Primary Dedifferentiated Liposarcoma of the Duodenum: A Report of a Rare Case With a Review of the Literature
Kayra Cangoz, Muhammed Bahadir Avci, Merve Meryem Kiran, Firathan Sarialtin

TL;DR
A rare case of primary dedifferentiated liposarcoma in the duodenum is reported, highlighting the disease's aggressive nature and diagnostic challenges.
Contribution
This report adds a new clinical case of primary duodenal dedifferentiated liposarcoma and emphasizes its diagnostic and therapeutic difficulties.
Findings
DDLPS is an aggressive malignancy with high recurrence and metastasis risks.
The patient's case highlights the lack of standardized treatment for DDLPS.
DDLPS should be considered in the differential diagnosis of duodenal masses.
Abstract
Primary and metastatic tumors of the duodenum are rare, and primary duodenal dedifferentiated liposarcomas (DDLPS) of this region are exceptionally uncommon. DDLPS is an aggressive malignancy characterized by a high risk of recurrence and metastasis. This report describes the case of a 43-year-old woman who presented with a 20-day history of isolated abdominal pain. CT images demonstrated a 68 x 120 mm lesion involving the distal portions of the duodenum. Intraoperatively, the lesion was found to be confined to the third and fourth portions, and a segmental duodenal resection with duodenojejunostomy using a circular stapler was performed. During the postoperative period, the patient experienced transient cholestatic findings likely secondary to papillary obstruction. After clinical improvement, she was lost to follow-up for seven months during doxorubicin therapy and later re-presented…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
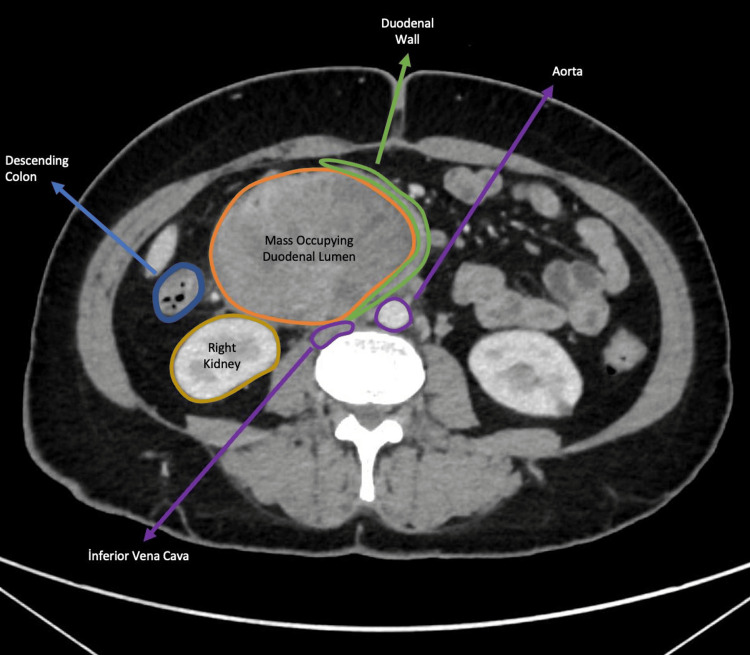 Figure 1
Figure 1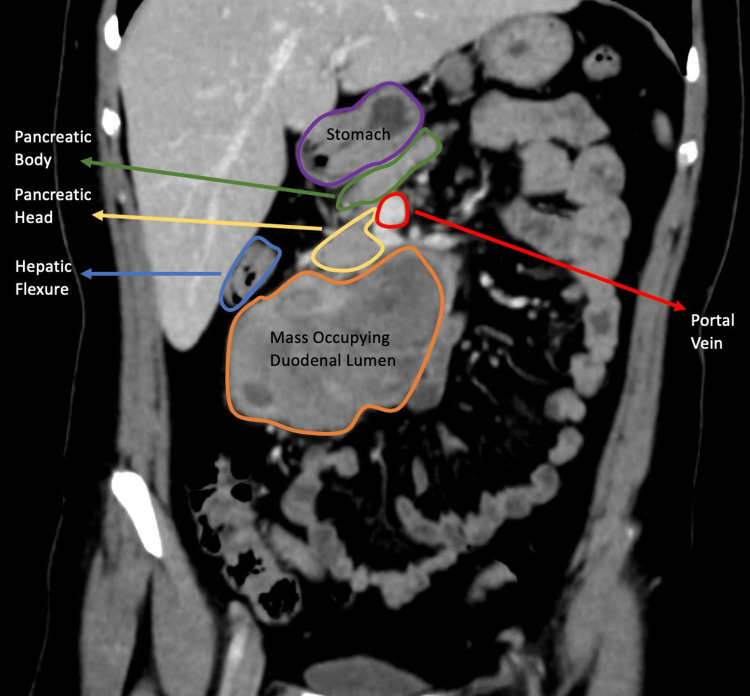 Figure 2
Figure 2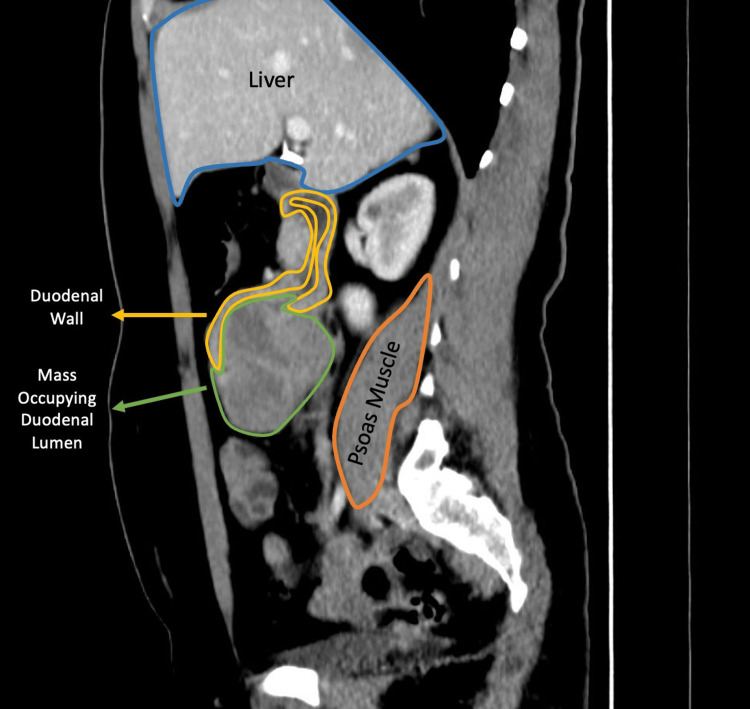 Figure 3
Figure 3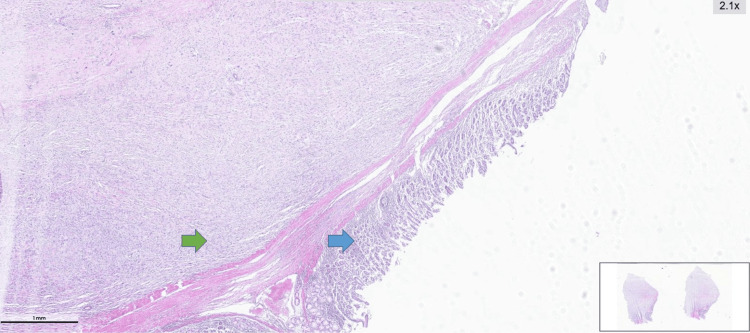 Figure 4
Figure 4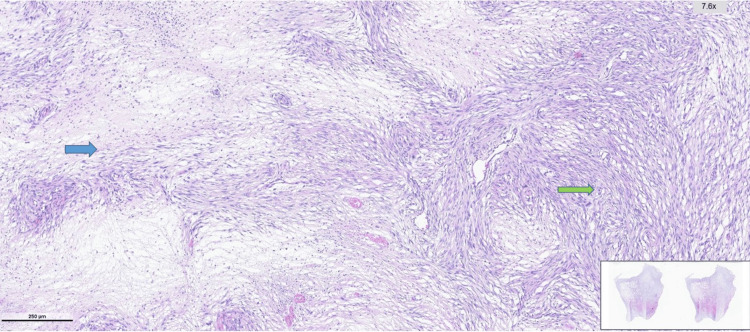 Figure 5
Figure 5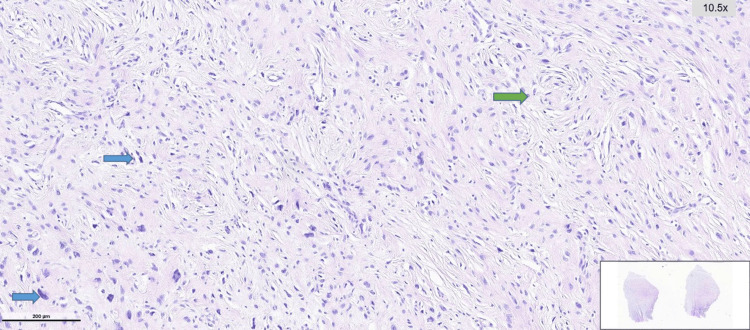 Figure 6
Figure 6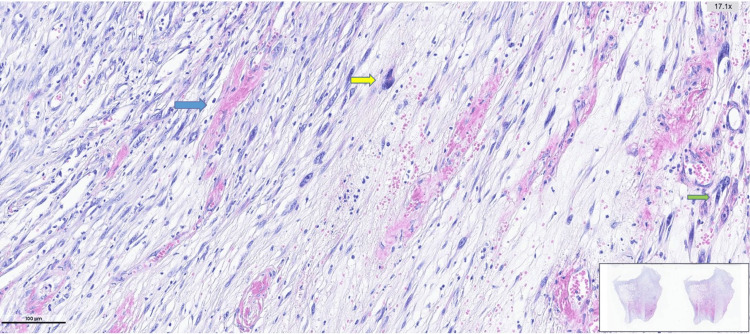 Figure 7
Figure 7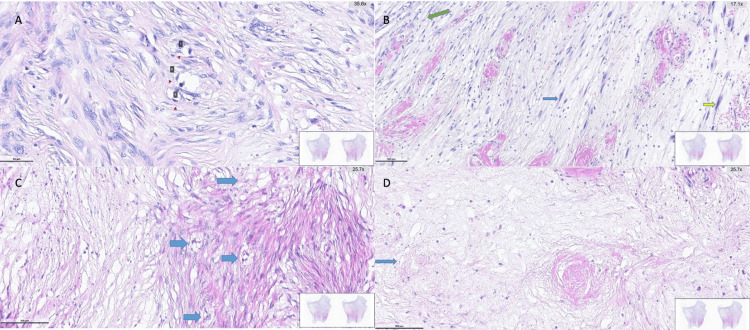 Figure 8
Figure 8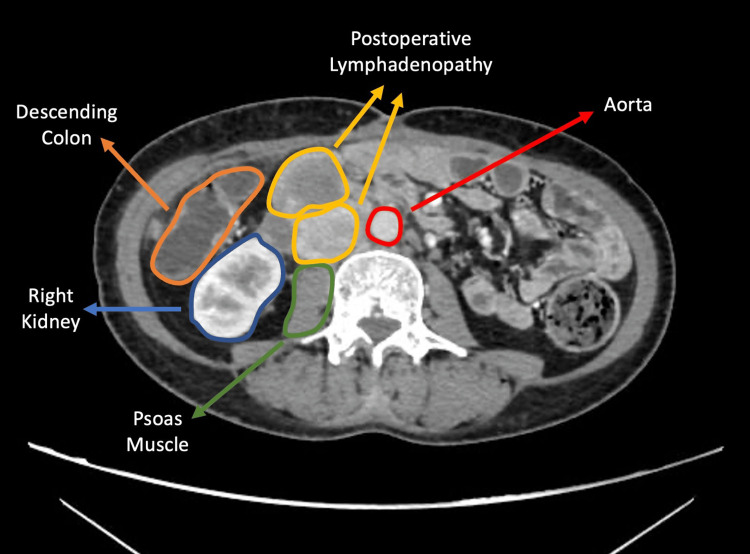 Figure 9
Figure 9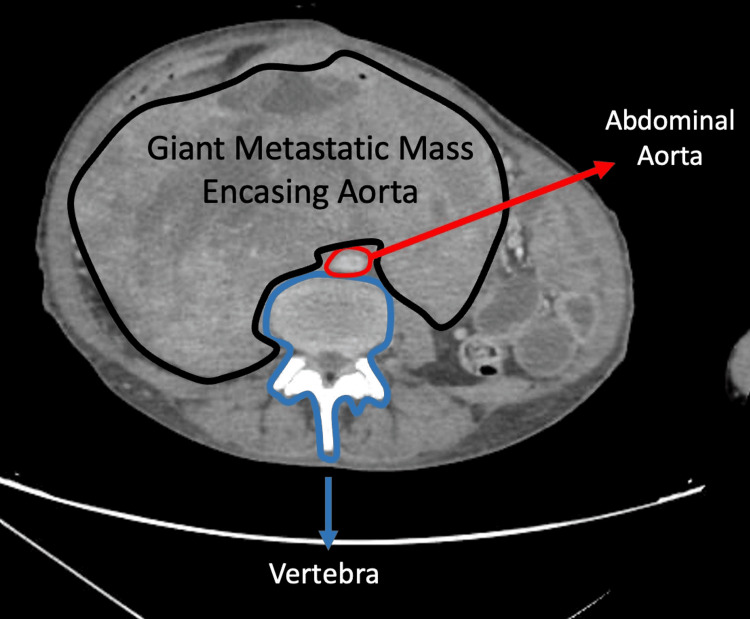 Figure 10
Figure 10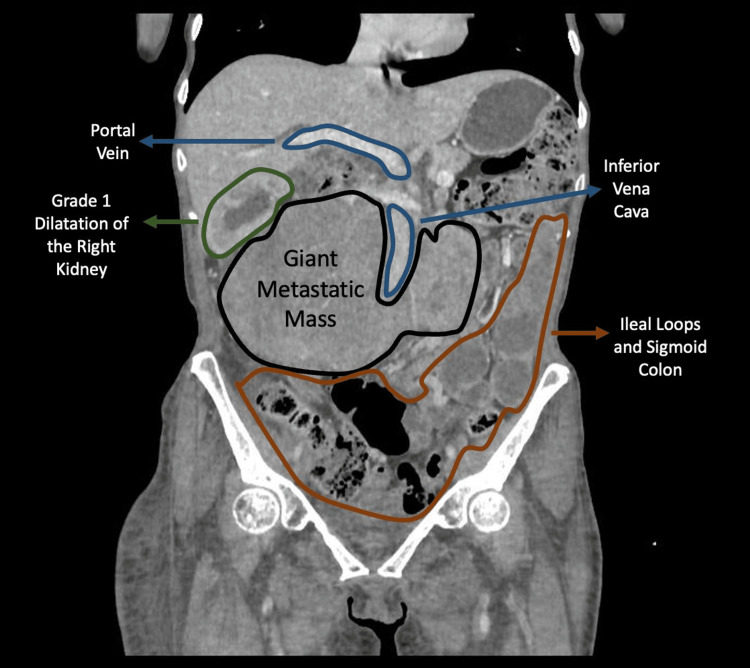 Figure 11
Figure 11| Author(s), Year | Age (years)/ Sex | Presentation | Tumor Size & Location | Surgery / Treatment | Outcome |
