Rapidly Progressive Primary Ovarian Malignant Perivascular Epithelioid Cell Tumor
Kenta Sonehara, Takashi Suzuki

TL;DR
A rare and aggressive ovarian tumor called PEComa is reported, highlighting its rapid progression and poor prognosis despite initial surgery.
Contribution
This report provides insights into the clinical behavior of primary ovarian malignant PEComa and emphasizes the need for systemic therapy alongside surgery.
Findings
The patient developed local recurrence and lung metastasis within 72 days after surgery.
The tumor exhibited multiple pathological risk factors, including high mitotic activity and vascular invasion.
The case underscores the importance of multidisciplinary management and systemic therapy for this rare tumor.
Abstract
Perivascular epithelioid cell tumor (PEComa) is a rare mesenchymal neoplasm characterized by a unique dual differentiation toward smooth muscle and melanocytic lineages. While PEComas can arise in various gynecologic organs, primary malignant ovarian PEComa is exceptionally rare and shows a wide spectrum of clinical behaviors. We report a case of a rapidly progressive primary ovarian malignant PEComa with an extremely poor prognosis. A 73-year-old woman presented with fever and malaise. A CT scan incidentally revealed a left ovarian tumor, for which she was referred to our department. Tumor markers were within normal limits, but MRI and CT suggested a left ovarian malignancy. A total hysterectomy and bilateral salpingo-oophorectomy were performed. Pathological examination revealed a 9 cm solid mass with necrosis, cytologic atypia, high mitotic activity (14/HPF), and vascular invasion.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
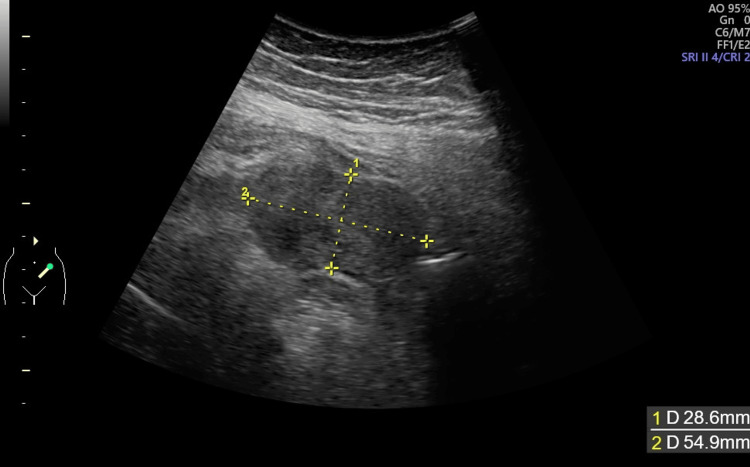 Figure 1
Figure 1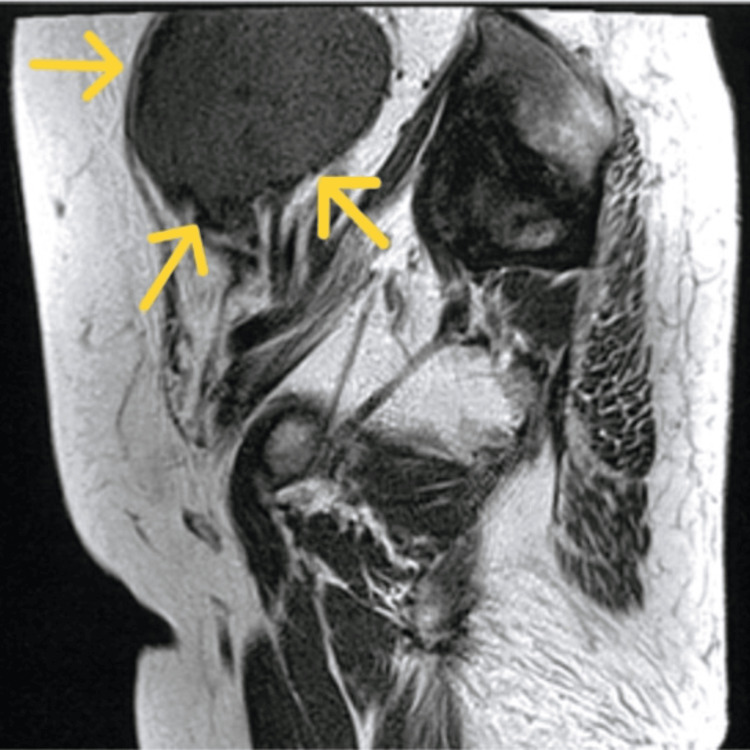 Figure 2
Figure 2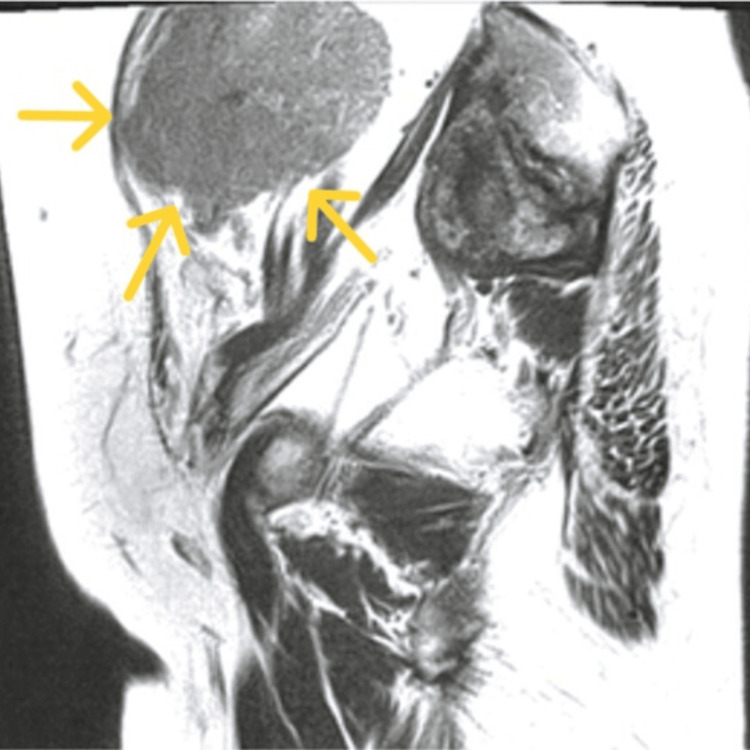 Figure 3
Figure 3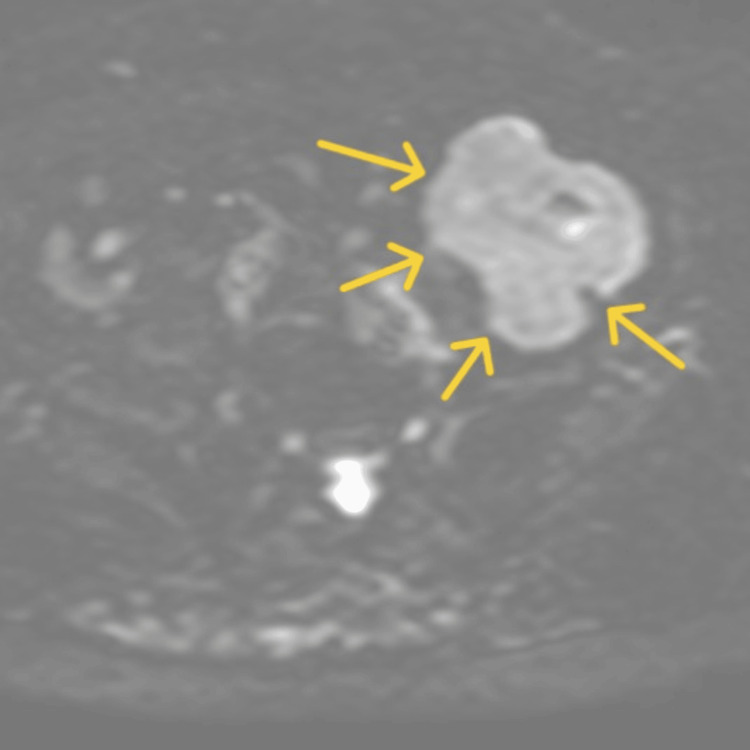 Figure 4
Figure 4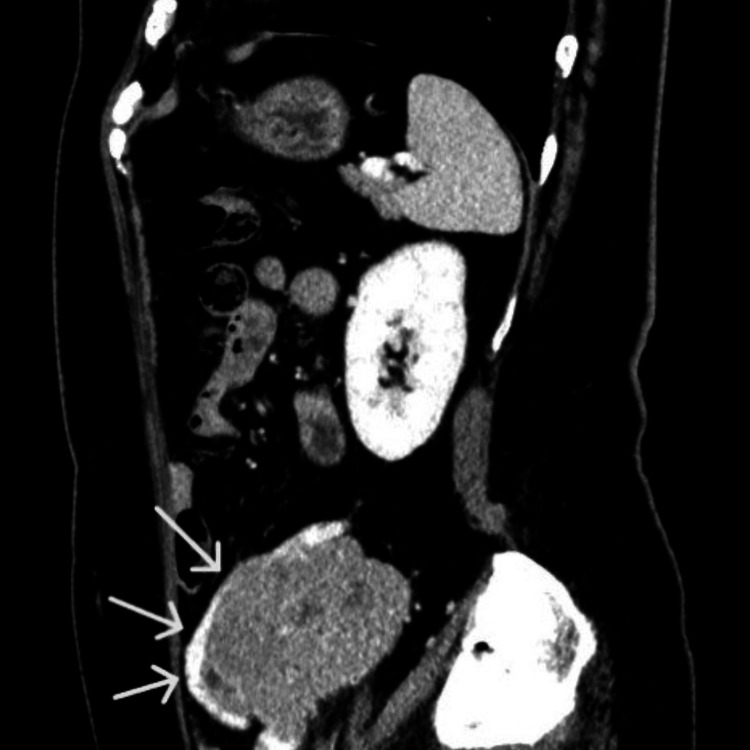 Figure 5
Figure 5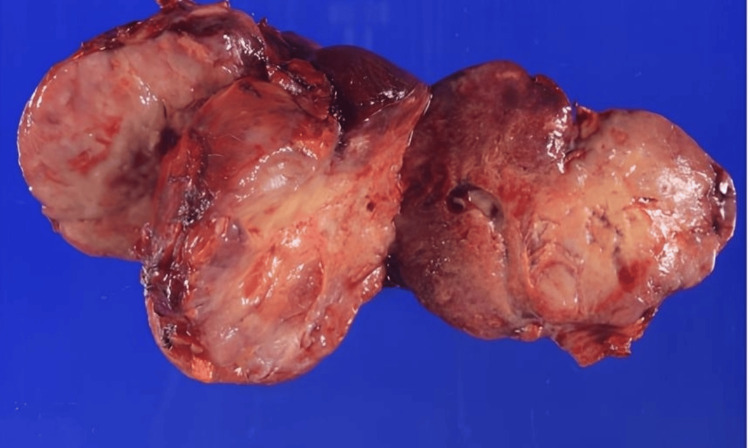 Figure 6
Figure 6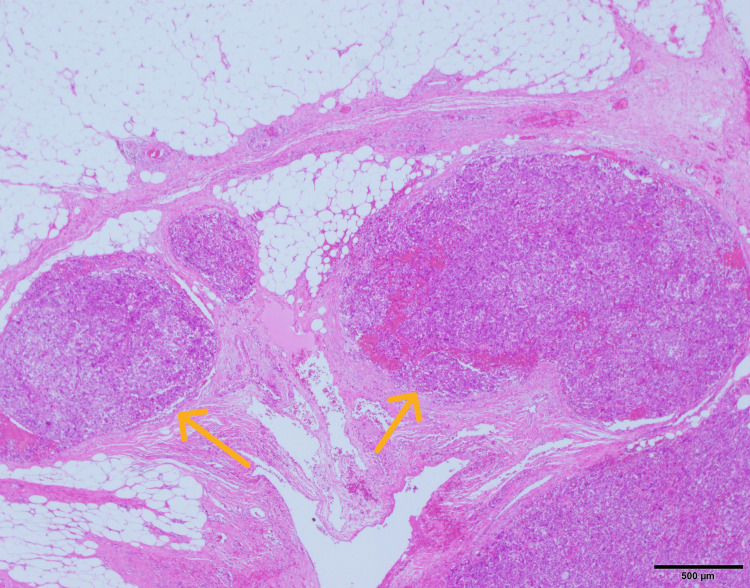 Figure 7
Figure 7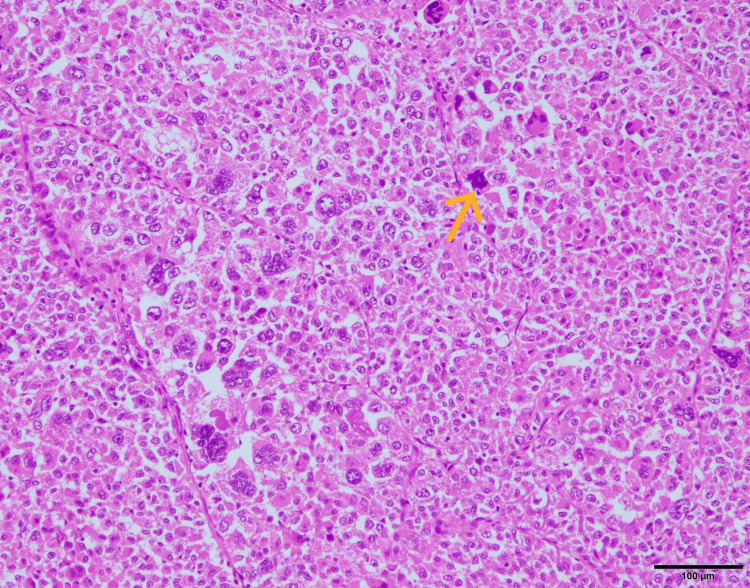 Figure 8
