Design and Implementation of Observational Studies Emulating a Target Trial
Yan Ren, Yulong Jia, Lingyan Liu, Houchen Lyv, Liyuan Tao, Yuezhen Li, Peng Zhao, Yiquan Xiong, Guowei Li, Jiayue Xu, Chunrong Liu, Yongmei Lu, Kang Zou, Jing Tan, Xin Sun

TL;DR
This study examines how target trial emulation is used in clinical research, identifies common scenarios and methodological issues, and offers a framework to improve its reliability.
Contribution
A structured framework and practical recommendations for improving target trial emulation methods in observational studies.
Findings
Target trial emulation was applied in eight recurring clinical scenarios, including drug interventions and extending evidence to underrepresented populations.
Major methodological gaps were identified, such as low adherence to prespecified protocols and poor justification for trial emulation choices.
A five-step framework was proposed to address these gaps and improve the credibility of observational evidence.
Abstract
This cross-sectional analysis of studies using target trial emulation assesses clinical scenarios in which this approach has been applied, identifies common methodologic challenges, and proposes a structured framework for rigorous target trial design. In which clinical scenarios has target trial emulation (TTE) been applied, and how well do TTE studies adhere to key principles of target trial design and implementation? In this cross-sectional analysis of 237 TTE studies (2017-2023), 8 recurring clinical scenarios and substantial variation in design quality and methodologic implementation were identified. A structured framework and practical recommendations were proposed to address these gaps. These findings highlight the need to improve methodologic rigor in TTE, and the provided recommendations complement the Transparent Reporting of Observational Studies Emulating a Target Trial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
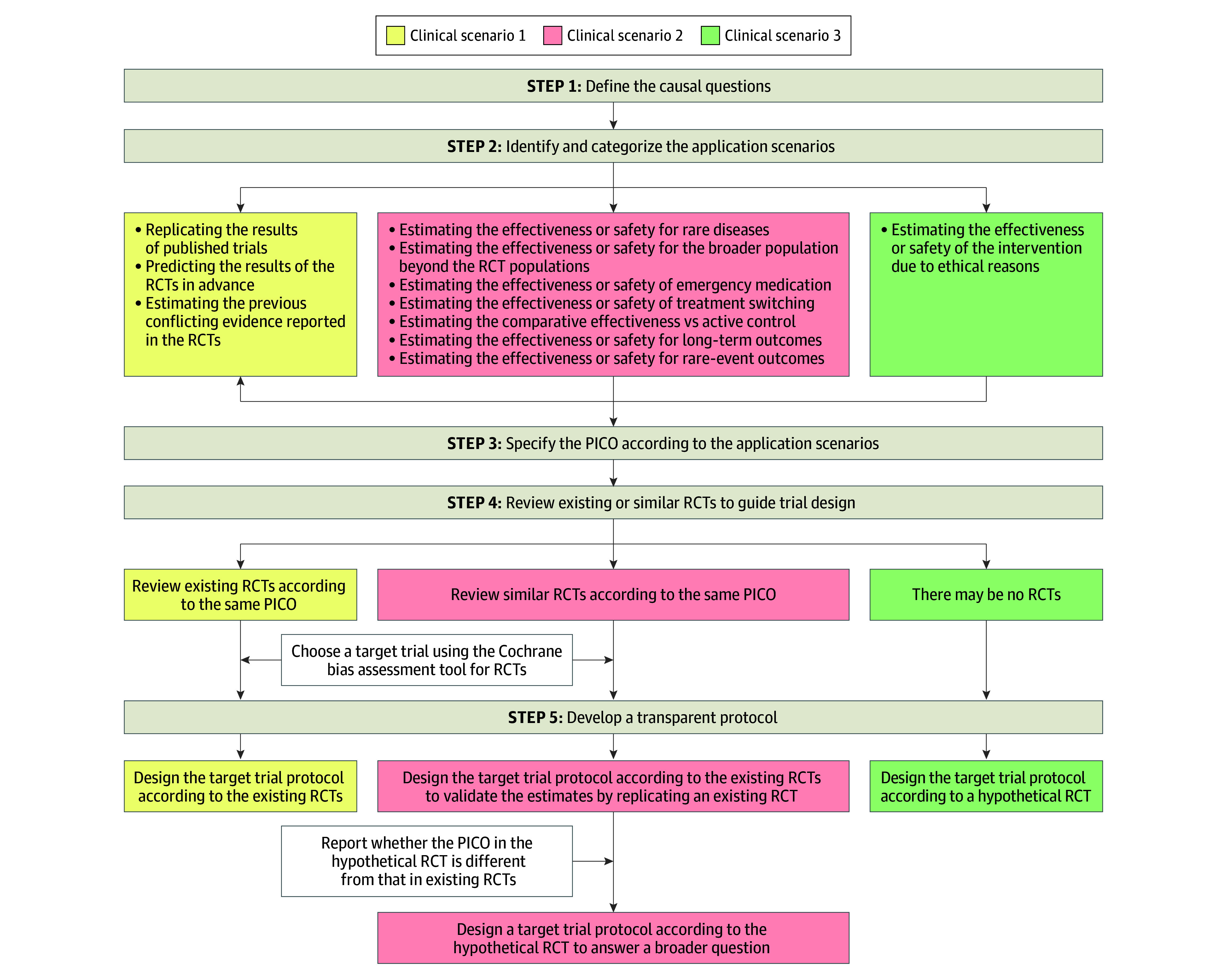 Figure 1
Figure 1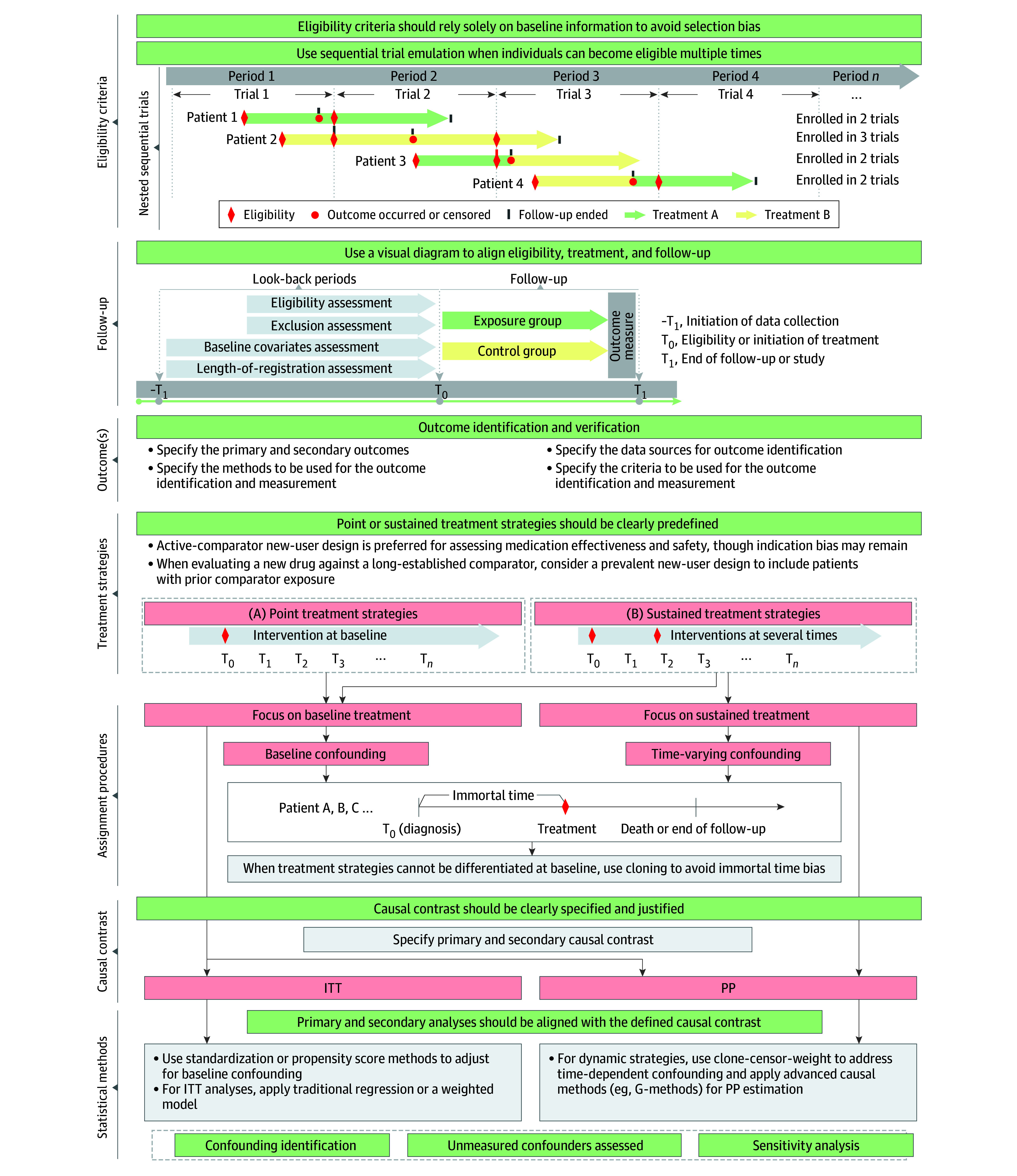 Figure 2
Figure 2| Variable | Studies, No. (%) (N = 237) |
|---|---|
| Target disease | |
| Infectious diseases (COVID-19, HIV, and others) | 59 (24.9) |
| Cardiology (cardiovascular diseases) | 33 (13.9) |
| Oncology | 25 (10.5) |
| Endocrinology (diabetes and other diseases) | 19 (8.0) |
| Neurology (cerebrovascular diseases) | 6 (2.5) |
| Rheumatology | 9 (3.8) |
| Psychiatry | 7 (3.0) |
| Kidney disease | 9 (3.8) |
| Orthopedic diseases | 5 (2.1) |
| Obstetrics and gynecology | 5 (2.1) |
| Critical care medicine | 5 (2.1) |
| Other | 23 (9.7) |
| No specified disease | 32 (13.5) |
| Type of intervention | |
| Drug | 128 (54.0) |
| Vaccine | 25 (10.5) |
| Surgical | 21 (8.9) |
| Behavioral | 16 (6.8) |
| Other | 47 (19.8) |
| Type of control | |
| Standard care | 38 (16.0) |
| Blank control | 93 (39.2) |
| Active control | 119 (50.2) |
