CD45-Positive Small Lymphocyte-Like Myeloma with IGH::CCND1 Fusion and TP53 Mutations
Ke Xu, Evan Vitsaras, Anna Childerhouse, Temenuzhka Boneva, Elisabeth Nacheva, Rajeev Gupta

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
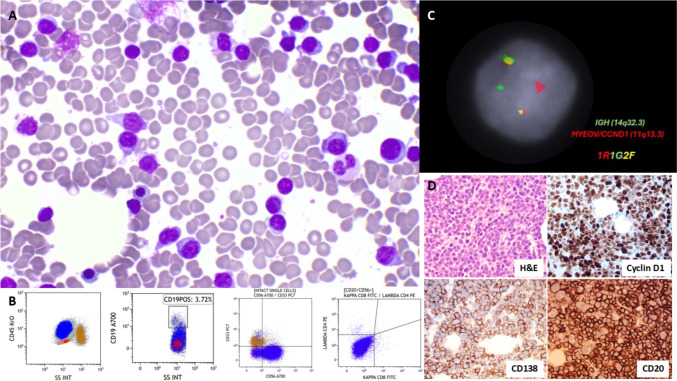 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Protein Degradation and Inhibitors · Peptidase Inhibition and Analysis
A 52-year-old male presented with hypercalcaemia and acute kidney injury. The serum-free kappa chain was 956 mg/L, and the K:L ratio was 119; paraprotein was not detected. A bone marrow aspirate showed excess small lymphocytoid cells (Fig. 1A). They were positive for CD45 and CD56 and negative for CD34, CD19, CD2, CD5, CD7, CD4, CD8, CD33, CD117, CD15, CD13, CD57, surface Ig, MPO, and cTdT (Fig. 1B). Small lymphocyte-like myeloma was suspected, but the addition CD38, CD138 and cytoplasmic Ig could not be performed on flow cytometry due to sample limitation. Targeted CD138 cell FISH showed IGH::CCND1 fusion (Fig. 1C). Trephine IHC showed CD138+, CD56+, cyclin D1+, CD20+, kappa-restricted small plasma cells (Fig. 1D), confirming the diagnosis of myeloma. Lymphoid NGS identified pathogenic TP53 p.Glu285Lys (VAF 62%, COSM10722) and TP53 p.Val272Leu (VAF 19%, COSM10859) variant. The patient had a short response to multiple lines of treatment, refractory to elranatamab and had only two years of overall survival.
Small-lymphocytes-like plasma cell myeloma could mimic mature B-cell lymphoma with or without plasmacytic differentiation. Adding plasma cell markers in the flow panel for lymphoma and adding cytoplasmic kappa/lambda stain in surface Ig-negative cases could help better detect atypical myeloma cases. Small-lymphocytes-like plasma cell myeloma is usually a standard risk with frequent CD20+ and t(11;14) [1]. Detecting pathogenic TP53 variants makes this case high-risk. Gonsalves reported that CD45 expression is an independent poor risk factor of myeloma overall survival in the era of novel treatment agents [2]. This case highlighted the importance of incorporating flow cytometry, molecular testing for diagnosis and full-risk stratification.Fig. 1A Bone marrow aspirate (Giemsa May-Grunwald stain × 100 objective). B Immunophenotyping (blue colour population). C FISH showing IGH::CCDN1 (DAPI staining, × 100 objective, Cytocell probes). D Bone marrow trephine biopsy (× 40 objective) was positive for CD138, cyclin D1, CD20