Figure 8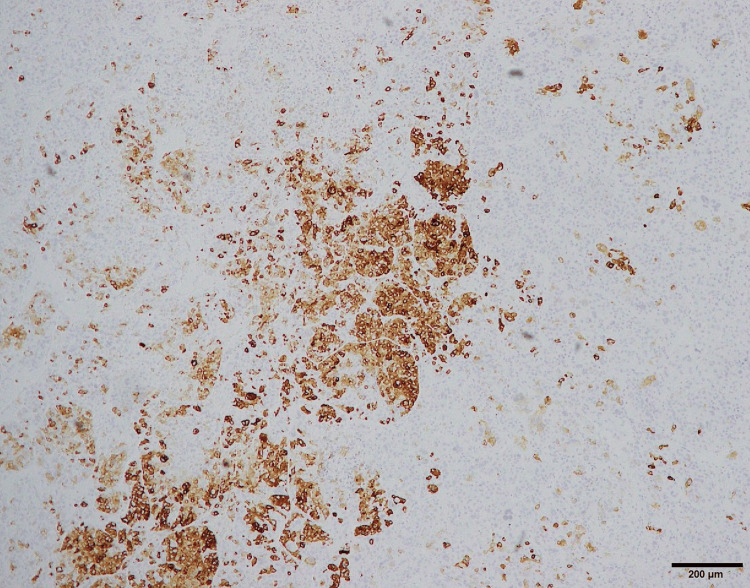 Figure 9
Figure 9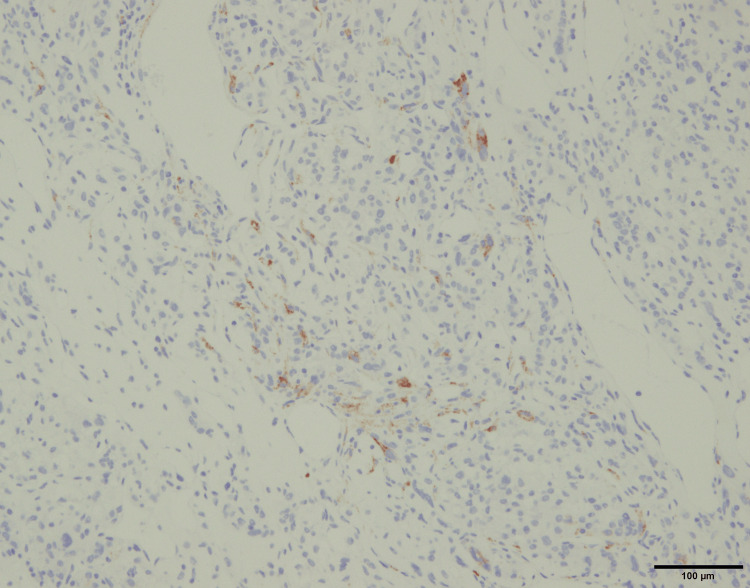 Figure 10
Figure 10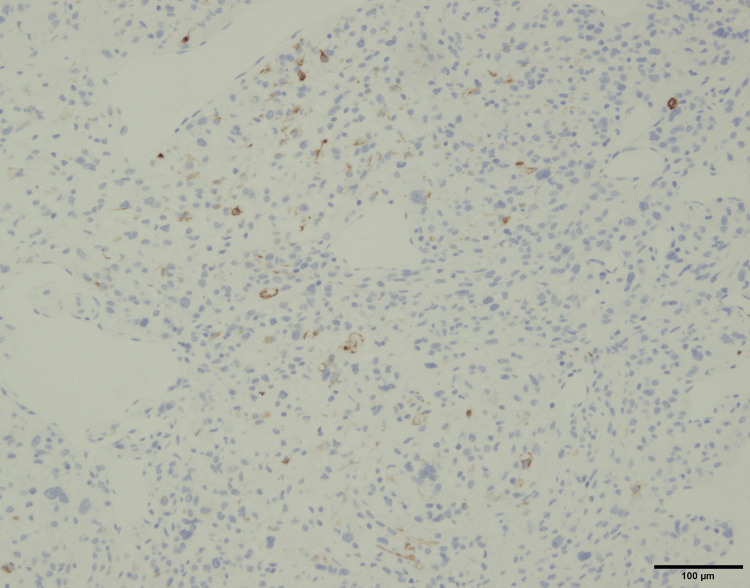 Figure 11
Figure 11| Laboratory parameter | Patient value | Reference range | Units |
| CRP | 11.98 | 0.00–0.14 | mg/dL |
| CEA | <1.8 | 0.0–5.0 | ng/mL |
| CA19-9 | 9 | 0–37 | U/mL |
| CA125 | 8.1 | 0–35 | U/mL |
| SCC | 0.8 | 0.0–1.9 | ng/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTuberous Sclerosis Complex Research · Vascular Tumors and Angiosarcomas · Renal cell carcinoma treatment
Introduction
Perivascular epithelioid cell tumor (PEComa) is a rare mesenchymal neoplasm characterized by a distinctive histological feature [1]. Perivascular epithelioid cells show both smooth muscle and melanocytic differentiation [2]. While PEComas can arise in various gynecologic organs such as the uterus, ovary, and vulva, gynecologic PEComas account for approximately 25% of all reported cases [3,4], and primary malignant ovarian PEComas are extremely rare [5]. Due to the infrequent nature of this disease and lack of distinct symptoms, diagnostic