| Okabayashi et al., 2013 [ | 55/M | Melena | 9.5 cm – 2nd portion of duodenum; invasion to transverse colon; CBD dilatation | Emergency pylorus-preserving pancreaticoduodenectomy + Partial transverse colon resection | No recurrence at 10 months |
| Whitham et al., 2020 [ | 59/F | Fatigue, SOB, Anemia (Hb: 6.9) | 5.2 x 4.9 x 4.8 cm – duodenal bulb (1stportion), ulcerated | Segmental duodenal resection + Distal gastrectomy (Roux-en-Y) | No recurrence or metastasis at 16 months |
| Kim et al., 2022 [ | 64/M | 7-day abdominal pain, weight loss | 3 cm – pancreaticoduodenal groove causing obstruction of 2ndportion, invasion to the pancreas, hepatic flexure and adjacent major vessels | Pylorus-preserving pancreaticoduodenectomy + En bloc right hemicolectomy + SMV segmental resection + IVC wedge resection | Complicated postoperatively, died on postoperative day 60 due to DIC |
| Alvi and Shankar, 2023 [ | 66/F | Syncope, Melena (Hb: 5.2) | 6.5 x 4.7 cm – superior duodenal wall; concurrent liver lesion | Arterial embolization for bleeding + GJ for GOO | Long-term outcome not reported |
| Noguchi et al., 2025 [ | 51/F | Syncope (Hb: 4.5) | 7 cm – horizontal part; multiple pancreatic and mesenteric lesions | Unresectable – RT + Eribulin chemotherapy + GJ | Died 9 months after diagnosis |
| Present Case (Cangoz et al.), 2026 | 43/F | 20-day abdominal pain | 68 x 120 mm – distal 2nd and 3rd portions of duodenum (intraoperative 3rd and 4th portions only) | Segmental duodenal resection (3rd and 4thportions) + duodenojejunostomy using circular stapler | Transient papillary obstruction; Lost to follow-up; Massive metastatic relapse; Died at 12 months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Gastrointestinal Tumor Research and Treatment · Cardiac tumors and thrombi
Introduction
Liposarcomas are among the most common malignant soft tissue tumors, and they predominantly occur in the retroperitoneum, extremities, and deep soft tissue of the trunk [1,2]. According to the 2020 World Health Organization Classification of Soft Tissue Tumors, malignant adipocytic tumors are classified into well-differentiated liposarcoma, dedifferentiated liposarcoma (DDLPS), myxoid liposarcoma, pleomorphic liposarcoma, and myxoid pleomorphic liposarcoma [3]. Primary and metastatic tumors of the duodenum are very rare [4]. Primary duodenal DDLPS tumors are extremely rare, aggressive tumors characterized by a high risk of recurrence and distant metastasis [5-8].