| Other | 4 (1.7) |
| Primary outcome | |
| All-cause mortality | 102 (43.0) |
| Disease-specific mortality | 19 (8.0) |
| Cardiovascular major morbid events | 38 (16.0) |
| Other major morbid events (eg, loss of vision, seizures, fracture, revascularization) | 53 (22.4) |
| Onset, recurrence, relapse, and/or remission of cancer and other chronic diseases (eg, COPD exacerbation) | 21 (8.9) |
| Hospitalization | 31 (13.1) |
| Infections | 24 (10.1) |
| Symptoms, quality of life, and functional status | 18 (7.6) |
| Laboratory examination | 16 (6.8) |
| Other | 6 (2.5) |
| Type of primary outcome | |
| Continuous | 12 (5.1) |
| Ordinal | 1 (0.4) |
| Binary | 72 (30.4) |
| Time-to-event | 153 (64.6) |
| Other | 3 (1.3) |
| Variable | Studies, No. (%) (N = 237) |
|---|---|
| What did the study aim to evaluate? | |
| Effectiveness | 165 (69.6) |
| Safety | 56 (23.6) |
| Safety and effectiveness | 15 (6.3) |
| Cost-effectiveness | 1 (0.4) |
| Which scenario did the emulated trial present? | |
| Replicating the results of a published trial in an actual clinical setting | 22 (9.2) |
| Predicting the results of the RCTs in advance | 5 (2.1) |
| Estimating the previous conflicting results reported in studies | 46 (19.4) |
| Estimating the effectiveness or safety of emergency medication (eg, COVID-19 drug) | 42 (17.7) |
| Estimating the comparative effectiveness vs active control | 49 (20.7) |
| Estimating the effectiveness of treatment switching | 5 (2.1) |
| Estimating the effectiveness or safety for a long-term outcome | 39 (16.5) |
| Estimating the safety for a rare-event outcome | 8 (3.4) |
| Estimating the effectiveness or safety for rare diseases | 4 (1.7) |
| Estimating the effectiveness or safety for the broader population | 21 (8.9) |
| Lacking RCT evidence | 35 (14.8) |
| Estimating the effectiveness or safety in an actual clinical setting | 19 (8.0) |
| Other | 20 (8.4) |
| What types of treatment strategies did the target trial emulation focus on? | |
| Point treatment strategies | 98 (41.4) |
| Static sustained treatment strategies | 128 (54.0) |
| Dynamic sustained treatment strategies | 11 (4.6) |
| What types of treatment strategies did the target trial emulation compare? | |
| Head-to-head comparison of ≥2 active treatments (A vs B) | 125 (52.7) |
| Single active treatment vs no treatment (A vs none) | 98 (41.4) |
| Combination treatment vs 1 active treatment (A + B vs A) | 18 (7.6) |
| Combination treatment vs no treatment (A + B vs none) | 2 (0.8) |
| Other | 10 (4.2) |
| Variable | Studies, No. (%) (N = 237) |
|---|---|
| Has the research protocol been registered? | |
| Yes | 40 (16.9) |
| No | 197 (83.1) |
| Was a target trial protocol made? | |
| Yes | 134 (56.5) |
| No | 103 (43.5) |
| How many target trials were emulated in this study? | |
| 1 | 175 (73.8) |
| 2 | 21 (8.9) |
| ≥3 (please specify) | 16 (6.8) |