procedures, as well as treatment options, are limited [6]. We report a case of a primary ovarian malignant PEComa with a poor prognosis that resulted in a rapidly progressive clinical course.
Case presentation
A 73-year-old woman was referred to our department with a suspected left ovarian tumor, which was incidentally found during a CT scan for a fever and general malaise. The patient had a significant oncological history of two independent primary malignancies: left breast cancer at age 58 and lung cancer at age 68, both of which were treated with curative surgical resection. No adjuvant radiotherapy or systemic chemotherapy was administered for these prior cancers. There was no clinical or radiological evidence of recurrence of these tumors at the time of the PEComa diagnosis.
Upon presentation, she had a temperature of 37.5°C. Abdominal palpation revealed no tenderness or palpable mass. A transabdominal ultrasound showed a 54 × 28 mm mass in the left lower abdomen (Figure 1), but a transvaginal ultrasound was unable to locate a mass. Laboratory tests showed an elevated C-reactive protein level of 11.98 mg/dL, while epithelial tumor markers (squamous cell carcinoma antigen, cancer antigen 125, carbohydrate antigen CA19-9, carcinoembryonic antigen) were within normal limits (Table 1).
Transabdominal ultrasonography.A transabdominal ultrasound showing a 54 × 28 mm mass in the left lower abdomen.
MRI revealed a 76 × 56 mm mass with a slightly hyperintense T2 signal and a hypointense T1 signal relative to the myometrium (Figures 2, 3).
T2-weighted MRI scan.MRI demonstrating a 76 × 56 mm mass (yellow arrow) with slightly higher T2 signal intensity than the myometrium and low T1 signal intensity.
T1-weighted MRI scan.MRI demonstrating a 76 × 56 mm mass (yellow arrow) with slightly higher T2 signal intensity than the myometrium and low T1 signal intensity.
In diffusion-weighted imaging, the tumor showed high signal intensity, supporting the suspicion of malignancy rather than a benign mesenchymal tumor (Figure 4).
Diffusion-weighted MRI scan.The tumor (yellow arrow) showing high signal intensity on diffusion-weighted imaging, which was suggestive of malignancy.