The standard treatment for DDLPS is wide-margin surgical resection similar to other sarcomas [7]. Surgical treatment of duodenal tumors is extremely important since the duodenum is located in the center of major structures and involves major operations such as the Whipple procedure [4]. The prognosis and treatment protocol of DDLPS are unclear due to the low number of cases documented in the literature. To the best of our knowledge, there are only five previously reported cases of DDLPS in the English literature [2,6-9]. The present report describes the case of a patient presenting with abdominal pain who was diagnosed with a duodenal DDLPS, together with the treatment strategy applied. We are reporting this case to add another documented example of primary DDLPS to the literature, which is an exceptionally uncommon entity. We also aim to share some diagnostic and perioperative insights that may help clinicians in the decision-making process when encountering similar cases.
Case presentation
A 43-year-old female patient presented to the emergency department with a 20-day history of abdominal pain. Her general condition was good, and her vital signs were stable. CT imaging revealed a heterogeneous soft tissue mass measuring 68 x 120 mm in the distal second and third parts of the duodenum. Duodenal luminal dilatation was observed at the level of the lesion, and multiple enlarged lymph nodes, the largest being 12 mm in diameter, were detected near the superior mesenteric artery (Figures 1-3). Upper endoscopy revealed a 6-cm lesion in the second part of the duodenum that prevented the passage of the endoscope. Biopsies were taken, and the result was reported as a malignant mesenchymal tumor consistent with DDLPS.
Post-contrast axial CT image demonstrating an intraluminal duodenal mass.A heterogeneously enhancing solid mass is seen within the duodenal lumen. No component extends beyond the lumen.
Contrast-enhanced coronal CT image of an intraluminal duodenal massA large heterogeneously enhancing intraluminal duodenal mass is seen. Distally, the lesion extends along the lumen and forms an acute angle with the duodenal wall.
Contrast-enhanced sagittal CT image of a polypoid intraluminal duodenal massA large heterogeneously enhancing intraluminal duodenal mass is seen. The lesion projects into the lumen in a polypoid fashion from the posterior wall, and its proximal margin forms an acute angulation with the duodenal wall.
After the biopsy, further surgical intervention was planned. During the operation, it was observed that the mass did not extend to the second portion of the duodenum and was confined to the third and fourth parts. Therefore, a Whipple procedure was not performed. In order to preserve the pancreas and the ampulla of Vater, the third and fourth parts of the duodenum were resected, and a duodenojejunostomy anastomosis was created using a circular stapler.
Final pathology revealed atypical cells with increased MDM2 signal activity, consistent with DDLPS. Tumor cells were positive for Vimentin. The tumor cells were negative for C-kit, Desmin, SMA, S-100, Pancytokeratin, DOG1, Factor XIIIa, MUC4, ALK, SOX10, Melan-A, and HMB-45. The closest surgical margin measured 3 cm, and the tumor dimensions were 12 x 7 x 5 cm. The tumor invaded the muscularis propria, submucosa, and, focally, the mucosa. No tumor involvement was identified at the surgical margins (Figures 4-6). Cellular atypia was evident (Figure 7). Necrosis and atypical mitotic figures were identified (Figure 8).
Histopathological appearance of the dedifferentiated liposarcoma showing preserved surface epithelium and an underlying spindle cell neoplastic proliferation.Blue arrow: Preserved surface epithelium. Green arrow: A well-circumscribed neoplastic proliferation composed of spindle cells, clearly demarcated from the epithelium.
Hematoxylin and eosin–stained sections showing spindle cell neoplastic proliferation with alternating hypocellular and hypercellular areasBlue Arrow: Hypocellular area. Green Arrow: Hypercellular area
Hematoxylin and eosin–stained section showing spindle cell neoplastic proliferation with focal whorled architecture and short fascicular arrangementsBlue Arrow: Areas with hyperchromatic and pleomorphic tumor cells. Green Arrow: Focal storiform growth pattern
Hematoxylin and eosin–stained section showing spindle cell neoplastic proliferation with prominent vascularitySpindle cell neoplastic proliferation is with alternating hypocellular and hypercellular areas. Areas with prominent vascularity composed of spindle cells exhibiting hyperchromatic and pleomorphic nuclei are observed.Blue Arrow: Dilated, congested vascular structures. Yellow and Green Arrows: Hyperchromatic, pleomorphic tumor cells.
Histopathological features of dedifferentiated liposarcoma on hematoxylin and eosin staining (A) Arrows indicate lipoblasts; (B) Blue and yellow arrows indicate pleomorphic spindle-to-oval tumor cells; green arrow indicates inflammatory cells; (C) Blue arrows indicate lipoblasts characterized by vacuolated cytoplasm and centrally located nucleoli; (D) Necrotic area within the tumor.
