Emerging Threat of Acinetobacter radioresistens Infection in Immunocompromised Patients
Jyotsna Mary George, Guiseppe Calandrino, Rushdah Malik

TL;DR
A rare Acinetobacter species, A. radioresistens, caused infection in an immunocompromised patient, highlighting the need for accurate diagnostics and antimicrobial stewardship.
Contribution
This case report highlights A. radioresistens as an emerging opportunistic pathogen in immunocompromised patients.
Findings
A. radioresistens was identified as pan-susceptible using MALDI-TOF mass spectrometry.
Rapid molecular diagnostics and confirmatory methods are critical for accurate identification and treatment.
The case emphasizes the importance of vigilance for uncommon Acinetobacter species in high-risk patients.
Abstract
Acinetobacter radioresistens is an uncommon human pathogen rarely reported to cause bacteremia. Its accurate identification is crucial yet challenging, with implications for antimicrobial stewardship due to its potential to harbor carbapenem resistance genes. We present the case of a 77‐year‐old male with metastatic lung adenocarcinoma, COPD, and dementia who presented with acute hypoxic respiratory failure and septic shock. Initial empiric antibiotics were vancomycin and cefepime. Gram stain of positive blood cultures revealed Gram‐negative coccobacilli. The VERIGENE BC‐GN microarray system identified an Acinetobacter species, negative for common resistance markers, which was subsequently confirmed as pan‐susceptible Acinetobacter radioresistens by MALDI‐TOF mass spectrometry. The patient’s antibiotic regimen was de‐escalated to intravenous ampicillin‐sulbactam, to which he initially…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
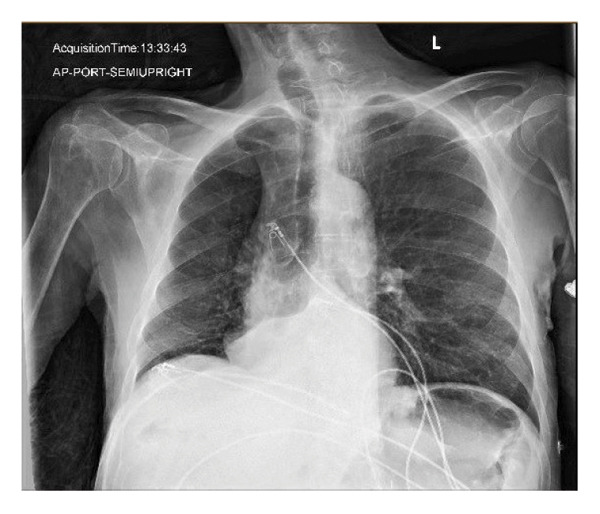 Figure 1
Figure 1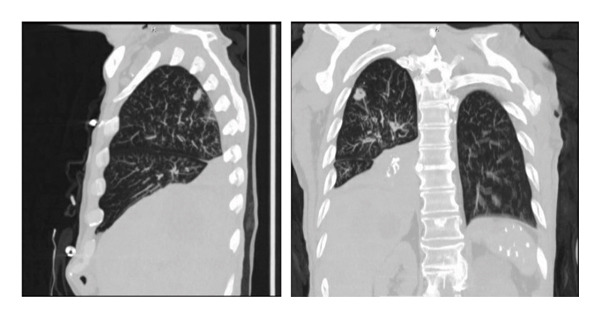 Figure 2
Figure 2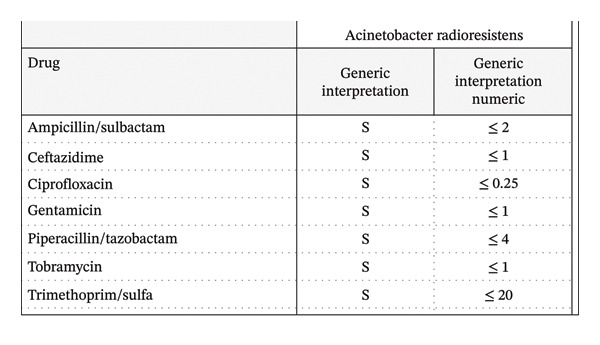 Figure 3
Figure 3| Hospital day | Clinical event | Diagnostic findings | Interventions and management |
|---|---|---|---|
| Day 1 | Presentation from group home with shortness of breath, hypotension, and hypoxia | Labs: Leukocytosis, AKI, lactic acidosis. Imaging: CXR/CT with RLL opacification | Admission to MICU, intubation, vasopressors initiated. Empiric antibiotics: Vancomycin and Cefepime. Blood cultures drawn |
| Day 2 | Blood cultures are reported as positive | VERIGENE BC‐GN: | Continued empiric antibiotics and supportive care |
| Day 4 | Initial clinical improvement noted | MALDI‐TOF and VITEK 2: Confirmed as pan‐susceptible | Antibiotic regimen de‐escalated to IV ampicillin/sulbactam |
| Day 5–11 | Patient improved, weaned off vasopressors and oxygen support. Successfully extubated | Completed 8‐day course of targeted IV ampicillin/sulbactam | |
