Long-Term Outcomes Associated With Posterior Fossa Syndrome in Survivors of Childhood Medulloblastoma
Supriya Sarvode, Rikeenkumar Dhaduk, Yan Chen, Siddhant Taneja, Johnnie K. Bass, Robyn Partin, Kristin Szymanek, Matthew Wogksch, Heather M. Conklin, Darcy Raches, Thomas E. Merchant, Paul Klimo, Amar Gajjar, Kevin R. Krull, Raja B. Khan, Gregory T. Armstrong, Kirsten K. Ness

TL;DR
This study shows that children who survive medulloblastoma and develop posterior fossa syndrome face lasting cognitive and physical challenges, highlighting the need for better surgical techniques and long-term support.
Contribution
The study provides the first long-term evaluation of posterior fossa syndrome's impact on survivors of childhood medulloblastoma.
Findings
Posterior fossa syndrome is linked to significant deficits in attention, processing speed, and cognitive flexibility.
Survivors with posterior fossa syndrome are more likely to need help with daily tasks due to physical and cognitive impairments.
The syndrome's effects persist despite recovery from acute symptoms, emphasizing the need for improved surgical and postoperative care.
Abstract
What are the long-term outcomes associated with posterior fossa syndrome in survivors of childhood medulloblastoma? In this cohort study of 158 survivors of medulloblastoma 5 or more years from diagnosis, 23% developed posterior fossa syndrome. Compared with participants without posterior fossa syndrome, those with posterior fossa syndrome had significant deficits in attention, processing speed, and cognitive flexibility, and physical function and were more likely to require assistance with routine needs. This cohort study found that posterior fossa syndrome was associated with lasting neurocognitive and physical deficits in survivors of medulloblastoma, emphasizing the need for strategies to minimize surgical morbidity, continued interventions, and support in this high-risk population to improve outcomes among survivors. This cohort study evaluates the long-term neurological,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Participants, No. (%) | ||
|---|---|---|---|
| Posterior fossa syndrome (n = 37) | No posterior fossa syndrome (n = 121) | ||
| Sex | |||
| Female | 12 (32.4) | 50 (41.3) | .33 |
| Male | 25 (67.6) | 71 (58.7) | |
| Age, median (range), y | |||
| At diagnosis | 7.5 (3.2-17.4) | 9.1 (3.0-22.3) | .13 |
| At assessment | 24.5 (14.6-43.2) | 25.0 (10.8-44.3) | .96 |
| Time from diagnosis, median (range), y | 18.4 (9.1-31.9) | 14.2 (7.8-33.1) | .17 |
| Craniospinal radiation, Gy | |||
| <30 | 19(51.4) | 65(53.7) | .80 |
| ≥30 | 18(48.6) | 56(46.3) | |
| Race and ethnicity | |||
| Other | 8 (21.6) | 35 (28.9) | .38 |
| White non-Hispanic | 29 (78.4) | 86 (71.1) | |
| Surgical resections, No. | |||
| 1 | 22 (59.5) | 91 (75.2) | .06 |
| >1 | 15 (40.5) | 30 (24.8) | |
| Extent of resection | |||
| Gross total resection | 25 (67.6) | 96 (79.3) | .14 |
| Subtotal resection | 16 (43.2) | 35 (28.9) | .10 |
| Biopsy only | 1 (2.7) | 5 (4.13) | .38 |
| Shunt | 22 (59.5) | 36 (29.8) | .001 |
| BMI >25 | 13 (35.1) | 68 (56.2) | .02 |
| Domain / Outcome | Mean (SD) score | Difference in | ||
|---|---|---|---|---|
| Posterior fossa syndrome (n = 37) | No posterior fossa syndrome (n = 121) | |||
| Attention | ||||
| Focused attention | −2.7 (1.45) | −1.1 (1.70) | −1.04 (−1.62 to −0.45) | <.001 |
| Sustained attention | −1.2 (1.76) | −0.5 (1.44) | −0.45 (−1.07 to 0.16) | .15 |
| Variability | −0.8 (1.50) | −0.4 (1.23) | −0.16 (−0.69 to 0.37) | .54 |
| Processing speed | ||||
| Motor processing speed | −3.3 (1.15) | −2.2 (1.50) | −0.62 (−1.16 to −0.09) | .02 |
| Visuomotor processing speed | −2.3 (0.83) | −1.3 (0.93) | −0.65 (−0.97 to −0.33) | <.001 |
| Executive function | ||||
| Cognitive flexibility | −3.4 (1.20) | −1.9 (1.77) | −0.85 (−1.44 to −0.27) | .005 |
| Verbal fluency | −1.4 (1.03) | −0.7 (1.18) | −0.42 (−0.86 to 0.02) | .06 |
| Self-monitoring | −0.6 (1.16) | −0.3 (1.20) | −0.22 (−0.68 to 0.24) | .35 |
| General intelligence | ||||
| Full-scale IQ | −1.2 (1.21) | −0.8 (1.07) | −0.06 (−0.45 to 0.33) | .75 |
| Nonverbal reasoning | −1.1 (1.17) | −0.7 (1.08) | −0.11 (−0.52 to 0.29) | .57 |
| Vocabulary and verbal reasoning | −1.0 (1.16) | −0.8 (1.07) | 0.00 (−0.39 to 0.38) | .99 |
| Academics | ||||
| Mathematics | −1.6 (1.37) | −1.3 (1.24) | 0.07 (−0.36 to 0.50) | .75 |