Examination of 14 lymph nodes revealed no metastasis. Based on the American Joint Committee on Cancer (AJCC) soft tissue sarcoma staging system [10], the specimen corresponded to pT3N0M0. No vascular invasion was observed. Cellular atypia was evident. Necrosis and atypical mitotic figures were identified. Ki-67 proliferation index was 28%. Fluorescence in situ hybridization (FISH) performed using the Kreatech™ MDM2 (12q15)/SE 12 (Leica Biosystems Nussloch GmbH, Nussloch, Germany) set on a ThermoBrite® Elite system (Leica Biosystems Nussloch GmbH) demonstrated increased MDM2 signal activity in atypical tumor cells, confirming gene amplification. On postoperative day 8, the patient was discharged without complications.
On postoperative day 13, she presented to the emergency department again with abdominal pain. Laboratory tests showed elevated bilirubin levels (total bilirubin: 6.4 mg/dL and direct bilirubin: 5.0 mg/dL; adult female reference ranges: total 0.3-1.2 mg/dL, direct < 0.0.3 mg/dL), along with increased amylase, lipase, liver function tests, and cholestatic markers. Abdominal CT demonstrated increased pancreatic duct caliber, and hepatic ultrasonography revealed a proximal common bile duct diameter of 15 mm. This presentation was considered consistent with transient papillary obstruction due to inflammatory edema of the residual duodenal segment. She was admitted to the hospital and evaluated by the interventional radiology department. Due to no contrast passage from papilla to duodenum and the presence of intrahepatic and extrahepatic ductal dilatation, percutaneous transhepatic cholangiography (PTC) and external drainage were performed.
On postoperative day 25, she developed nausea and vomiting. She underwent upper gastrointestinal (GI) endoscopy, which showed no pathology at the anastomosis. Subsequently, endoscopic retrograde cholangiopancreatography (ERCP) was performed. Blue dye injected through the PTC catheter was observed entering the duodenum during the procedure; however, the papilla could not be visualized. By the second postoperative month, her bilirubin levels had normalized, but she required a secondary operation. Due to increased intra-abdominal inflammation, hepaticojejunostomy (HJ) could not be performed, and a gastrojejunostomy (GJ) was created.
During her admission, her general status worsened in the third postoperative month, and she was transferred to the intensive care unit (ICU). During her ICU stay, she experienced seizures, which were evaluated by the neurology department and diagnosed as neuropathy of chronic disease. After a 10-day ICU admission, she was transferred back to the ward, and her general condition improved. Following normalization of her blood tests and clinical stabilization, her external drain was removed, and she was discharged.
Her prolonged postoperative hospitalization and subsequent development of significant cachexia after discharge resulted in poor functional status, limiting her eligibility for immediate adjuvant therapy. In the fifth postoperative month, she presented to the oncology department, and her follow-up CT imaging revealed three lymph nodes anterior to the inferior vena cava (IVC) at the level of the left renal hilum, the largest measuring 35 × 27 mm, exerting pressure on the IVC (Figure 9). Following multidisciplinary tumor board evaluation, single-agent doxorubicin therapy was recommended while immediate radiotherapy was not planned, considering the patient’s clinical condition and tumor-related features.
Contrast-enhanced axial CT image showing retroperitoneal lymphadenopathyLymphadenopathies are seen anterior to the psoas muscle at the level of the renal hilum
Shortly thereafter, the patient relocated to another city to continue treatment, interrupting her planned care at our center. She was subsequently lost to follow-up until 12 months postoperatively. Her CT imaging at that time, when she presented with bilateral grade-3 edema, revealed a 22 mm metastatic lesion in liver; a 20 x 15 x 20 cm metastatic lesion extending from the duodenum to the IVC and encasing the aorta 270 degrees (Figures 10, 11); a 21 mm metastatic nodule in right kidney invading the right renal artery and vein; and dilatation of the portal and splenic veins. Following these findings, she was referred to palliative care and subsequently died.
Contrast-enhanced axial CT image demonstrating a large retroperitoneal massPost-contrast axial image showing a large mass encasing the aorta, extending into the paravertebral region, filling the right hemiabdomen, and displacing the small-bowel loops to the left
Contrast-enhanced coronal CT image demonstrating a large retroperitoneal massPost-contrast coronal image demonstrating an enlarged mass encasing the aorta and dispşacing the right kidney superiorly
Discussion
Primary liposarcomas located in the GI tract are extremely rare [2]. Furthermore, primary DDLPS is considered the rarest type of GI liposarcomas [8]. To the best of our knowledge, only five cases of primary duodenal DDLPS have been documented in the English literature [2,6-9]. The present case represents the sixth reported case, and it differs from previously published cases by its surgical management and postoperative course.