| Day 12 | Sudden clinical deterioration with recurrent hypoxemic respiratory failure | Re‐intubation and vasopressor support resumed. Family discussion regarding poor prognosis. Transition to comfort care. Withdrawal of life support. Patient expires |
| Case | Age | Sex | Comorbidities | Treatment | Outcome |
|---|---|---|---|---|---|
| Wang et al. [ | 71 | Female | Adenocarcinoma of the lung | Ampicillin‐sulbactam 3 g q6h for 14 days | Deceased |
| Lopes et al. [ | 71 | Male | Alzheimer’s, Parkinson’s | Ceftriaxone | Survived |
| Visca et al. [ | 32 | Female | HIV | Ciprofloxacin 400 mg BID for 14 days | Survived |
| Tan et al. [ | 55 | Male | Tobacco abuse | IV ampicillin‐sulbactam 3 g q6h for 1 week followed by PO ampicillin‐sulbactam 750 mg BID for 1 week | Survived |
| Brady et al. [ | 53 | Female | Li‐Fraumeni syndrome, colon/breast/adrenal/bone cancer | Ceftriaxone and ampicillin‐sulbactam | Survived |
| 60 | Male | Diabetes, ESRD | Cefepime | Survived | |
| Savov et al. [ | 85 | Male | COPD, CHF | Ceftriaxone 1 g BID and Gentamicin 80 mg | Deceased |
| Verma et al. [ | 61 | Male | COPD, Hepatitis C | Ampicillin‐sulbactam for 14 days | Survived |
| Lazarev et al. [ | 83 | Male | CHF, CAD, COPD | Ceftriaxone 2 g and azithromycin 500 mg | Survived |
| Our case | 77 | Male | Adenocarcinoma of the lung with metastasis to the liver | Ampicillin‐sulbactam 3 g q6h for 8 days and Flagyl 500 mg q8h for 2 days | Deceased |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Resistance in Bacteria · Infections and bacterial resistance · Bacterial Identification and Susceptibility Testing
1. Introduction
The genus Acinetobacter consists of Gram‐negative coccobacilli that are a growing concern as a cause of hospital‐acquired infections. While Acinetobacter baumannii is the most prevalent and notorious species due to its multidrug resistance, other species within the genus are increasingly recognized as opportunistic pathogens. Acinetobacter radioresistens is one such organism, typically considered to have low virulence but capable of causing serious infections in immunocompromised hosts. Accurate and rapid identification of bacterial pathogens in bloodstream infections is crucial for guiding appropriate antibiotic therapy. This case report describes a case of bacteremia and pneumonia caused by A. radioresistens in a patient with multiple comorbidities, highlighting the diagnostic pathway and the importance of advanced microbiological techniques in clinical management. This case report has been prepared in accordance with the CARE guidelines (see Supporting Information [available here]).