| Reading | −1.3 (1.24) | −0.8 (1.07) | −0.27 (−0.67 to 0.13) | .18 |
| Memory | ||||
| Verbal learning | −1.3 (1.32) | −1.0 (1.28) | −0.16 (−0.66 to 0.35) | .54 |
| Short-term memory | −0.9 (0.99) | −0.8 (1.08) | 0.01 (−0.40 to 0.41) | .97 |
| Long-term memory | −1.3 (1.39) | −0.9 (1.28) | −0.23 (−0.74 to 0.29) | .39 |
| Visual memory | −1.9 (1.33) | −1.3 (1.30) | −0.44 (−0.96 to 0.07) | .09 |
| Working memory | −1.1 (1.02) | −0.6 (1.06) | −0.25 (−0.66 to 0.15) | .21 |
| NCQ self-report | ||||
| Memory | 1.2 (1.04) | 1.4 (1.39) | −0.33 (−0.88 to 0.23) | .24 |
| Task efficiency | 1.7 (1.09) | 1.1 (1.31) | 0.23 (−0.28 to 0.75) | .37 |
| Emotional regulation | 0.5 (1.01) | 0.3 (1.13) | 0.06 (−0.38 to 0.51) | .77 |
| Organization | 0.5 (0.98) | 0.3 (1.03) | 0.23 (−0.21 to 0.67) | .30 |
| Variable | Mean (SD) | Adjusted mean difference, β (95% CI) | ||
|---|---|---|---|---|
| Posterior fossa syndrome (n = 37) | No posterior fossa syndrome (n = 121) | |||
| Physical Performance Test, total test score | 20.1 (5.91) | 24.7 (3.27) | −3.65 (−5.36 to −1.93) | <.001 |
| Resting heart rate | 78.2 (14.80) | 78.3 (12.63) | −0.42 (−5.19 to 4.35) | .86 |
| Mobility | 8.7 (3.43) | 7.9 (6.65) | 0.43 (−2.11 to 2.97) | .73 |
| Outcome | No. (%) | Adjusted, OR (95% CI) | ||
|---|---|---|---|---|
| Posterior fossa syndrome (n = 37) | No posterior fossa syndrome (n = 121) | |||
| Assistance with routine needs | 17 (60.7) | 18 (17.6) | 8.00 (2.56 to 25.04) | <.001 |
| Assistance with personal care needs | 3 (10.7) | 3 (2.9) | 3.06 (0.39 to 24.27) | .29 |
| Driver’s license | 11 (39.3) | 72 (70.6) | 0.42 (0.14 to 1.22) | .57 |
| Educational attainment | ||||
| ≥College | 6 (22.2) | 28 (28.3) | 0.77 (0.31 to 1.89) | .57 |
| ≥High school | 8 (29.6) | 35 (35.3) | ||
| <High school | 13 (48.1) | 36 (36.4) | ||
| Employed, yes | 6 (35.3) | 57 (71.2) | 0.32 (0.08 to 1.27) | .11 |
| Independent living | 7 (22.6) | 36 (35.3) | 0.66 (0.17 to 2.47) | .54 |
| Married, yes | 5 (50.0) | 20 (50.0) | 0.50 (0.11 to 2.37) | .38 |
| HRQoL | ||||
| Physical Component Summary impairment | ||||
| Overall | 10 (37.0) | 17 (17.2) | 2.13 (0.71 to 6.44) | .18 |
| Physical functioning subscale | 11 (39.3) | 20 (19.6) | 1.61 (0.57 to 4.54) | .37 |
| Role limitations (physical) | 12 (42.9) | 25 (24.5) | 1.98 (0.71 to 5.52) | .19 |
| Bodily pain impairment | 3 (10.7) | 11 (11.0) | 0.70 (0.14 to 3.38) | .65 |
| General health impairment | 6 (20.7) | 21 (20.8) | 1.61 (0.50 to 5.25) | .43 |
| Mental Component Summary (MCS) impairment | ||||
| Overall | 4 (14.8) | 12 (12.1) | 1.12 (0.26 to 4.87) | .88 |
| Vitality impairment | 3 (10.3) | 14 (13.9) | 0.88 (0.19 to 4.09) | .87 |
| Social functioning impairment | 6 (20.7) | 13 (12.7) | 1.32 (0.39 to 4.49) | .67 |
| Role limitations (emotional) | 6 (21.4) | 8 (7.8) | 3.31 (0.79 to 13.84) | .10 |
| Emotional well-being impairment | 4 (13.8) | 12 (12.0) | 1.00 (0.25 to 3.93) | .99 |
| Alcohol use disorder risk | 5 (16.7) | 26 (25.7) | NA | .30 |
| Smoking status: current smoker | 5 (16.7) | 7 (6.8) | NA | .14 |
| Physical activity | 13 (43.3) | 41 (41.0) | NA | .82 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlioma Diagnosis and Treatment · Intraoperative Neuromonitoring and Anesthetic Effects · Meningioma and schwannoma management
Introduction
Posterior fossa syndrome, also known as cerebellar mutism syndrome, is a severe and debilitating postoperative complication after posterior fossa tumor resection,^1,2^ with reported incidence ranging from 6% to 39% because of variability in diagnostic criteria, timing of assessment, and treatment era.^3,4,5,6,7^ Symptoms typically emerge 1 to 2 days after surgery and include transient mutism or reduced speech, ataxia, hypotonia, motor weakness, and emotional lability.^2^ More recent, methodologically rigorous cohorts using standardized definitions report a more consistent incidence of approximately 20% to 30%.^4,8,9^
Posterior fossa syndrome has been described under multiple labels over the past 35 years, including cerebellar speech syndrome, pseudobulbar palsy, mutism without behavioral impairment, and cerebellar cognitive affective syndrome.^10,11,12,13,14,15^ To encompass the full spectrum of neuropsychiatric and behavioral manifestations, we use the term posterior fossa syndrome throughout.^16^ Recovery is often prolonged and incomplete, with persistent cognitive, affective, and motor sequelae^17^ that place significant burdens on families and the health care system.^18^