CT images indicated that the mass was a left ovarian tumor, as the left ovarian vein drained into it (Figure 5).
Contrast-enhanced CT (sagittal view).CT showing the left ovarian vein (white arrow) draining into the mass, suggesting an ovarian origin, with areas of poor enhancement indicating necrosis.
Based on the MRI and CT findings, a left ovarian malignant tumor was suspected, and the patient underwent surgery. The enlarged left adnexa was resected and sent for frozen section pathology, which was inconclusive for distinguishing between an epithelial and a non-epithelial tumor but suggested malignancy. Consequently, a total hysterectomy, completion of bilateral salpingo-oophorectomy (by removing the right adnexa), and partial omentectomy were performed. Peritoneal washings were performed and later confirmed to be negative for malignant cells. Although the intraoperative frozen section suggested malignancy, lymphadenectomy was not performed because the possibility of metastatic recurrence from the patient’s previous breast or lung cancers could not be entirely ruled out at that time. Given the diagnostic uncertainty regarding the primary site, we prioritized a less invasive approach. The resected tumor was a 9 × 7 × 7 cm solid mass with partial necrosis (Figure 6).
Macro image of the resected mass.
Histopathological examination revealed vascular invasion (Figure 7), a mitotic count of 10 mitoses per 10 high-power field (Figure 8), infiltrative growth, cytologic atypia, high mitotic rate, necrosis, and epithelioid cells with eosinophilic to clear cytoplasm.
Hematoxylin and eosin-stained image (×40).Evidence of vascular invasion is present (yellow arrow).
Hematoxylin and eosin-stained image (×100).Representative mitotic figures are shown (yellow arrow).
Immunohistochemical staining was positive for melanocytic markers MelanA and HMB45, as well as the myogenic marker desmin (Figure 9-11).
Immunohistochemical staining for MelanA.
Immunohistochemical staining for HMB45.
Immunohistochemical staining for desmin.
S-100 was negative. Based on the tumor size, infiltrative growth, cytologic atypia, high mitotic rate, necrosis, and vascular invasion, a diagnosis of malignant PEComa was made.
Postoperatively, we offered the patient carboplatin and paclitaxel chemotherapy, which was proposed based on standard ovarian carcinoma protocols, as no established regimen for malignant PEComa exists in Japan. However, the patient declined treatment. CT performed 72 days after surgery revealed a local recurrence on the left pelvic wall, measuring 5 × 3 cm, along with new lung metastases. Despite the aggressive disease progression, the patient’s condition deteriorated rapidly, and she passed away 169 days after surgery.
Discussion
We report the case of a patient with a primary ovarian malignant PEComa with an extremely poor prognosis, who died approximately six months after surgery. Primary ovarian PEComa is exceedingly rare, and its clinical behavior is variable, with most reported cases being benign or borderline [7]. However, previously reported malignant cases have also shown rapid recurrence or death within a short period, consistent with our case [8].
The diagnosis of PEComa is often challenging, requiring differentiation from other tumors such as leiomyoma, epithelioid leiomyosarcoma, and melanoma [1,5-8]. Immunohistochemical analysis demonstrated positivity for MelanA and HMB45, both of which are melanocytic markers characteristic of PEComas. The tumor cells also showed focal positivity for desmin, indicating partial smooth muscle differentiation. The co-expression of melanocytic markers and smooth muscle markers represents a defining immunophenotypic feature of PEComa and is essential for establishing the diagnosis. This immunoprofile is particularly useful in differentiating PEComa from leiomyoma and epithelioid leiomyosarcoma, which typically lack melanocytic marker expression, as well as from malignant melanoma, which does not express smooth muscle markers such as desmin [9-11]. In our case, the diagnosis was based on the positive immunohistochemical staining for both myogenic and melanocytic markers, reflecting the tumor’s biological heterogeneity.
The assessment of malignancy in PEComas has evolved over time. Folpe et al. were the first to propose diagnostic criteria based on six worrisome features (tumor size >5 cm, infiltrative growth pattern, high nuclear grade and cellularity, mitotic rate ≥1 per 50 HPF, necrosis, and vascular invasion) [11]. Later, Schoolmeester et al. evaluated gynecologic PEComas and reported that tumors with four or more worrisome features could be considered malignant [12]. Subsequently, the Modified Folpe criteria were proposed, emphasizing that the presence of necrosis alone, or multiple risk factors, is sufficient for a malignant diagnosis [13]. Our case, which presented with multiple malignant factors, had a predicted poor prognosis. This pathological finding, consistent with the actual rapid clinical course, reinforces the importance of these factors in evaluating the malignancy of PEComas.