Published data indicate that adult soft tissue sarcomas often arise without well-established predisposing risk factors [11]. Our patient similarly had no identifiable environmental, hereditary, or iatrogenic risk factors. Furthermore, DDLPS can present with nonspecific symptoms, and GI stromal tumors (GIST), leiomyosarcoma (LMS), malignant melanoma, and sarcomatoid carcinoma should be considered in the differential diagnosis [2,6]. GISTs typically show expression of CD117, DOG1, and CD34, whereas sarcomatoid carcinomas can be identified by cytokeratin positivity due to their epithelial differentiation. LMS is usually positive for at least one myogenic marker, such as desmin or SMA [2]. Tumors with melanocytic differentiation commonly express S100, SOX10, HMB-45, and Melan-A [3]. In our case, negativity for CD117, DOG1, desmin, SMA, S-100, pancytokeratin, SOX10, Melan-A, and HMB-45, together with increased MDM2 signal activity, supported a definitive diagnosis of DDLPS, which is genomically characterized by amplification of the 12q13-15 region, particularly involving MDM2 and CDK4 [2].
Okabayashi et al. reported the first documented case of primary duodenal DDLPS in the literature. They described a 55-year-old patient with a 9.5 cm lesion located in the second portion of the duodenum, causing dilatation of the common bile duct, and showing invasion into the transverse colon [9]. Due to active hemorrhage, an emergency pylorus-preserving pancreaticoduodenectomy with partial resection of the transverse colon was performed. After a 10-month follow-up period, no recurrence was observed. They noted that endoscopic control of bleeding was difficult, arterial embolization around the duodenum could lead to ischemic necrosis, and catheter-based interventions would be insufficient due to complex arterial anastomoses in this region. Therefore, they concluded that their surgical approach represented the most appropriate technique for hemorrhagic primary duodenal liposarcoma [9].
Whitham et al. reported a case of a 59-year-old female patient who presented to the emergency department with fatigue, shortness of breath, and a hemoglobin level of 6.9 g/dL [8]. Upper endoscopy, performed due to suspicion of GI bleeding, revealed an ulcerated submucosal lesion on the posterior wall of the duodenal bulb. CT imaging confirmed a 5.2 x 4.9 x 4.8 cm heterogeneous mass. During surgery, pancreaticoduodenectomy was avoided since the lesion was confined to the first portion of the duodenum. Instead, they performed segmental duodenal resection and distal gastrectomy with Roux-en-Y reconstruction. The patient experienced no recurrence or distant metastasis during 16 months of postoperative follow-up. The authors emphasized that complete surgical resection remains the gold standard treatment for soft tissue sarcomas and offers the only chance for cure [8].
Kim et al. presented a 64-year-old male patient with a seven-day history of abdominal pain [2]. CT imaging revealed a 3 cm heterogeneous mass in the pancreaticoduodenal groove, causing obstruction of the second portion of the duodenum. Intraoperative findings demonstrated invasion into the pancreas, hepatic flexure, and adjacent major vessels; therefore, the patient underwent pylorus-preserving pancreaticoduodenectomy with en bloc right hemicolectomy, segmental resection of the superior mesenteric vein (SMV), and wedge resection of the IVC. Although the mass was resected, complete removal was not possible because of disseminated disease. The postoperative course was complicated by HJ leakage, peritonitis, sepsis, and multiple reoperations, and the patient died on postoperative day 60 due to disseminated intravascular coagulation. They emphasized that DDLPS of the small intestine may present with nonspecific symptoms and should be considered in the differential diagnosis of duodenal masses [2].
Alvi et al. reported a 66-year-old female patient who presented to the emergency department with syncope and melena with a hemoglobin level of 5.2g/dL [6]. CT imaging revealed a 6.5 x 4.7 cm lobulated soft-tissue mass arising from the superior wall of the duodenum, along with a 4 x 3 cm hepatic lesion. Endoscopy demonstrated a duodenal mass with active bleeding and gastric outlet obstruction. Arterial embolization was performed to control the bleeding, and GJ was subsequently created via laparotomy to address the obstruction. They emphasized that surgical resection is the first-line treatment for soft-tissue sarcomas and that achieving negative surgical margins improves overall survival. They also stated that radiotherapy and doxorubicin-based chemotherapy may provide additional benefit, although treatment should be individualized on a case-by-case basis, given the risk of radiation-related toxicity to intra-abdominal organs [6]. In our patient, immediate postoperative radiotherapy was not administered due to the patient’s postoperative clinical condition and tumor-related features, as concluded by the multidisciplinary tumor board.