Clinical and anatomic risk factors for posterior fossa syndrome include tumor histology, size, location, invasiveness, patient age, and the medulloblastoma molecular subgroup.^4,19^ Neuroimaging suggests that injury to the proximal dentatothalamocortical tract and disruption of the fastigial nucleus and/or superior cerebellar peduncles may play a critical role in posterior fossa syndrome pathophysiology.^20,21^ The severity of mutism, dysmetria, and ataxia is associated with dentatothalamocortical tract injury, and functional magnetic resonance imaging demonstrates cerebrocerebellar abnormalities extending beyond the surgical field.^22^
Survivors of medulloblastoma face long-term morbidity,^23,24^ particularly in processing speed, task efficiency, and working memory.^25,26^ Survivors of medulloblastoma with posterior fossa syndrome show greater early declines,^27^ raising concerns about accelerated cognitive aging and early dementia. However, long-term neurobehavioral outcomes in adolescents and young adults with posterior fossa syndrome remain poorly characterized. Rigorous evaluation of chronic morbidity is essential to guide clinical care and targeted interventions.
The St. Jude Lifetime Cohort Study (SJLIFE) provides a unique opportunity to assess neurologic, neurocognitive, social, and quality of life outcomes among long-term survivors of medulloblastoma and to examine differences by posterior fossa syndrome status. We investigated these outcomes in a prospectively followed cohort, hypothesizing that survivors with posterior fossa syndrome would show worse neurologic, intellectual, and academic performance than those without posterior fossa syndrome.
Methods
This cohort study was conducted as part of SJLIFE, retrospective cohort with prospective follow-up of survivors of childhood cancer with at least 5 years since diagnosis, diagnosed between 1962 and 2012 and treated at St. Jude Children’s Research Hospital.^28^ SJLIFE was approved by the St. Jude Children’s Research Hospital institutional review board, and all participants provided written informed consent. This study is reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline
Study Design and Population
The St. Jude Children’s Research Hospital brain tumor program began in 1985; thus, all survivors of medulloblastoma in this analysis were diagnosed between 1985 and 2012. Long-term outcome assessment of survivors began in 2007. Participants undergo comprehensive clinical evaluation and neurocognitive testing every 5 years,^29^ with additional assessments, including physical function testing (eMethods in Supplement 1) and questionnaires capturing sociodemographic characteristics, health status, and medical history. Race and ethnicity were categorized as White, non-Hispanic and other. Further categorization of the other race group and ethnicity is not feasible owing to small cell sizes. This category includes Asian; Black; Caribbean; Mexican or Chicano; not otherwise specified Spanish, Hispanic, or Latino; Puerto Rican; and South or Central American. The SJLIFE cohort has been previously described.^28,30^
Eligibility criteria included a diagnosis of medulloblastoma at age 3 years or older and completion of at least 1 on-campus SJLIFE evaluation. Children younger than 3 years at diagnosis were excluded because they typically receive infant treatment protocols involving high-dose chemotherapy (with or without autologous stem cell transplant) and radiation-delaying strategies. Posterior fossa syndrome classification was based on physician documentation in the medical record. It required mutism or markedly reduced speech output (eg, limited to 2- to 3-word phrases), with or without accompanying behavioral dysregulation, ataxia, or hypotonia. For survivors diagnosed before standardized posterior fossa syndrome definitions were widely adopted, classification relied on explicit clinical documentation. Survivors with unrelated neurologic or neurogenetic disorders were excluded. Among 337 eligible survivors with at least 5 years from diagnosis, 231 were aged 3 years or older at diagnosis, and 158 (37 with posterior fossa syndrome; 121 without posterior fossa syndrome) completed a campus evaluation before the analysis cutoff (April 30, 2020) (eFigure in Supplement 1).