PEComas are characterized by the activation of the mTOR pathway due to mutations in TSC1/TSC2 [14]. In recent years, mTOR inhibitors have garnered attention as a promising therapeutic strategy [15]. Clinical trials, such as the AMPECT study of nab-sirolimus, have demonstrated favorable results, including an objective response rate of 39%, a disease control rate of 71%, a median progression-free survival of 10.6 months, and a median overall survival of 40.8 months [16]. However, in Japan, mTOR inhibitors are currently not covered by national health insurance for the treatment of malignant PEComas. Due to these regulatory and financial constraints, we were unable to offer this molecularly targeted therapy to our patient. This case highlights the importance of including malignant PEComa in the differential diagnosis, especially in cases presenting with multiple risk factors. It also underscores the necessity of considering an aggressive treatment strategy from the outset. As this case illustrates, surgery alone may be insufficient, and the introduction of adjuvant therapy or molecularly targeted agents should be actively considered to improve the clinical outcome.
This report is limited by its single-case nature, which restricts the ability to generalize the findings. In addition, molecular analyses were not performed, and standardized treatment strategies for malignant PEComa remain undefined. Nevertheless, this case provides important clinical insight into the potential for rapid progression in primary ovarian PEComa.
Conclusions
Primary ovarian PEComa is a rare mesenchymal tumor with variable clinical behavior. This case highlights that, although many reported cases show indolent features, aggressive progression with early recurrence and metastasis may occur. Accurate diagnosis relies on appropriate histopathological and immunohistochemical evaluation. Further accumulation of cases is necessary to better understand the biological behavior and establish optimal management strategies for this rare entity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Perivascular epithelioid cell tumors (PE Comas) of the bone and soft tissue: a Japanese Musculoskeletal Oncology Group (JMOG) multi-institutional study J Cancer Res Clin Oncol Izubuchi Y Hamada S Tanzawa Y 130651307514920233747085310.1007/s 00432-023-05114-1PMC 10587015 · doi ↗ · pubmed ↗
- 2Malignant perivascular epithelioid cell tumor in the female genital tract: Preferred reporting items for systematic reviews and meta-analyses Medicine (Baltimore) Liu CH Chao WT Lin SC Lau HY Wu HH Wang PH 098201910.1097/MD.0000000000014072 PMC 633659830633211 · doi ↗ · pubmed ↗
- 3Primary perivascular epithelioid cell tumor (PE Coma) of the ovary: a case report and review of the literature Anticancer Res Gadducci A Ugolini C Cosio S Vistoli F Kauffmann EF Boggi U 448344884120213447507310.21873/anticanres.15258 · doi ↗ · pubmed ↗
- 4A retrospective case study of 13 uterine perivascular epithelioid cell neoplasm (PE Coma) patients Onco Targets Ther Gu J Wang W Wang S 178317901420213372782810.2147/OTT.S 300523 PMC 7955772 · doi ↗ · pubmed ↗
- 5Gynecologic perivascular epithelioid cell tumors (PE Comas): a review of recent evidence Arch Gynecol Obstet Levin G Capella MP Meyer R Brezinov Y Gotlieb WH 2381238630920243866426910.1007/s 00404-024-07510-5PMC 11147862 · doi ↗ · pubmed ↗
- 6Perivascular epithelioid cell tumors (PE Coma) of the female genital tract: a challenging question for gynaecologic oncologist and pathologist Gynecol Oncol Rep Gadducci A Zannoni GF 1006033320203268565110.1016/j.gore.2020.100603 PMC 7356199 · doi ↗ · pubmed ↗
- 7Perivascular epithelioid cell tumor of the uterus with ovarian involvement: a case report and review of the literature Am J Case Rep Fitzpatrick M Pulver T Klein M Murugan P Khalifa M Amin K 3093141720162715024610.12659/AJCR.896401 PMC 4913755 · doi ↗ · pubmed ↗
- 8Primary ovarian malignant PE Coma: a case report Int J Gynecol Pathol Westaby JD Magdy N Fisher C El-Bahrawy M 4004043620172768488510.1097/PGP.0000000000000331 · doi ↗ · pubmed ↗