2. Presentation of Case
A 77‐year‐old male with adenocarcinoma of the lung and liver metastasis, presented from a group home due to shortness of breath. His cancer diagnosis was recent, and he had not yet undergone chemotherapy or radiation. His additional comorbidities included COPD, dementia, and history of alcohol abuse. Physical examination revealed he was afebrile, tachypneic (31 breaths/min), hypoxic (85% saturation on room air), and hypotensive (77/61 mm Hg). Crackles were noted in the upper right lung lobe. He was initially placed on a nonrebreather mask, but his respiratory support was escalated to BIPAP therapy. Due to progressive fatigue on BIPAP, he was subsequently intubated. His laboratory evaluation was significant for leukocytosis of 14.89 × 10^3^/μL, hypoglycemia 55 mg/dL, acute kidney injury (creatinine 2.5 mg/dL; baseline 0.8 mg/dL), hypernatremia 162 mg/dL, hyperkalemia 5.5 mg/dL, anion gap metabolic acidosis (AGAP 30, bicarb 10 mmol/L, lactic acid 18.5 mmol/L), and transaminitis (Alk Phos 440 U/L, AST 552 U/L, ALT 117 U/L). Venous blood gas showed metabolic acidosis with a pH of 7.15, pCO_2_ 32 mmHg, bicarb 11.1 mmol/L, and lactic acid of 17.0 mmol/L. Chest X‐ray (Figure 1) revealed a retrocardiac opacity consistent with lobar atelectasis, potentially postobstructive. Noncontrast CT of the thorax (Figure 2) revealed complete opacification of the right lower lobe and a 1.5 cm solid pulmonary nodule in the right upper lobe, along with multiple smaller nodules throughout the right lung. Noncontrast CT of the abdomen and pelvis showed findings of colitis and multiple hypoattenuating liver lesions, suggestive of cholangiocarcinoma or metastasis. The patient was admitted to the medical intensive care unit for acute hypoxic respiratory failure requiring mechanical ventilation. Vasopressors were initiated for persistent hypotension despite fluid resuscitation. Empiric antibiotic therapy with vancomycin (1000 mg IVPB) and cefepime (1000 mg IVPB) was initiated.
Retrocardiac opacity consistent with lobar atelectasis, possibly postobstructive.
Complete opacification of the right lower lobe of the lung, and a 1.5 cm solid pulmonary nodule within the right upper lobe of the lung with multiple smaller nodules throughout the right lung.
Gram stain of one of two positive blood cultures (aerobic bottle) obtained on admission was positive but initially untypable by standard microbial testing. Tracheal aspirate and sputum cultures grew Klebsiella pneumoniae. VERIGENE molecular testing of the blood cultures identified an Acinetobacter species [1] that was negative for resistance markers CTX‐M, KPC, IMP, NDM, OXA, and VIM. This was subsequently identified as Acinetobacter radioresistens by MALDI‐TOF mass spectrometry, demonstrating pan‐susceptibility to ampicillin/sulbactam, ceftazidime, ciprofloxacin, gentamicin, piperacillin/tazobactam, tobramycin, and trimethoprim/sulfamethoxazole. Antimicrobial susceptibility testing was performed by the VITEK 2 system according to the Clinical and Laboratory Standards Institute (CLSI) guidelines (Figure 3). He was treated with an eight‐day course of intravenous ampicillin‐sulbactam (3 g every 8 h) and a two‐day course of metronidazole (500 mg every 8 h).
Antimicrobial susceptibility profile of the Acinetobacter radioresistens isolate from the patient’s blood culture, as determined by minimum inhibitory concentrations (MICs) according to CLSI guidelines.
The patient initially showed improvement following antibiotic initiation and was weaned off vasopressor and oxygen support. His subsequent clinical course was complicated by a sudden hypoxemic respiratory failure, again necessitating vasopressor support and mechanical ventilation. Given the patient’s poor prognosis, diminished quality of life, and multiple comorbidities, his family elected for hospice and comfort care and to withdraw life support. The patient expired shortly after the withdrawal of life support. It remained unclear whether the patient’s death was attributable to the infectious process, given his initial improvement with antibiotics, or to the progression and complications of his metastatic disease. A detailed timeline of the patient’s clinical course is provided in Table 1.
3. Discussion
Acinetobacter are aerobic, oxidase‐negative, Gram‐negative, nonmotile coccobacilli. While generally considered to have low virulence, they are capable of causing significant infections in immunocompromised and neutropenic patients [2]. Risk factors for Acinetobacter infections include prolonged ICU stays, prolonged antibiotic exposure, mechanical ventilation, central venous catheter use, and hemodialysis [3]. Acinetobacter infections are associated with high morbidity and mortality rates, reportedly up to 70% in patients with multiorgan dysfunction [3]. To our knowledge, this represents the tenth reported case of Acinetobacter radioresistens isolated from culture, with seven of these cases reportedly achieving successful treatment (Table 2).