Because younger age at craniospinal irradiation and at diagnosis are strongly correlated and both are associated with posterior fossa syndrome risk,^31,32,33^ only age at diagnosis was included in multivariate models. Treatment details, including surgery, radiation, and chemotherapy, were abstracted from medical records. Patients with medulloblastoma were stratified as average risk or high risk based on modified Chang tumor staging, patient age, and extent of surgical resection and received risk-adapted craniospinal photon irradiation followed by chemotherapy..
Neurocognitive Assessment
Participants completed a standardized 2-hour evaluation administered by a trained examiner. The battery assessed intelligence, attention, academics, processing speed, memory, and executive function and was repeated every 5 years.^18,19,20^ Scores were converted to age-adjusted z scores normalized to the general population (mean [SD], 0 [1]); impairment was defined as lower than −1.28 (10th percentile). Participants also completed the 32-item Neurocognitive Questionnaire^34^ on a validated scale (range, 1-3; higher scores indicate more problems).
Physical Performance and Neurologic Assessment
A clinical exercise physiologist conducted physical performance testing, including resting vitals, the 7-item Physical Performance Test,^35^ and timed up-and-go evaluation.^36^ Additional performance assessments are detailed in the eMethods in Supplement 1.^35,36,37,38,39,40,41,42,43^^,^ Neurologic symptoms, including dysarthria, were obtained through medical record review, self-report, or physical examination and graded using the modified National Cancer Institute Common Terminology Criteria for Adverse Events (version 4.03).^44^ Grade 2 or greater was considered impaired. Motor function was assessed through neurologic examination as part of the standardized SJLIFE evaluation.
Hearing Assessment
Audiologic evaluations measured pure tone thresholds (0.25-8.00 kHz). Hearing loss was classified using the International Society of Pediatric Oncology ototoxicity grading scale, with grade 3 or higher considered severe.^45,46,47^ We used grades 3 to 4 to define severe hearing loss because these levels most consistently correspond to clinical recommendations for hearing aids or a cochlear implant at the end of therapy. For asymmetrical hearing loss, the least-impaired ear was used to determine severity.
Social and Quality of Life Assessment
Quality of life was evaluated using the Short Form-36 (SF-36),^48^ with impairment defined as a T-score less than 40, reflecting 1 SD below age-adjusted norms (population mean [SD], 50 [10]). Questionnaires assessed marital status, employment, education, and daily functioning.
Statistical Analysis
Distributions of continuous variables were visually inspected to assess normality, and potential outliers or influential observations were evaluated. Baseline demographic and treatment characteristics were compared between participants with and without posterior fossa syndrome using the Mann-Whitney U test for continuous variables and the χ^2^ test or Fisher exact test for categorical variables, as appropriate.
Associations between posterior fossa syndrome and outcomes were examined using multivariable linear regression for continuous outcomes and multivariable logistic regression for binary outcomes. Models adjusted for age at diagnosis, years since diagnosis, sex, extent of surgical resection, craniospinal irradiation dose, cerebrospinal fluid (CSF) shunt placement, and treatment protocol; models of neurocognitive outcomes additionally adjusted for severe hearing loss. For continuous outcomes, age-adjusted z scores from the SJLIFE registry were used, and coefficients represent adjusted mean differences in z score units. No baseline covariates had missing data. Participants with missing outcome data were excluded from the respective analyses, and models were fit using all available observations. Because the mechanism of missingness cannot be fully assessed, results should be interpreted accordingly. Cumulative incidence was compared using the log-rank test. P values were 2-sided, and statistical significance was set at P ≤ .05. All analyses were performed using SAS software version 9.4 (SAS Institute). Data were analyzed from January 1, 2024, to December 1, 2025.
Results
A total of 158 patients (median [range] age at assessment, 25 [11-44] years; 96 [60.8%] male) were assessed, including 37 (23%) who developed posterior fossa syndrome and 121 (76.6%) who did not. Patients with vs without posterior fossa syndrome did not differ in age at diagnosis, radiation dose, or age at assessment (Table 1). Neurological, neurocognitive, physical performance, and social outcomes were assessed at a median (range) of 14.2 (7.8-33.1) years after diagnosis of medulloblastoma. Participants with posterior fossa syndrome were more likely to have a CSF shunt (22 participants [59.5%] vs 36 participants [29.8%]; P = .001), and a higher proportion underwent multiple surgical resections (15 participants [40.5%] vs 30 participants [24.8%]), although the difference did not reach statistical significance (P = .06). Participants with posterior fossa syndrome were more likely to have a CSF shunt (22 participants [59.5%] vs 36 participants [29.8%]; P = .001) and less likely to have a body mass index (calculated as weight in kilograms divided by height in meters squared) greater than 25 (13 participants [35.1%] vs 68 participants [56.2%]; P = .02), while all other baseline characteristics were similar between groups (Table 1). Additionally, there were no baseline differences between individuals who participated and those who did not (eTable 1 in Supplement 1), indicating the representativeness of the study sample. There was no significant difference in age at the time of diagnosis between participants with posterior fossa syndrome (median [range] age, 7.5 [3.2-17.4] years) and those without posterior fossa syndrome (median [range] age, 9.1 [3.0-22.3] years). Age at diagnosis and age at craniospinal irradiation were highly correlated clinically; all comparisons were adjusted using age at diagnosis.