| Not reported | 25 (10.5) |
| If ≥1 target trial was conducted, what was the reason? | |
| Different intervention, No. /total No. (%) | 18/37 (48.6) |
| Different primary outcome, No. /total No. (%) | 1/37 (2.7) |
| Different population, No. /total No. (%) | 14/37 (37.8) |
| Other, No. /total No. (%) | 6/37 (16.2) |
| How many arms were compared in target trials? | |
| 1 | 8 (3.4) |
| 2 | 162 (68.4) |
| 3 | 13 (5.5) |
| 4 | 6 (2.5) |
| >4 | 8 (3.4) |
| Not reported | 40 (16.9) |
| Did the researcher review existing RCTs for the target trial? | |
| Yes | 110 (46.4) |
| No | 127 (53.6) |
| Which type of target trial was the study planned to emulate? | |
| Existing complete RCT | 26 (11.0) |
| Existing ongoing RCT | 5 (2.1) |
| Hypothetical RCT | 105 (44.3) |
| May be a hypothetical RCT | 48 (20.3) |
| Not specified | 53 (22.4) |
| If the emulated trial was an existing RCT, did the researcher give the reason for selecting this RCT as the target trial? | |
| Yes, No./total No. (%) | 11/31 (35.5) |
| No, No./total No. (%) | 20/31 (64.5) |
| If the emulated trial was a hypothetical RCT, did the researcher give the reference standards for defining such a trial? | |
| Yes, No./total No. (%) | 6/153 (3.9) |
| No, No./total No. (%) | 147/153 (96.1) |
| Which type of RCT was the study claimed to emulate? | |
| Parallel RCT | 33 (13.9) |
| Cluster RCT | 4 (1.7) |
| Pragmatic trial | 49 (20.7) |
| Other | 4 (1.7) |
| Not specified | 147 (62.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdvanced Causal Inference Techniques · Meta-analysis and systematic reviews · Genetic Associations and Epidemiology
Introduction
Target trial emulation (TTE) is an increasingly adopted framework for estimating causal effects using observational data.^1,2^ By explicitly mimicking a hypothetical randomized clinical trial (RCT), TTE aims to reduce bias and enhance the credibility of observational studies.^3,4,5,6^ The methodologic foundation was established by Hernán and Robins,^7,8^ and the empirical validity from the RCT DUPLICATE initiative^9^ has accelerated the uptake of TTE across diverse domains, including infectious diseases, cancer, and cardiovascular research.^10,11,12,13,14,15,16^
Despite the growing popularity of TTE, important uncertainties remain. It is not fully understood in which clinical scenarios TTE has been applied or whether such applications are always conceptually appropriate. A distinguishing feature of TTE, in contrast to traditional observational studies, is the emphasis on explicitly defining a target trial aligned with the research purpose.^17^ However, methodologic guidance on how to design such trials remains underdeveloped.
