-pharmacological strategies (continuous cold-flow therapy and music), two studies of local pharmacological approaches (periarticular infiltration or local infiltration anesthesia (LIA)), and one study comparing a mixed regimen (cryotherapy vs. IV tranexamic acid). Across the pharmacological studies, patient-controlled opioid analgesia (morphine, fentanyl, or sufentanil) was commonly employed, usually within a multimodal background of acetaminophen and/or NSAIDs, often supplemented with LIA. Several trials directly compared route or timing of administration, including IV versus oral acetaminophen, pre- versus postoperative NSAIDs, IV versus oral NSAIDs, and the addition of steroids to LIA.
3.2. Arthroscopy Set: Table 3
Eighteen studies with 1870 participants were included. The reported mean age was approximately 42.0 years (median of means = 43 years), with an average of ~50% male participants across the 7 studies that reported sex distribution, accounting for 862 of the participants. Mobilization outcomes were assessed in only 2 studies, with assessments limited to range of motion or day-to-day activities in a few trials. Interventions were dominated by pharmacological strategies, including systemic NSAIDs, opioids, and a wide range of intra-articular adjuvants, while non-pharmacological strategies were almost absent. Routes of administration spanned oral (celecoxib, loxoprofen, meloxicam, oxycodone/acetaminophen, zolpidem), intravenous (magnesium, NSAIDs), and intra-articular (ketamine, clonidine, neostigmine, levobupivacaine, sufentanil, warmed lidocaine).
3.3. Cruciate Ligament or Meniscus Repair (CLMR) Set: Table 4
Eight studies with 1722 participants were included. The reported mean age was approximately 33.5 years (median of means ~32.1 years), with an average of ~63% male participants in the 7 studies that reported sex, accounting for 1006 of the included participants. Mobilization or physiotherapy outcomes were only reported in one cohort, noting rehabilitation beginning on postoperative day two and no quantitative mobilization outcomes reported. The interventions tested covered a range of systemic and local strategies, including systemic NSAID timing comparisons, systemic drug combinations, intra-articular adjuvants (remifentanil, dexmedetomidine, sufentanil), and non-pharmacologic intraoperative irrigation protocols.
3.4. Comparison Across Groups
Seventeen studies with a total of 2243 participants were included in the TKA studies and involved the oldest populations (mean ~62 years, ~32% male) and more often assessed mobilization outcomes (10/17, typically ROM, TUG, or time-to-walk), with interventions spanning from pharmacological, local periarticular infiltration to non-pharmacologic, and mixed strategies. Arthroscopy studies (18 trials, 1870 participants) focused on a younger cohort (~42 years) more balanced in sex (~50% male), with mobilization rarely assessed and outcomes limited to very early pain (0–24 h) and day-case recovery. The CLMR set (8 trials, 1722 participants) represented the youngest groups (~33.5 years, ~63% male), with mobilization outcomes almost absent, and tested both systemic combinations and potent intra-articular adjuvants.
Across all three surgical groups, the most frequently described intervention was multimodal pain management strategies comprising combining systemic non-opioid analgesics with LIA. Opioids were primarily used as rescue therapy in cases of postoperative pain. NSAIDs and COX-2 inhibitors were the most frequently reported systemic interventions in all three groups, often in combination with paracetamol. Local strategies such as periarticular injections and cryotherapy were widely represented in the TKA set, as with LIA with or without adjuvants (e.g., clonidine, dexmedetomidine, ketamine, opioids) in the arthroscopy and CLMR set. A broad range of adjunctive interventions was explored across all three groups, including α2-agonists, NMDA antagonists, antidepressants, sleep or stress-modulating therapies, with highly heterogeneous outcome measures. Overall, the literature mapped in this scoping review demonstrates a tendency to focus on multimodal, opioid-sparing analgesic strategies, with noticeable variation in intervention type and reported outcome measures depending on surgical procedure.
4. Discussion
This scoping review provides a comprehensive overview of current non-regional strategies for postoperative pain management in knee surgeries, which predominantly include TKA, arthroscopy, and CLMR. The strategies reflect a broad clinical shift toward multimodal regimens and reduced reliance on opioids, although the extent and composition of these approaches varied considerably across studies. The included studies revealed significant gaps in consistency, comparability, and limited evaluation beyond the early postoperative period, that require further investigation before a standardized regimen can be recommended. As a scoping review, the findings should be interpreted as a descriptive overview of current practices and evidence gaps rather than conclusions regarding comparative efficacy.
The most consistent observation is the central role of systemic multimodal pharmacotherapy. Regular administration of non-opioid agents, particularly NSAIDs and acetaminophen, was frequently reported to be associated with lower early postoperative pain scores or reduced opioid use, although reporting practices differed markedly. Some compared oral and intravenous formulations; others examined pre-emptive versus postoperative initiation. None of these comparisons established a clear superiority of one regimen.
The observed variation in the selection of agents, routes, and timing likely reflects both the complexity of postoperative pain mechanisms and the diversity of clinical settings in which knee surgery is performed [62].