Long-Term Neurological Impairment
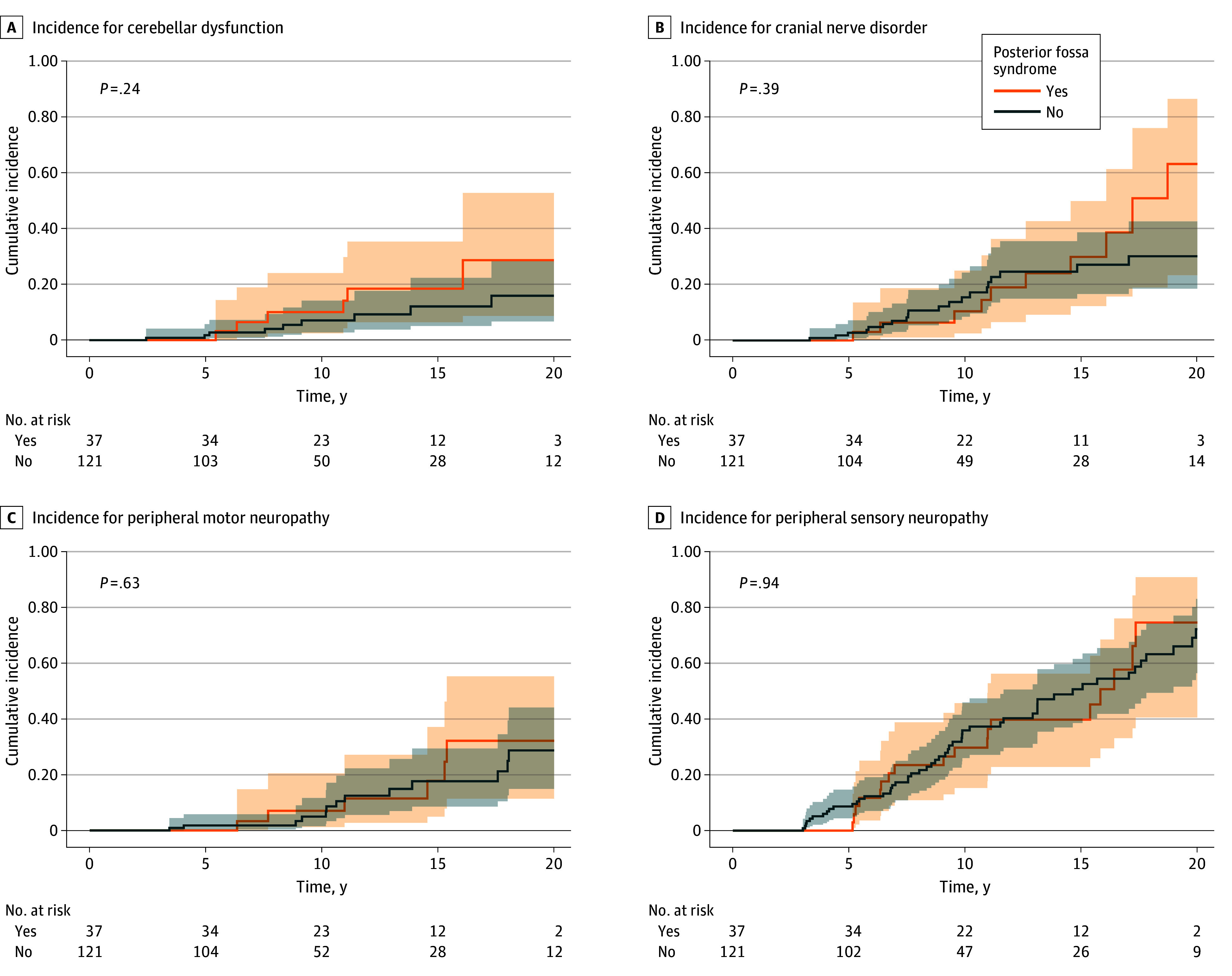
The prevalence of cerebellar dysfunction, cranial nerve disorders, and peripheral sensory and motor neuropathy increased with increasing time from diagnosis in both groups with and without posterior fossa syndrome (Figure). Although no significant differences between groups were observed in time-to-event analyses, the cumulative incidence difference of cranial nerve disorders 20 years after diagnosis was 33% (95% CI, 0% to 68.7%), and the difference for cerebellar dysfunction was 12% (95% CI, 0% to 39.0%) (Figure). Among participants with posterior fossa syndrome, the median (IQR) time to speech follow-up was 2.11 (1.05-3.37) months (range, 0.03-19.47 months). Of 10 neurological outcomes examined, only severe hearing loss differed between groups in unadjusted analyses, although this association was not significant after adjustment (odds ratio [OR], 1.84 [95% CI, 0.58-5.82]; P = .30) (eTable 2 and eTable 3 in Supplement 1). Sensory Organization Test performance did not differ significantly between participants with and without posterior fossa syndrome.