Several efforts have contributed to improving the conduct and reporting of TTE. Methodologic studies have addressed specific challenges, such as avoiding immortal time bias,^18,19^ selecting appropriate comparators,^20^ or implementing sustained treatment strategies through techniques such as cloning or censoring.^21,22,23,24,25,26^ Previous reviews have also examined reporting quality, specific biases, clinical disease areas, or specific components of TTE implementation.^27,28,29,30,31^ Most recently, the Transparent Reporting of Observational Studies Emulating a Target Trial (TARGET) reporting guideline introduced a structured checklist to enhance reporting clarity and reproducibility.^32^ However, TARGET focuses on what should be reported rather than how target trials should be designed or technically executed. Likewise, existing reviews do not offer context-specific, practice-oriented recommendations for designing and implementing TTE studies across diverse clinical scenarios.
To address these gaps, we conducted a cross-sectional methodologic survey of published TTE studies. Our objectives were to (1) characterize the clinical scenarios in which TTE has been applied, (2) evaluate the specification and implementation of target trials, and (3) identify common methodologic challenges. Building on these findings, we propose a structured, scenario-based framework for target trial design and provide practical recommendations for applying the 7 core methodologic elements essential for rigorous TTE.
Methods
The protocol of this cross-sectional study was registered on the Open Science Framework website.^33^ Given that the unit of analysis comprised published studies, ethics approval and informed consent were not applicable. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Data Sources
We systematically searched PubMed to identify TTE studies published between January 1, 2017, and December 15, 2023. To ensure quality, we restricted the search to studies published in Journal Impact Factor quartile 1 journals under the “clinical medicine” category of the Journal Citation Reports. We used a combination of MeSH terms and keywords related to TTE, such as target trial**, emulat trial**, and trial emulat**, to search for potentially eligible studies (eAppendix 1 in Supplement 1). To ensure comprehensiveness, we also screened eligible studies from 3 previously published scoping and systematic reviews on TTE.^27,28,29^
Eligibility Criteria
We included original studies that explicitly stated the use of “target trial emulation” or clearly indicated the emulation of a trial using observational data. We excluded studies that met any of the following criteria: (1) case report or series, editorial, letter, commentary, study protocol, abstract, systematic review, meta-analysis, or randomized controlled study; (2) not published in English; (3) methodologic study discussing TTE without applying it; or (4) only mentioned the concept of trial emulation—such as in sensitivity analyses or as part of confounding control—without explicitly identifying the study as a TTE.