Postoperative pain after knee surgery arises from multiple nociceptive sources, and no single drug can target all mechanisms [11]. Consequently, clinicians began to combine agents with complementary mechanisms to achieve additive or synergistic analgesia, while reducing opioid exposure and its related adverse effects [63]. Similarly, some investigators emphasized pre-emptive dosing to inhibit peripheral sensitization before tissue injury, whereas others prioritized postoperative initiation to align with the recovery workflow and minimize bleeding risk. Such variation also reflects the heterogeneity of patient populations: elderly arthroplasty recipients often have comorbidities limiting NSAID use, whereas younger sports patients can tolerate more aggressive anti-inflammatory therapy. This variation underscores the descriptive nature of the present review, as differences in pharmacological rationale, clinical pathways, and institutional resources preclude direct comparisons across studies. Differences in institutional analgesic policies, anesthetic practices, and the availability of adjunct modalities have further contributed to inconsistent regimens [64,65]. In essence, the multiplicity of systemic strategies represents a pragmatic clinical response to the complex and evolving challenge of balancing analgesic efficacy, opioid minimization, and safety across diverse patient groups. Local multimodal techniques offer another promising dimension. Peri-articular infiltration after TKA and intra-articular injection during arthroscopy or ligament reconstruction can deliver high drug concentrations at the surgical site while minimizing systemic exposure. The principle is well established, but the practical implementation varies widely. The included trials used numerous combinations of local anesthetics, alone or mixed with ketorolac, corticosteroids, morphine, or α_2_-agonists, applied in different volumes and at different tissue planes. Several studies have reported modest early analgesic effects, but consensus on the optimal composition and safety remains limited. Concerns about potential chondrotoxicity, delayed wound healing, and systemic absorption remain insufficiently studied [66]. To achieve comparability, future trials should adopt standardized infiltration mixtures, clearly define administration techniques, and include follow-up long enough to detect late complications. The goal should be to identify one or two reproducible, safe protocols that could be applied across knee procedures with minor adaptations.
Despite growing interest in multimodal regimens, non-pharmacological interventions remain notably under-represented in the literature. Only two TKA studies evaluated strategies such as music and continuous cold-flow therapy, while no trial addressed behavioral preparation, structured physiotherapy, or sleep optimization. This omission is striking, considering that enhanced recovery after surgery (ERAS) pathways emphasize multimodal, non-pharmacologic support to accelerate rehabilitation and reduce opioid need [67]. Non-drug measures can influence both the sensory and emotional components of pain and often improve patient satisfaction [68]. They are inexpensive, scalable, and rarely associated with harm [69]. Their limited inclusion suggests a persistent pharmacologic bias in trial design. These gaps highlight an opportunity for future trials to integrate non-pharmacological components more systematically and assess their additive value within multimodal pathways. Cold therapy, guided early mobilization, and patient education on realistic pain expectations could easily be standardized and tested across all knee procedures.
An important consideration is the evolving role of motor-sparing regional techniques in knee surgery, including adductor canal, iPACK, and genicular nerve blocks which have reduced the functional limitations traditionally associated with motor blockade in regional anesthesia [70]. These techniques, however, are time-limited, operator-dependent, and variably available, and they do not fully address central sensitization, inflammatory responses, or cognitive–emotional contributors to postoperative pain. In this context, non-regional analgesic strategies should be viewed as complementary rather than competitive, providing a scalable and broadly applicable foundation that ensures continuity of analgesia beyond block resolution. Notably, pain science education and expectation management were almost entirely absent from the included studies, despite their potential to improve pain perception, opioid use, and patient satisfaction [71]. Future research should therefore evaluate integrated perioperative approaches that combine non-regional multimodal analgesia, selective motor-sparing regional techniques when available, non-pharmacological interventions, and standardized functional outcome measures.
Another critical limitation identified in this review concerns the narrow scope of reported outcomes. Most trials assessed pain only within the first 24 h, typically using visual analogue scales at rest, with limited attention to pain during movement or rehabilitation. Functional such as range of motion, timed up-and-go, and time to independent walking, were primarily reported in TKA studies. They were rarely included in arthroscopy or CLMR trials (see File S3). The absence of standardized functional outcome domains further complicates cross-study interpretation, as measures differed in timing, definition, and clinical relevance. For younger and more active populations undergoing reconstructive procedures, functional recovery is a critical endpoint that has often been underrepresented. Adoption of standardized core outcome domains encompassing both pain and function would improve interpretability and clinical relevance. Incorporating measures such as quality of recovery, patient satisfaction, and readiness for rehabilitation would further ensure that postoperative pain research reflects outcomes meaningful to both clinicians and patients. Future research should move beyond isolated demonstrations of short-term analgesic benefit and instead focus on optimizing timing, duration, and patient selection while evaluating safety and functional recovery in parallel.