For timely and appropriate antibiotic administration, accurate and rapid identification of bacterial pathogens in bloodstream infections is crucial. In this case, Acinetobacter radioresistens was identified using the VERIGENE System [11]^,^ which is a multiplexed nucleic acid microarray platform that allows for the simultaneous detection of different pathogens and resistance markers directly from positive blood cultures. This provides results faster than traditional culture‐based methods and consists of automated nucleic acid extraction, hybridization to species‐specific probes on a microarray, and nanoparticle‐based detection.
The ability of the VERIGENE system for detecting Acinetobacter radioresistens at the species level reliably depends on the specific panel used. The VERIGENE Gram‐Negative Blood Culture (BC‐GN) panel usually targets common bloodstream pathogens. The inclusion and validation of probes that are specific for A. radioresistens can vary. The successful identification in this case supports the evidence that the panel utilized has the capability to detect this species. However, if clinical suspicion for less common organisms arises, confirmation with alternative methods may be warranted.
The most suitable methods for accurate identification of Acinetobacter radioresistens currently include conventional culture with biochemical identification [12], which is the foundational approach, and Matrix‐Assisted Laser Desorption/Ionization Time‐of‐Flight Mass Spectrometry (MALDI‐TOF MS) [13], which is known for its rapid and generally accurate identification of Acinetobacter species.
High resolution for species identification can be obtained through molecular methods such as PCR and sequencing of housekeeping genes [14] (e.g., rpoB, gyrB, and 16S rRNA). Even though the VERIGENE system serves as a rapid diagnostic tool, it is important to be aware of the coverage of the specific assay used for common pathogens and the need for supplementary methods for instances where unexpected isolates like A. radioresistens are encountered.
Acinetobacter baumannii has become a significant cause of hospital‐associated infections in recent years [15]. The Acinetobacter genus exhibits intrinsic resistance to ampicillin, first‐ and second‐generation cephalosporins, aztreonam, and ertapenem. The acquisition and expression of carbapenem‐hydrolyzing oxacillinases contributes to the carbapenem resistance in Acinetobacter baumannii. Acinetobacter radioresistens isolates have the bla‐OXA‐23 gene chromosomally encoded, which is implicated in the carbapenem resistance [16, 17].
Acinetobacter radioresistens is rarely identified as the causative agent of bacterial pneumonia. They are commonly found in the environment and are known to colonize human skin and the respiratory tract. While acknowledging the presence of Klebsiella pneumoniae in the patient’s pulmonary samples, which could contribute to the pneumonia, its isolation from the bloodstream makes Acinetobacter radioresistens is a clinically significant finding. Even though it has low virulence, its presence in an immunocompromised patient with severe pneumonia and sepsis, coupled with a positive blood culture confirmed by molecular methods and an initial rapid response to targeted antibiotics (ampicillin‐sulbactam, to which the A. radioresistens was fully susceptible), suggests it was the likely cause of bacteremia and sepsis in this setting. The critical clinical presentation of the patient aligns with a significant bloodstream infection, making simple blood culture contamination less likely in this context. The ability of this species to harbor the carbapenem resistance genes throws light on a significant pathway through which less virulent Acinetobacter species can contribute to the escalating antimicrobial resistance problem. Even though only one blood culture was positive for Acinetobacter radioresistens, the severity of the clinical presentation combined with the molecular identification of the species and the initial improvement to antibiotics, supports the diagnosis of A. radioresistens bacteremia.
In the case presented, the patient had several risk factors for Acinetobacter infection, including immunocompromised status, metastatic disease, mechanical ventilation, and ICU admission. Having any one of these risk factors increases the probability of acquiring an Acinetobacter infection. Comparison with other reported cases of Acinetobacter radioresistens isolation reveals that most, if not all, patients had comorbidities predisposing them to pulmonary compromise. This includes lung adenocarcinoma, COPD, Alzheimer’s/Parkinson’s (associated with increased risk of aspiration), tobacco use and immunocompromised status. Despite being rare, clinicians should remain vigilant for Acinetobacter radioresistens infections in patients with the risk factors mentioned and to tailor antibiotic therapy accordingly to reduce disease burden. Given that these infections mostly result from colonization and nosocomial spread [3], there should be measures taken to prevent colonization through appropriate isolation measures. In the absence of these measures, it can contribute to the further emergence of carbapenem‐resistant Acinetobacter species.