Finally, Noguchi et al. described a 51-year-old woman who presented to the emergency department with syncope and a hemoglobin level of 4.5 g/dL [7]. CT imaging demonstrated a 7 cm mass centered in the horizontal portion of the duodenum, accompanied by multiple mesenteric and pancreatic lesions. Endoscopy revealed a solid tumor with active bleeding. A non-surgical approach was adopted, and a GJ was performed to relieve newly developed GI obstruction. The patient subsequently received systemic chemotherapy with eribulin and radiotherapy. However, she died nine months after the initial presentation. The authors noted that this was the first reported duodenal DDLPS managed with a combination of radiotherapy and chemotherapy. They also emphasized that, although surgical resection remains the most effective curative, unresectability may occur in some cases. Duodenal liposarcomas appear to present more frequently with bleeding compared to liposarcomas in other segments of the small intestine, which more commonly cause obstruction [7].
In our case, the patient was the youngest among the previously reported cases and had the largest primary lesion (Table 1). As noted by Noguchi et al. [7], larger liposarcomas may be associated with a higher likelihood of recurrence and mortality, although available data remain limited. This observation may partially explain the aggressive metastatic progression seen in our patient following surgery. Because the tumor did not extend to the second portion of the duodenum, we performed a segmental resection with duodenojejunostomy using a circular stapler. Atie et al. stated that postoperative edema can occur in anastomosis following gastrointestinal surgery and can cause partial obstruction [12]. Additionally, Takada et al. reported that interventions involving the duodenum can lead to papillary edema and subsequent bile-flow obstruction [13]. Considering this mechanism, postoperative edema in the remaining duodenal segment may have transiently obstructed the ampulla of Vater, contributing to the cholestatic findings observed during follow-up.
Although the surgical margins were negative (R0 resection), the locoregional lymph-node recurrences identified at the fifth postoperative month, combined with the patient's subsequent seven-month loss to follow-up, likely allowed the disease, characterized by the inherently aggressive biology of DDLPS, to progress unchecked. By the time of re-presentation at the 12th month, the massive retroperitoneal mass encasing 270 degrees of the aorta and compressing the IVC represented not a continuation of the original lesion, but rather the result of this rapid and destructive recurrence. This case underscores the critical importance of uninterrupted oncologic surveillance and patient adherence following surgery for DDLPS.
Conclusions
We reported a case of primary duodenal DDLPS, an exceedingly rare entity. This case highlights the importance of including DDLPS in the differential diagnosis of duodenal tumors, even in patients presenting with nonspecific symptoms such as isolated abdominal pain. The primary lesion was large, which was followed by rapid metastatic progression and clinical deterioration. Given the rarity, no standardized treatment approach for surgical strategy has been established for duodenal DDLPS. Therefore, we believe that this case adds valuable insight that may assist clinicians in the diagnostic evaluation and management of future patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Primary gastrointestinal liposarcoma-a clinicopathological study of 8 cases of a rare entity Hum Pathol Gajzer DC Fletcher CD Agaimy A Brcic I Khanlari M Rosenberg AE 80939720203188408510.1016/j.humpath.2019.12.004 · doi ↗ · pubmed ↗
- 2Primary duodenal dedifferentiated liposarcoma: a case report and literature review World J Clin Cases Kim NI Lee JS Choi C Nam JH Choi YD Kim HJ Kim SS 200720141020223531713610.12998/wjcc.v 10.i 6.2007 PMC 8891777 · doi ↗ · pubmed ↗
- 3The 2020 WHO classification of soft tissue tumours: news and perspectives Pathologica Sbaraglia M Bellan E Dei Tos AP 708411320213317961410.32074/1591-951X-213PMC 8167394 · doi ↗ · pubmed ↗
- 4Tumor and tumor-like lesions of duodenum: CT and barium imaging features Clin Imaging Wei CJ Chiang JH Lin WC 89962720031263977310.1016/s 0899-7071(02)00494-1 · doi ↗ · pubmed ↗
- 5A rare case report: retroperitoneal dedifferentiated liposarcoma associated with paraneoplastic pemphigus Front Surg Yang F Chen Y Liu J 16908601220254118134610.3389/fsurg.2025.1690860 PMC 12575289 · doi ↗ · pubmed ↗
- 6Primary dedifferentiated duodenal liposarcoma with gastric outlet obstruction: a rare small bowel tumor Cureus Alvi AT Shankar M 015202310.7759/cureus.50978 PMC 1080139438259374 · doi ↗ · pubmed ↗
- 7Primary dedifferentiated liposarcoma of the duodenum with intestinal bleeding: a case report and literature review Intern Med Noguchi Y Abe K Imamura H Hashimoto T Mukai S Ohira H 26202510.2169/internalmedicine.5734-25PMC 1290058540571619 · doi ↗ · pubmed ↗
- 8A case of primary duodenal liposarcoma Case Rep Oncol Whitham Z Blackham A Loven V 6496541320203277425010.1159/000507479 PMC 7383206 · doi ↗ · pubmed ↗