Cumulative Incidence Function Plots of Grade 2 or Higher Neurologic Impairments Among Survivors With and Without Posterior Fossa Syndrome
Long-Term Neurocognitive Impairment
Participants with history of posterior fossa syndrome demonstrated lower performance across several neurocognitive domains compared with those without posterior fossa syndrome (Table 2; eTable 4 in Supplement 1), including for focused attention (mean [SD] score, −2.7 [1.45] vs −1.1 [1.70]; P < .001), motor processing speed (mean [SD] score, −3.3 [1.15] vs −2.2 [1.50]; P < .001), visuomotor processing speed (mean [SD] score, −2.3 [0.83] vs −1.3 [0.93]; P < .001), cognitive flexibility (mean [SD] score, −3.4 [1.20] vs −1.9 [1.77]; P < .001), verbal fluency (mean [SD] score, −1.4 [1.03] vs −0.7 [1.18]; P = .001), visual memory (mean [SD] score, −1.9 [1.33] vs −1.3 [1.30]; P = .02), and working memory (mean [SD] score, −1.1 [1.02] vs −0.6 [1.06]; P = .01). After adjusting for demographic and treatment variables, posterior fossa syndrome remained significantly associated with poorer focused attention (β = −1.04 [95% CI, −1.62 to −0.45]), motor processing speed (β = −0.62 [95% CI, −1.16 to −0.09]), visuomotor processing speed (β = −0.65 [95% CI, −0.97 to −0.33]), and cognitive flexibility (β = −0.85 [95% CI, −1.44 to −0.27]). Differences in verbal fluency and visual memory were not statistically significant. No adjusted differences were identified for general intelligence, academic achievement, or most Neurocognitive Questionnaire self-report domains. In multivariable models, posterior fossa syndrome, younger age at diagnosis, and CSF shunt placement were associated with lower scores in selected domains (eTables 5-8 in Supplement 1).
Long-Term Physical Performance, Social Outcomes, and Quality of Life Outcomes
Participants with posterior fossa syndrome had poorer Physical Performance Test z scores (estimate, −3.65 [95% CI, −5.36 to −1.93]; P < .001) than those without posterior fossa syndrome after adjusting for age at diagnosis, years from diagnosis, sex, surgical resections, craniospinal radiation, shunt placement, and treatment protocol (Table 3). Participants with posterior fossa syndrome were more likely to require assistance with routine needs (eg, walking, grocery shopping, cleaning) (OR, 8.00 [95% CI, 2.56 to 25.04]; P < .001) (Table 4). Independent living was reported by 7 participants (22.6%) with posterior fossa syndrome compared with 36 participants (35.3%) without posterior fossa syndrome (Table 4). Although participants with posterior fossa syndrome reported higher unemployment (31 participants [64.7%]) than those without posterior fossa syndrome (64 participants [28.8%]) (P = .005) (Table 4), multivariable models adjusting for age at diagnosis, years from diagnosis, sex, surgical resections, craniospinal radiation dose, CSF shunt, and treatment protocol found no significant difference between groups (OR, 0.32 [95% CI, 0.08 to 1.27]; P = .11) (Table 4). Participants with posterior fossa syndrome were less likely to have a driver’s license (11 participants [39.3%]) than those without posterior fossa syndrome (72 participants [70.6%]) (P = .002), a difference which was not significant in multivariable models (OR, 0.42 [95% CI, 0.14 to 1.22]; P = .57) (Table 4).
Discussion
Our cohort study identified significant neurocognitive and physical impairments in participants with posterior fossa syndrome at a median of 14.2 years of follow-up, which may adversely affect their social and functional abilities.^49^ After adjusting for age at diagnosis and treatment, participants with posterior fossa syndrome demonstrated greater neurocognitive impairments in attention, processing speed, and executive function than those without posterior fossa syndrome. Additionally, participants with posterior fossa syndrome demonstrated decreased physical performance scores and increased need for assistance with daily routine needs, highlighting the long-term outcomes of the devastating postoperative complication of posterior fossa syndrome. Our findings complement but differ from those of Schreiber et al,^27^ who described worsening neurocognitive outcomes within approximately 5 years of diagnosis among individuals treated with the SJMB03 risk-adapted craniospinal irradiation protocol. In contrast, our study draws on the broader SJLIFE cohort, which includes survivors of medulloblastoma diagnosed from 1985 to 2012 across multiple treatment protocols and regimens. We found that neurocognitive impairments not only persisted but broadened over time, with enduring deficits in attention, processing speed, and executive function evident well into adulthood. These results extend prior observations of early survivorship by suggesting that neurocognitive dysfunction in individuals with posterior fossa syndrome is long-lasting, clinically meaningful, and more extensive than previously characterized.