Study Selection
We used a predesigned, machine learning–assisted framework—fuzzy population–intervention study design (fPIS) combined with gradient boosting decision tree ensemble modeling—to assist in identifying eligible TTE studies (eAppendix 2 in Supplement 1). The algorithm analyzed full-text content to classify articles as “yes” (a TTE study) or “no” (not a TTE study). Two researchers (Y.R., Y.J.) trained in clinical epidemiology and TTE independently screened full texts for studies classified as “yes” and a randomly selected subset of “no” classifications to minimize false negatives. Disagreements were resolved through discussion or, if needed, adjudication by a third investigator (J.T.).
Questionnaire Development and Data Extraction
We developed a standardized data extraction form based on relevant methodologic literature.^3,4,7,8,27,28,29,34,35,36,37^ The initial draft was created by 2 researchers (Y.R., Y.J.) and reviewed by a panel of 6 domain experts (H.L., L.T., Y.X., J.X., J.T., X.S.). The form was refined following pilot testing on 20 studies and consensus discussion. The final form (eAppendix 3 in Supplement 1) included 5 domains: general study characteristic; population, intervention, control, and outcome (PICO) elements; clinical scenarios; target trial design characteristics; and implementation of core methodologic components.
All investigators (Y.R., Y.J., L.L., Yuezhen L., P.Z., Y.X.) were trained on the definitions and procedures. To ensure consistency, each investigator conducted a pilot extraction on 5 studies, with discrepancies discussed as a group. Each article was independently extracted by 1 reviewer (Y.J., Yuezhen L., P.Z., or Y.X.) and verified by a second reviewer (Y.R., Y.J., or L.L.) with expertise. If multiple TTEs were presented within a single article, we collected information regarding only the first reported emulation; if several target trials were emulated within a single article, we collected information regarding only the first reported target trial.
Recommendations Development
We designed a structured questionnaire and conducted an expert consensus process to develop recommendations for the design and implementation of TTE studies. First, we generated candidate recommendations based on the findings from our survey of methods in TTE research and related methodologic studies. Next, we designed a structured consultation questionnaire (eAppendix 4 in Supplement 1). Then, we invited 22 experts from multidisciplinary fields—including TTE, epidemiology, statistics, clinical trials, and clinical medicine—who had experience conducting observational studies or TTE research to participate in the expert consensus process. Subsequently, 6 additional external experts were invited to independently evaluate the scenario-based framework.
Statistical Analysis
Descriptive analysis was used to summarize the study characteristics. Categorical variables were presented as frequencies and percentages. Continuous variables were reported as means with SDs or medians with IQRs, as appropriate. All analyses were conducted using SAS software, version 9.4 (SAS Institute Inc).
Results
A total of 46 986 records were identified through the PubMed search. After automated screening using the fPIS–machine learning technique, 46 024 records were excluded. The remaining 962 records underwent manual eligibility assessment. An additional 334 records were retrieved from the 3 previous scoping reviews on TTE.^27,28,29^ In total, 237 records met the eligibility criteria and were included in the final analysis^6,10,15,19,21,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184,185,186,187,188,189,190,191,192,193,194,195,196,197,198,199,200,201,202,203,204,205,206,207,208,209,210,211,212,213,214,215,216,217,218,219,220,221,222,223,224,225,226,227,228,229,230,231,232,233,234,235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256,257,258,259,260,261,262,263,264,265,266,267,268,269^ (eFigure 1 in Supplement 1).
The expert panel consisted of 22 multidisciplinary specialists from 4 countries, primarily in fields of epidemiology and statistics. Eleven (50.0%) held senior academic titles, 5 (22.7%) had published TTE studies, and 11 (50.0%) had participated in TTE-related research. All panelists were familiar with TTE methods.
General Characteristics
The number of published TTE studies increased steadily from 2017 to 2023, with a marked rise beginning in 2021 (eFigure 2 in Supplement 1). Corresponding authors were most commonly based in the US (98 [41.4%]). As shown in eTable 1 in Supplement 1, most studies used a retrospective cohort design (207 [86.4%]), and nearly half (118 [49.8%]) relied on electronic medical records. National-level data sources were used in 175 studies (73.8%). The median analyzed sample size was 11 200 (IQR, 2381-106 112). Methodologists were involved in 193 studies (81.4%), and 197 (83.1%) reported receiving financial support.
