A silent threat: Post-traumatic rib fragments near the ascending aorta
Ana Rodrigo Costa, Catarina Lencastre, Glória Cabral Campello

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
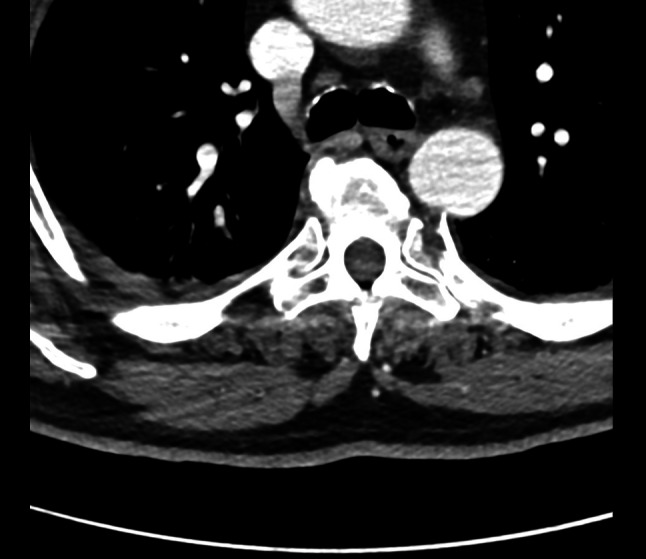 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTrauma Management and Diagnosis · Aortic Disease and Treatment Approaches · Tracheal and airway disorders
A 55-year-old man was admitted to the intensive care unit following a high-energy polytrauma sustained in a bicycle-versus-car road traffic accident. Upon arrival at the emergency room, he was hemodynamically stable, with a GCS score of 15 and no signs of active bleeding. A bedside echocardiogram revealed no significant abnormalities. Imaging studies showed mild bilateral hemopneumothorax and a splenic laceration. Skeletal injuries included an aligned sternal body fracture and multiple bilateral rib fractures, without evidence of instability. Posterior bone fragments from the fractures of the left 5th to 7th ribs were in contact with the posterior wall of the descending thoracic aorta, with a minimum separation of 2 mm (Fig. 1), posing a risk of vascular injury. Given this context, the patient underwent successful surgical excision of the bone fragments by the thoracic surgery team.Fig. 15th left rib in contact with the posterior wall of the descending aorta