Impaired processing speed (>2 SD below the mean) and below-average intellectual ability have been observed in individuals with posterior fossa syndrome as early as 1 year after diagnosis,^50^ with deficits persisting into later survivorship, likely reflecting disruption of frontocerebellar pathways.^11^ Our findings suggest that more than a decade after diagnosis, individuals with posterior fossa syndrome continue to have poorer attention, processing speed, and executive functioning than survivors of medulloblastoma without posterior fossa syndrome. These findings suggest that early brain injury limits brain plasticity and cognitive recovery in the long term. Additionally, we found discrepancies between objective and subjective neurocognitive outcomes, indicating that survivors may underreport their impairments, possibly due to limited insight or impaired judgment, as reported in adult brain tumor patients.^51,52,53^
Participants with posterior fossa syndrome had a higher shunt rate than those without posterior fossa syndrome, consistent with increased posterior fossa syndrome risk.^4^ Hydrocephalus is associated with reduced attention, IQ, academic performance, and school retention in childhood brain tumor survivors.^54^ Although the incidence of hydrocephalus appears similar across surgical centers, shunt placement is reported more frequently at lower-volume centers.^4,55,56^ Higher neurosurgical volume has been associated with improved outcomes. However, definitions vary across studies and over time,^55,57,58^ with Nationwide Inpatient Sample data indicating a progressive centralization of pediatric brain tumor resections to higher-volume centers beginning in the late 1980s. In 2021, Khan et al^4^ defined low-volume centers as those in resource-limited settings, staffed by nonpediatric neurosurgeons, or with cumulative pediatric neurosurgical case volume of fewer than 500 procedures, whereas accredited pediatric neurosurgery fellowships were considered high-volume regardless of caseload.^59^ Given these differing frameworks and the extended temporal span of our cohort, volume-based comparisons should be interpreted cautiously. Even after controlling for shunt placement, posterior fossa syndrome remained associated with poorer cognitive outcomes.
Although not statistically significant, numerically more participants with posterior fossa syndrome patients required multiple surgical resections (15 participants [40.5%] vs 30 participants [24.8%]; P = .06). Long-term complications can be reduced by performing surgical procedures at high-volume centers staffed by accredited pediatric neurosurgeons.^60^ One high-volume center observed reduced incidence of posterior fossa syndrome, from 39% to 10.8%, in association with using a telovelar-over-transvermian approach.^3^ However, a large prospective European postoperative speech impairment study found no association between surgical approach and postoperative speech impairment.^8^ Recent consensus guidelines recommend approaches that maximize exposure while minimizing retraction, even if a small residual is left to preserve function.^61^
Hearing loss and neurological impairments are known treatment-related comorbidities in patients treated for medulloblastoma secondary to exposure to platinum-based chemotherapies and radiation. Based on our findings, we cannot determine whether posterior fossa syndrome was associated with increasing these risks. Severe hearing loss, younger age at diagnosis, and posterior fossa syndrome are substantial risk factors associated with decline in intellectual and academic outcomes in childhood medulloblastoma.^62,63^ This emphasizes the need for close monitoring and early interventions, such as hearing aids and reading interventions, in patients with posterior fossa syndrome at risk of neurocognitive impairments. However, prior studies indicate that patients with posterior fossa syndrome experience more severe neurological deficits and slower recovery in the first 5 years after diagnosis compared with those without posterior fossa syndrome.^4^
Notably, prior studies of pediatric survivors of brain tumor found that only 40% achieved complete independence,^64^ and many faced work-related challenges.^65^ In contrast, only 22.6% of participants with posterior fossa syndrome in our study lived independently, potentially underscoring the additive burden of posterior fossa syndrome alongside craniospinal radiation. However, we used a single indicator of independent living, whereas prior studies used multiple indicators in their definitions of independence. Individuals with posterior fossa syndrome are nearly twice as likely to require special education services compared with those without posterior fossa syndrome.^66^ Our findings highlight significant deficits in quality of life, social outcomes, and functioning. Early cognitive assessments can help identify long-term needs, guiding caregiver education and support services.^67^ This underscores the importance of educational institutions and employers recognizing these unique challenges and providing necessary accommodations for individuals with posterior fossa syndrome.^68^
Evidence for the efficacy of cognitive remediation in posterior fossa syndrome is still emerging, but initial findings show promise. A pilot study demonstrated the benefits of a cognitive-motor intervention, resulting in significant improvements in visual attention, visuospatial working memory, semantic verbal fluency, eye-hand coordination, reaction time, and auditory-motor synchronization and a reduction in ataxia symptoms.^69^ Interventions focused on physical activity and health behaviors also benefit brain structure and functioning among survivors.^70,71^
Limitations
This study has notable strengths, but several limitations highlight areas that warrant further research. Posterior fossa syndrome diagnoses were retrospectively made from medical records of patients diagnosed between 1962 and 2012, before the syndrome was well characterized and severity classifications existed, potentially underestimating milder cases. The first study linking mutism to cerebellar injury was published in 1985,^14^ and a formal definition of posterior fossa syndrome was only established in 2011.^72^ The current posterior fossa syndrome diagnostic criteria^4,73,74,75^ categorize impairments into complete or partial mutism, providing a more granular measure of posterior fossa syndrome.^4^ We were unable to include molecular subgroup data of medulloblastoma because our patient diagnoses predated the 2012 consensus.^76^ Records lacked details on tumor size and surgical techniques, preventing inclusion in our analysis. As standardized motor coordination measures, such as the Sensory Organization Test and modified Total Neuropathy Score, were not collected, our ability to characterize gait and coordination deficits was limited—a gap that future studies can address using our dedicated gait laboratory. Furthermore, small sample size and reliance on the most recent assessment restricted our analysis to cross-sectional long-term outcomes, which may not capture progression or account for selection bias.