PICO Elements
As shown in Table 1, the most common disease areas were infectious diseases (59 studies [24.9%]), cardiology (33 [13.9%]), and oncology (25 [10.5%]). More than half of the studies (128 [54.0%]) evaluated drug interventions. In comparator selection, 119 studies (50.2%) used active controls and 38 (16.0%) used standard care. All-cause mortality was the most frequently examined primary outcome (102 studies [43.0%]). Most outcomes (153 studies [64.6%]) were measured on a time-to-event scale.
Objectives and Application Scenarios
Most studies (165 [69.6%]) aimed to evaluate treatment effectiveness. We identified 8 clinical scenarios in which TTE was applied. The application scenarios addressed were heterogenous. A minority of studies focused on broader populations beyond RCT eligibility (21 [8.9%]) or on rare diseases (4 [1.7%]). Regarding intervention contexts, 42 studies (17.7%) evaluated emergency-use medications (eg, COVID-19 treatments), 49 (20.7%) assessed active-treatment comparisons, and 5 (2.1%) focused on treatment switching. For outcomes, 39 studies (16.5%) examined long-term effects and 8 (3.4%) evaluated rare-event outcomes. Additionally, 46 (19.4%) addressed settings with conflicting prior evidence, 35 (14.8%) examined questions lacking RCT evidence, and 19 (8.0%) estimated the results in actual clinical settings, while 22 (9.2%) attempted RCT replication and 5 (2.1%) aimed to predict future trial results (Table 2).
Over half of the studies (128 [54.0%]) evaluated static sustained treatment strategies, 98 (41.4%) examined point treatment strategies, and 11 (4.6%) examined dynamic strategies. Treatment comparisons frequently involved head-to-head comparisons (125 [52.7%]) and a single active treatment compared with no treatment (98 [41.4%]).
Methodologic Characteristics of Target Trial Design
As shown in Table 3, only 40 studies (16.9%) reported prospective protocol registration, and 134 (56.5%) explicitly developed a target trial protocol. More than half (127 [53.6%]) did not review existing RCTs during trial specification. Among the included studies, 31 (13.1%) emulated existing RCTs, while 153 (64.6%) emulated hypothetical trials; however, most of those (20 of 31 [64.5%] and 147 of 153 [96.1%], respectively) did not justify their choice of trial to emulate. Twenty-seven studies (11.4%) reported trials with more than 2 arms, and 37 studies (15.7%) emulated 2 or more target trials, primarily due to variations in interventions or populations.
Methodologic Characteristics of TTE Implementation
Overall, 103 studies (43.5%) did not report all 7 core components of TTE (eTable 2 in Supplement 1). Inconsistencies between the emulated and target trials were reported in eligibility criteria (37 studies [15.6%]), treatment strategies (20 [8.4%]), and outcome definitions (10 [4.2%]). Thirty-six studies (15.2%) used postbaseline information inappropriately for eligibility determination, and 42 (17.7%) did not include flowcharts describing eligibility processes. Only 35 studies (14.8%) used a sequential design with multiple eligibility time points. Regarding treatment strategy design, 93 studies (39.2%) did not use active comparators, and 71 (30.0%) adopted new user design. Only 37 (15.6%) explicitly assessed the quality of the outcome.
Most studies (158 [66.7%]) reported efforts to emulate randomization, and 29 of those (18.4%) applied cloning techniques in scenarios where cloning was appropriate. Few studies (40 [16.9%]) provided follow-up diagrams to define time zero. Most studies (106 of 161 [65.8%]) described the causal contrast in the target trial as an intention-to-treat (ITT) analysis, while the emulated trial often used a per-protocol (PP) approach (eFigure 3 in Supplement 1). Although 185 studies (78.1%) conducted sensitivity analyses, only 73 (30.8%) used statistical methods to assess the impact of unmeasured confounding.
