Understanding an aorto-atrial fistula in a patient with heart failure
Rita Almeida Carvalho, Débora Sá, Pedro Magro, Marisa Trabulo, Miguel Mendes, Regina Ribeiras

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
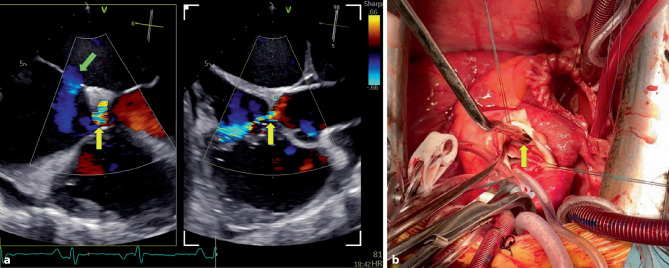 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfectious Aortic and Vascular Conditions · Infective Endocarditis Diagnosis and Management · Coronary Artery Anomalies
A 37-year-old previously healthy man presented with progressive dyspnea, peripheral edema, and weight gain over four months. Examination revealed a continuous heart murmur with pulmonary and peripheral congestion. NT-proBNP was markedly elevated despite high-dose furosemide therapy.
Transthoracic and three-dimensional transesophageal echocardiography (3D TOE) identified an aorto-atrial fistula from the non-coronary sinus of Valsalva to the right atrium (Fig. 1a, yellow arrows; Supplementary Videos 1–4). The fistulous jet coursed parallel to the tricuspid annulus, impinging eccentrically on the right atrial wall. A concomitant 16-mm ostium secundum atrial septal defect produced a significant left-to-right shunt (Fig. 1a, green arrow; Supplementary Videos 2–3). No evidence of endocarditis was found, and the fistula was considered congenital.Fig. 1a Transesophageal echocardiography with color Doppler demonstrating an aorto-atrial fistula from the non-coronary sinus of Valsalva to the right atrium (yellow arrows) and a concomitant ostium secundum atrial septal defect (green arrow). b Intraoperative view showing the fistulous pathway (yellow arrow) during surgical repair
The patient underwent successful surgical repair of both defects (Fig. 1b, yellow arrow showing the fistulous pathway) and was discharged uneventfully. This rare case highlights the crucial role of multimodality imaging in guiding tailored surgical planning.
Supplementary Information
ESM1: Supplementary material 1
ESM2: Supplementary material 2
ESM3: Supplementary material 3
ESM4: Supplementary material 4