Conclusions
In this cohort study, survivors of medulloblastoma with posterior fossa syndrome experienced persistent neurocognitive impairments and diminished physical performance, which were associated with greater need for assistance with daily activities. While acute postsurgical deficits associated with posterior fossa syndrome are recognized, their persistence in long-term survivors highlights the importance of longitudinal surveillance and continued intervention to optimize quality of life. These findings suggest that posterior fossa syndrome could worsen neurocognitive and neurological outcomes in survivors of medulloblastoma. Early assessment of posterior fossa syndrome severity in this high-risk population can facilitate timely opportunities for caregiver education, speech and physical therapy, and advocacy for support services, including academic support, vocational rehabilitation, and accommodations that enhance functional independence and quality of life. Finally, our study highlighted the substantial and long-lasting morbidity associated with a postoperative complication, emphasizing the urgent need for improved surgical techniques in posterior fossa tumor resections performed at high-volume, accredited, pediatric neurosurgical centers.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thomale UW, Driever PH. Inconsistent terminology for cerebellar mutism. Childs Nerv Syst. 2013;29(5):717-718. doi:10.1007/s 00381-013-2074-z 23503612 · doi ↗ · pubmed ↗
- 2Wibroe M, Cappelen J, Castor C, . Cerebellar mutism syndrome in children with brain tumours of the posterior fossa. BMC Cancer. 2017;17(1):439. doi:10.1186/s 12885-017-3416-0 28637445 PMC 5480181 · doi ↗ · pubmed ↗
- 3Kameda-Smith MM, Ragulojan M, Elliott C, ; Mc Master Pediatric Brain Tumour Study Group (PBTSG) and the Canadian Neurosurgery Research Collaborative (CNRC). National multicentered retrospective review of clinical and intraoperative factors associated with the development of cerebellar mutism after pediatric posterior fossa tumor resection. Childs Nerv Syst. 2024;40(5):1339-1347. doi:10.1007/s 00381-024-06292-0 38279985 · doi ↗ · pubmed ↗
- 4Khan RB, Patay Z, Klimo P, . Clinical features, neurologic recovery, and risk factors of postoperative posterior fossa syndrome and delayed recovery: a prospective study. Neuro Oncol. 2021;23(9):1586-1596. doi:10.1093/neuonc/noab 030 33823018 PMC 8408840 · doi ↗ · pubmed ↗
- 5Thacker N, Bouffet E. Posterior fossa syndrome-time to unmute the silence on cerebellar mutism. Neuro Oncol. 2021;23(9):1427-1428. doi:10.1093/neuonc/noab 147 34139019 PMC 8408842 · doi ↗ · pubmed ↗
- 6de Laurentis C, Cristaldi PMF, Rebora P, . Posterior fossa syndrome in a population of children and young adults with medulloblastoma: a retrospective, multicenter Italian study on incidence and pathophysiology in a histologically homogeneous and consecutive series of 136 patients. J Neurooncol. 2022;159(2):377-387. doi:10.1007/s 11060-022-04072-x 35767101 · doi ↗ · pubmed ↗
- 7Renne B, Radic J, Agrawal D, . Cerebellar mutism after posterior fossa tumor resection in children: a multicenter international retrospective study to determine possible modifiable factors. Childs Nerv Syst. 2020;36(6):1159-1169. doi:10.1007/s 00381-019-04058-7 30659354 · doi ↗ · pubmed ↗
- 8Grønbæk JK, Wibroe M, Toescu S, ; CMS study group. Postoperative speech impairment and surgical approach to posterior fossa tumours in children: a prospective European multicentre cohort study. Lancet Child Adolesc Health. 2021;5(11):814-824. doi:10.1016/S 2352-4642(21)00274-1 34624241 · doi ↗ · pubmed ↗