A Structured Framework for Designing Target Trials
To enhance consistency and rigor in target trial specification, we developed a 5-step framework (Figure 1 and eAppendix 5 in Supplement 1). Step 1 is to define the causal questions and intervention effect of interest. Step 2 is to identify and categorize the application scenario into 3 types: (1) replication or prediction of RCT findings in clinical settings; (2) extension of evidence to new populations, rare outcomes, or treatment switching; or (3) settings where RCTs are infeasible due to ethical or logistic constraints. Step 3 is to specify all PICO elements to ensure alignment between purpose and design. Step 4 is to review existing or similar RCTs to guide trial design, with 3 scenarios: (1) emulate an existing RCT with matched PICO, (2) consult similar RCTs to inform a hypothetical trial specification, or (3) justify the design choices based on clinical reasoning when RCT evidence is absent. Step 5 is to develop a transparent protocol, which should explicitly describe all key components, including eligibility criteria, treatment strategies, assignment procedures, follow-up, outcomes, causal contrast, and the statistical analysis plan. For the second scenario in step 4, 2 protocols may be considered: 1 to replicate existing RCTs and 1 to address novel questions, as previously suggested.^6^
Diagram of the Recommended Framework to Design a Target Trial According to the Clinical ScenarioPICO indicates population, intervention, control, and outcome; RCT, randomized clinical trial.
Considerations for Implementing TTE Methods
Drawing on identified gaps, we outline practical considerations for implementing the 7 core methodologic components of TTE (Figure 2 and eAppendix 5 in Supplement 1). First, eligibility criteria are generally expected to rely on information available at baseline to avoid selection bias. Sequential trial emulation is recommended when individuals become eligible multiple times during follow-up. Second, treatment strategies may benefit from adopting an active comparator new-user design. Point or sustained treatment strategies should be clearly predefined. Third, assignment procedures may be strengthened through analytic approaches (eg, propensity score matching, G-methods) to emulate randomization. Depending on the type of treatment strategy, different methods may be appropriate. Fourth, follow-up can be more clearly communicated using a visual design diagram that illustrates the alignment of eligibility, treatment initiation, and follow-up at time zero. Fifth, outcomes are ideally prespecified, with clear documentation of definitions, data sources, and any validation procedures to support outcome accuracy and relevance. Sixth, causal contrast (ITT or PP) should be clearly stated and contextually justified based on the research question and the type of treatment strategy. Seventh, statistical methods should be aligned with the defined causal contrast and might include techniques to explore or adjust for unmeasured confounding and sensitivity analyses to assess the robustness of findings. For dynamic treatment strategies, we recommend using the clone-censor-weight approach for time-dependent confounding and immortal time bias and using causal inference methods such as G-methods or doubly robust estimators to quantify treatment effects.
Diagram of the Methodologic Recommendation for Implementing a Target Trial Emulation StudyITT indicates intention to treat; PP, per protocol; T, time.
Discussion
Summary of Main Findings
In this survey of 237 published TTE studies, we observed a rapid increase in their use since 2021, which may reflect both the growing recognition of observational evidence and the substantial expansion of COVID-19–related research—consistent with prior findings that approximately 20% of TTE publications between 2020 and 2021 addressed COVID-19 questions.^29^ Most studies focused on pharmacologic treatment effectiveness and were conducted primarily in high-income countries using national or large-scale electronic health records. We identified 8 recurrent clinical scenarios in which TTE has been applied, ranging from RCT replication to extending evidence to underrepresented populations or rare outcomes. These findings suggest that TTE has become a versatile tool to complement RCTs, particularly in settings where trials are infeasible, underpowered, or ethically challenging. However, observed misuse of the framework in evaluating nonmodifiable exposures^117,171,242^ underscores the need for clearer conceptual boundaries.
Despite increasing adoption, major gaps remain in how target trials are designed. Fewer than 1 in 5 studies included in this cross-sectional survey prospectively registered a protocol, and nearly half did not explicitly develop a target trial protocol. More than half did not review existing RCTs before designing their target trial, and many failed to clarify whether they emulated a hypothetical or existing RCT. These shortcomings undermine transparency, reproducibility, and the interpretability of causal claims. Our proposed 5-step framework addresses these issues by emphasizing a priori protocol development, systematic use of the PICO framework, and explicit consideration of prior RCTs when defining the target trial.
The 7 core methodologic items of the TTE framework are key points for achieving causal inference through control bias.^36,242,270^ However, deviations from the 7 core methodologic elements of TTE were also common. Examples included the inappropriate use of postbaseline information for eligibility, inadequate description or implementation of procedures intended to emulate randomization, and inconsistent specification of time zero. Fewer than one-third of studies assessed the influence of unmeasured confounding, and fewer than one-fifth used visual diagrams to clarify follow-up design. These limitations pose risks of systematic bias and weaken causal inference, particularly in comparative effectiveness research. Strengthening TTE practice therefore requires both adherence to established principles (eg, active-comparator new-user designs) and broader adoption of causal inference methods, including cloning, censoring, and advanced sensitivity analyses.^35,54,271^
Comparison With Other Studies
Previous methodologic reviews have examined reporting practices, specific biases, or selected clinical areas,^27,28,29,30,31^ although none provided a comprehensive evaluation across application scenarios or offered practice-oriented guidance for designing and implementing a TTE. Existing methodologic commentaries have proposed recommendations within specific contexts, such as diabetes, critical care, and rehabilitation,^272,273^ but they did not articulate a generalizable framework for target trial design.