4. Conclusion
Our case highlights Acinetobacter radioresistens as a cause of bacteremia and significant pneumonia necessitating mechanical ventilation. Accurate identification was achieved using VERIGENE, a nucleic acid microarray capable of rigorously detecting pathogens and resistance markers. We highlight the importance of precise identification of pathogens, including profiling antibiotic resistance, in the management of critically ill patients. Molecular assays, such as VERIGENE, should be incorporated as an integral step when performing a comprehensive evaluation of such patients. This will allow us to understand the pathogenesis of Acinetobacter radioresistens, which may become more prevalent due to the increasing incidence of poor antimicrobial stewardship. We would also like to highlight the presence of Acinetobacter radioresistens infections in those with comorbidities which affect the lung. Further investigation is needed to determine if these comorbidities independently increase the risk of acquiring Acinetobacter radioresistens infection, or if their increased susceptibility is associated with their need for higher levels of care such as mechanical ventilation and ICU care.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not‐for‐profit sectors.
Ethics Statement
As the data was fully de‐identified and the report was retrospective in nature, patient consent was not obtained. Patient privacy and confidentiality were maintained throughout the preparation of this case report.
Consent
No written consent has been obtained from the patients as there is no patient identifiable data included in this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting Information
The CARE checklist for this case report is provided as a supporting file (CARE Checklist.pdf).
Supporting information
Supporting Information Additional supporting information can be found online in the Supporting Information section.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fournier P. E. , Richet H. , and Weinstein R. A. , The Epidemiology and Control of Acinetobacter baumannii in Health Care Facilities, Clinical Infectious Diseases. (2006) 42, no. 5, 692–699, 10.1086/500202, 2-s 2.0-33144460009.16447117 · doi ↗ · pubmed ↗
- 2Wang T. , Costa V. , Jenkins S. G. , Hartman B. J. , and Westblade L. F. , Acinetobacter radioresistens Infection With Bacteremia and Pneumonia, ID Cases. (2019) 15, 10.1016/j.idcr.2019.e 00495, 2-s 2.0-85062395261.PMC 641150430906692 · doi ↗ · pubmed ↗
- 3Playford E. G. , Craig J. C. , and Iredell J. R. , Carbapenem-Resistant Acinetobacter baumannii in Intensive Care Unit Patients: Risk Factors for Acquisition, Infection and Their Consequences, Journal of Hospital Infection. (2007) 65, no. 3, 204–211, 10.1016/j.jhin.2006.11.016.17254667 · doi ↗ · pubmed ↗
- 4Lopes M. C. , Évora B. S. , Cidral T. A. et al., Bloodstream Infection by Acinetobacter Radioresistens: the First Case Report in Brazil, Jornal Brasileiro de Patologia e Medicina Laboratorial. (2019) 55, 667–672, https://www.scielo.br/j/jbpml/a/MVHWH Lm MCH Jkbxgd 3nr KMVK/?format=html%26lang=en.
- 5Visca P. , Petrucca A. , De Mori P. et al., Community-Acquired Acinetobacter radioresistens Bacteremia in an HIV-Positive Patient, Emerging Infectious Diseases. (2001) 7, no. 6, 1032–1035, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 2631918/pdf/11747736.pdf, 10.3201/eid 0706.010621, 2-s 2.0-0035202733.11747736 PMC 2631918 · doi ↗ · pubmed ↗
- 6Tan T. , Yh Y. H. , Quah Q. et al., Community-Acquired Pneumonia With Acinetobacter radioresistens Bacteremia in an Immunocompetent Host: A Case Report, Asian Pacific Journal of Tropical Medicine. (2019) 12, no. 6, 10.4103/1995-7645.261308, 2-s 2.0-85068708556. · doi ↗
- 7Brady A. C. , Lewis J. S. , and Pfeiffer C. D. , Rapid Detection of bla OXA in Carbapenem-Susceptible Acinetobacter radioresistens Bacteremia Leading to Unnecessary Antimicrobial Administration, Diagnostic Microbiology and Infectious Disease. (2016) 85, no. 4, 488–489, 10.1016/j.diagmicrobio.2016.04.025, 2-s 2.0-84970044578.27236714 · doi ↗ · pubmed ↗
- 8Savov E. , Pfeifer Y. , Wilharm G. et al., Isolation of Acinetobacter radioresistens From a Clinical Sample in Bulgaria, The Journal of Global Antimicrobial Resistance. (2016) 4, 57–59, 10.1016/j.jgar.2015.10.008, 2-s 2.0-84949818828.27436395 · doi ↗ · pubmed ↗