The heterogeneity observed across studies spanning differences in age groups, sex distribution, comorbidities, dosing regimens, and outcome measures highlights a persistent gap between controlled research settings and real-world clinical practice. Single-center studies, while valuable for of concept, often reflect the resources, routines, and patient populations of their institutions and therefore cannot be generalized [72]. Analgesic regimens are strongly influenced by local logistics, drug availability, staffing patterns, and departmental culture, which determine what is feasible rather than what is ideal [73]. Even when multicenter protocols exist, adherence may vary due to institutional policies on opioid prescribing, perioperative monitoring, or nursing workload [74]. Consequently, consensus guidelines and standardized pathways, though scientifically sound, often face practical barriers at the implementation level. Collaborative multicenter trials should preserve core methodological uniformity while allowing limited flexibility for local adaptation. Such pragmatism may partly explain the continued exploration of similar analgesic strategies across diverse settings.
Although most trials reported favorable short-term outcomes, the persistent proliferation of studies across different drug classes and modalities appears driven more by contextual and pragmatic motivations than by conflicting evidence. Variations in institutional practice and logistical constraints have repeatedly prompted investigators to test similar concepts in new configurations. This pattern reflects an ongoing effort to balance mechanistic rationale with real-world applicability, rather than genuine uncertainty regarding the efficacy of multimodal analgesic principles (Detailed study-level rationales and contextual motivations are summarized in File S4).
When the findings across systemic, local, and non-pharmacological domains are considered collectively, the evidence suggests a pragmatic rather than uniform approach to postoperative pain management in knee surgery. Systemic non-opioid therapy forms a consistent and evidence-based foundation, while local infiltration and non-pharmacological strategies provide variable but potentially additive benefits. However, the absence of standardized protocols, inconsistent reporting of functional outcomes, and methodological diversity across studies limit the ability to define a single optimal regimen applicable to all surgical contexts. Instead, the emerging consensus favors flexible multimodal combinations tailored to institutional logistics, patient characteristics, and surgical complexity. Such flexibility aligns with the descriptive purpose of this review and highlights the need for future standardized, comparative studies across knee surgery populations.
5. Conclusions
The evidence on non-regional postoperative analgesia in knee surgery is heterogeneous and unevenly distributed across procedures and study designs. Multimodal systemic strategies and pre-emptive NSAID use were frequently associated with lower early postoperative pain scores or reduced opioid consumption, although substantial variation in interventions and outcome reporting limits firm conclusions. Periarticular and intra-articular techniques were commonly applied as adjuncts to systemic regimens, reflecting their pragmatic role within multimodal pathways. As this scoping review focused on early postoperative outcomes, future research should adopt standardized pain and functional outcome measures and directly compare systemic and local multimodal approaches, while extending follow-up beyond the immediate postoperative period to better characterize sustained clinical relevance.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Grosu I. Lavand’homme P. Thienpont E. Pain after knee arthroplasty: An unresolved issue Knee Surg. Sports Traumatol. Arthrosc.2014221744175810.1007/s 00167-013-2750-224201900 · doi ↗ · pubmed ↗
- 2Price A.J. Alvand A. Troelsen A. Katz J.N. Hooper G. Gray A. Carr A. Beard D. Knee replacement Lancet 20183921672168210.1016/S 0140-6736(18)32344-430496082 · doi ↗ · pubmed ↗
- 3Wainwright T.W. Gill M. A Mc Donald D. Middleton R.G. Reed M. Sahota O. Yates P. Ljungqvist O. Consensus statement for perioperative care in total hip replacement and total knee replacement surgery: Enhanced Recovery After Surgery (ERAS®) Society recommendations Acta Orthop.20209131910.1080/17453674.2019.168379031663402 PMC 7006728 · doi ↗ · pubmed ↗
- 4Gan T.J. Poorly controlled postoperative pain: Prevalence, consequences, and prevention J. Pain Res.2017102287229810.2147/JPR.S 14406629026331 PMC 5626380 · doi ↗ · pubmed ↗
- 5Rhamelani P. Mahdhiya N.Z. Yoviana I. Jessica J. Komariah M. Early Mobilization in Post-Orthopedic Surgery Patients: A Scoping Review J. Multidiscip. Healthc.20251830531710.2147/JMDH.S 48323239866347 PMC 11761157 · doi ↗ · pubmed ↗
- 6Chan E.Y. Fransen M. Parker D.A. Assam P.N. Chua N. Femoral nerve blocks for acute postoperative pain after knee replacement surgery Cochrane Database Syst. Rev.20142014 CD 00994110.1002/14651858.CD 009941.pub 224825360 PMC 7173746 · doi ↗ · pubmed ↗
- 7Wang D. Yang Y. Li Q. Tang S.-L. Zeng W.-N. Xu J. Xie T.-H. Pei F.-X. Yang L. Li L.-L. Adductor canal block versus femoral nerve block for total knee arthroplasty: A meta-analysis of randomized controlled trials Sci. Rep.201774072110.1038/srep 4072128079176 PMC 5228345 · doi ↗ · pubmed ↗
- 8Fillingham Y.A. Hannon C.P. Kopp S.L. Austin M.S. Sershon R.A. Stronach B.M. Meneghini R.M. Abdel M.P. Griesemer M.E. Woznica A. The Efficacy and Safety of Regional Nerve Blocks in Total Knee Arthroplasty: Systematic Review and Direct Meta-Analysis J. Arthroplast.20223719061921 e 210.1016/j.arth.2022.03.07836162923 · doi ↗ · pubmed ↗