The recently published TARGET guideline represents an important advancement by standardizing reporting for observational studies emulating a target trial.^32^ Its primary focus is on what should be reported to enhance clarity and reproducibility. However, TARGET does not offer technical guidance on how to specify or operationalize the target trial, nor does it provide scenario-specific recommendations for implementing TTE in practice.
In contrast, our study addressed gaps not covered by TARGET or prior reviews. Our 5-step framework and methodologic considerations are intended to guide the design and implementation of TTE studies before reporting occurs. The 5-step framework focuses on upstream design decisions—defining the causal question, identifying the clinical scenario, specifying PICO, reviewing existing or similar RCTs to guide trial design, and developing a transparent protocol. Our accompanying recommendations expand the 7 methodologic elements by offering operational, practice-oriented guidance for implementation, including handling multiple eligibility time points, selecting appropriate comparators, determining time zero, and applying cloning or censoring when warranted. Thus, TARGET and our recommendations play complementary but distinct roles: TARGET strengthens reporting, whereas our framework strengthens design quality and methodologic rigor, thereby supporting more credible and reproducible TTE research.
Strengths and Limitations
This study has several strengths. We conducted a systematic evaluation of both clinical applications and methodologic rigor of TTE across a wide range of disease areas. The large and diverse sample enhances generalizability, and the integration of prior methodologic literature allowed us to develop practical, scenario-specific recommendations. Nonetheless, limitations should be noted. We included studies published between 2017 and 2023 in clinical journals with a Journal Impact Factor in quartile 1, which may not reflect the most recent developments or practices in lower-tier outlets. Our analysis relied on reported information, and unreported methodologic decisions could lead to underestimation of actual practice quality. In addition, we did not conduct a formal applicability assessment for the proposed recommendations.
Conclusions
In this cross-sectional study, we documented the growing use of TTE for estimating causal effects in contexts where randomized trials are impractical, unethical, or unavailable. However, we identified substantial and persisting heterogeneity in how target trials were defined and how core methodologic elements were implemented. Our study highlights the need to improve clarity, transparency, and methodologic rigor in both the design and execution of TTE. By proposing a structured framework for target trial specification and outlining practical considerations for implementation, we aimed to complement existing reporting standards and contribute to more robust, credible, and reproducible TTE research.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rasouli B, Chubak J, Floyd JS, . Combining high quality data with rigorous methods: emulation of a target trial using electronic health records and a nested case-control design. BMJ. 2023;383:e 072346. doi:10.1136/bmj-2022-072346 38154827 · doi ↗ · pubmed ↗
- 2Dib BN, Swanson SA. Emulating a target trial using observational data. JAMA Intern Med. 2025;185(4):459-460. doi:10.1001/jamainternmed.2024.8129 39992643 · doi ↗ · pubmed ↗
- 3Usman MS, Pitt B, Butler J. Target trial emulations: bridging the gap between clinical trial and real-world data. Eur J Heart Fail. 2021;23(10):1708-1711. doi:10.1002/ejhf.2331 34383997 · doi ↗ · pubmed ↗
- 4Matthews AA, Danaei G, Islam N, Kurth T. Target trial emulation: applying principles of randomised trials to observational studies. BMJ. 2022;378:e 071108. doi:10.1136/bmj-2022-071108 36041749 · doi ↗ · pubmed ↗
- 5Liang X, Zhang D, Wang H, . Importance of cohort and target trial emulation in clinical research. Cell Rep Med. 2025;6(4):102081. doi:10.1016/j.xcrm.2025.102081 40239630 PMC 12047467 · doi ↗ · pubmed ↗
- 6Matthews AA, Dahabreh IJ, Fröbert O, . Benchmarking observational analyses before using them to address questions trials do not answer: an application to coronary thrombus aspiration. Am J Epidemiol. 2022;191(9):1652-1665. doi:10.1093/aje/kwac 098 35641151 PMC 9437817 · doi ↗ · pubmed ↗
- 7Hernán MA, Wang W, Leaf DE. Target trial emulation: a framework for causal inference from observational data. JAMA. 2022;328(24):2446-2447. doi:10.1001/jama.2022.21383 36508210 · doi ↗ · pubmed ↗
- 8Hernán MA, Robins JM. Using big data to emulate a target trial when a randomized trial is not available. Am J Epidemiol. 2016;183(8):758-764. doi:10.1093/aje/kwv 254 26994063 PMC 4832051 · doi ↗ · pubmed ↗