Self-efficacy and quality of life mediate self-reported mental health outcomes in visual snow syndrome
Qing Huang, Xuanyue Yu, Haojie Gao, Xiao-xiao Lin, Jing Wang, Ping Su, Xiaofeng Li, Dong Chen, Dirk M. Hermann, Yi Liu

TL;DR
People with visual snow syndrome have lower self-efficacy and quality of life, which may explain their higher risk of depression and suicidal thoughts.
Contribution
This study identifies self-efficacy and quality of life as serial mediators linking visual snow syndrome to mental health outcomes.
Findings
VSS patients had significantly lower self-efficacy and quality of life compared to healthy controls.
Self-efficacy and quality of life sequentially mediate the relationship between VSS and depression or suicidal ideation.
Lower self-efficacy and quality of life may serve as modifiable targets for early intervention in VSS.
Abstract
Visual snow syndrome (VSS) is a chronic neurological disorder associated with impaired mental health. While self-efficacy and quality of life (QOL) are known to influence mental health outcomes (depression and suicidal ideation) in clinical populations, their roles in VSS remain unexplored. This study aimed to examine the associations among VSS, self-efficacy, QOL, mental health outcomes and the potential serial mediation roles of self-efficacy and QOL. A cross-sectional study compared 64 VSS patients and 67 healthy controls matched with age, sex and education level. Participants completed validated questionnaires assessing self-efficacy (GSES), QOL (WHOQOL-BREF), depression (CES-D), and suicidal ideation (BSSI, first five items). Analyses included group comparisons, correlation analyses to examine variable relationships, multimodel linear regression and serial mediation modeling to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
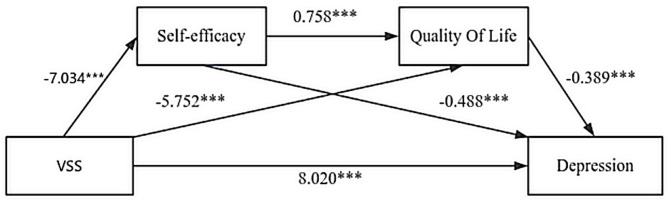 Figure 1
Figure 1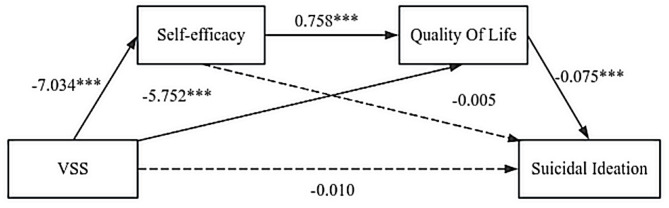 Figure 2
Figure 2- —Revitalisation Talents Program of LiaoNing Province
- —Science and Technology Innovation for Public Welfare
- —Dalian Medical Key Specialties “Summit Project”
- —https://doi.org/10.13039/501100019033Key Research and Development Program of Liaoning Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFibromyalgia and Chronic Fatigue Syndrome Research · Stress Responses and Cortisol · Winter Sports Injuries and Performance
Introduction
Visual snow syndrome (VSS) is a chronic neurological disorder characterized by persistent visual disturbances resembling television static, accompanied by palinopsia, photophobia, and enhanced entoptic phenomena^1^. With a lifetime prevalence of 2.2%^2^, VSS represents a significant public health burden. Cross-sectional studies report that VSS patients exhibit significantly elevated rates of depression (25% reporting severe symptoms), anxiety, depersonalization, and sleep disturbances compared to healthy populations^3,4^.Although direct investigations of suicidal ideation in VSS remain limited, both visual impairment and chronic neurological conditions independently elevate suicide risk^5,6^. However, the psychological mechanisms linking visual symptoms to mental health deterioration remain poorly characterized, limiting the development of targeted interventions.
Previous research examining psychological mediators in VSS has been limited to direct pathways between visual symptoms and depressive outcomes^7,8^, failing to identify modifiable intervention targets that could guide clinical practice. Self-efficacy—defined as an individual’s belief in their capacity to execute behaviors necessary to produce specific performance outcomes^9^—has demonstrated robust associations with mental health outcomes across diverse chronic disease populations^10,11^. Critically, self-efficacy operates through its influence on QOL, defined by the World Health Organization as an individual’s perception of their position in life encompassing physical, psychological, social, and environmental well-being^12,13^. Theoretical frameworks postulate that self-efficacy enhances adaptive coping strategies, thereby improving QOL, which subsequently buffers against psychological distress^14,15^. Empirical evidence from chronic disease research supports this sequential pathway: self-efficacy predicts QOL improvements, which in turn reduce depressive symptoms and suicidal risk^16–18^ .
This serial model (VSS → self-efficacy → QOL → mental health outcomes) is theoretically more appropriate than alternative configurations because: (1) VSS diagnosis represents a stable clinical characteristic temporally preceding adaptive psychological processes, (2) self-efficacy as a belief system logically precedes its functional consequences on daily well-being (QOL), and (3) QOL impairments serve as proximal risk factors for subsequent mental health deterioration, as supported by intervention studies showing that enhancing self-efficacy improves QOL and thereby reduces psychological distress^19–21^.
Addressing these critical gaps in the VSS literature, the present study employed serial mediation analysis to examine whether self-efficacy and QOL sequentially mediate the relationship between VSS diagnosis and mental health outcomes of depression and suicidal ideation. We hypothesized that: (H1) VSS patients would exhibit significantly lower self-efficacy and QOL compared to healthy controls; (H2) VSS diagnosis would be associated with elevated depression and suicidal ideation; and (H3) the association between VSS and mental health outcomes would be serially mediated by reduced self-efficacy followed by impaired QOL. Confirmation of this theoretically grounded pathway would identify specific, modifiable intervention targets to mitigate mental health burden in this vulnerable population.
Method
Participants and procedures
Data collection occurred between December 2024 and January 2025. One hundred thirty-one participants were enrolled in this study, including 64 patients diagnosed with VSS (male: 51.6%, M = 29.39, SD = 6.52) and 67 healthy controls (male: 47.8%, M = 30.12, SD = 6.23). With the assistance of experienced therapists, 64 VSS patients from across China were recruited via a nation-wide patient group and provided with electronic questionnaires via the Questionnaire Star platform through QR codes. Participants in the healthy control group were recruited both online and via in-person word-of-mouth referrals, with the identical electronic questionnaires mentioned above.
Inclusion criteria for the VSS group were: (a) meeting the full diagnostic criteria for VSS^1^, (b) ability to provide informed consent and complete the online questionnaires. Exclusion criteria included: (a) presence of significant cognitive impairment, (b) Coexisting severe ophthalmic diseases (e.g., glaucoma, retinal detachment) or neurological disorders (e.g., epilepsy, stroke). Key demographic variables, including age, sex, and education level, were matched for VSS and healthy control subjects., with no statistically significant differences (p > 0.05) between these two groups. Healthy participants were screened in the structured questionnaires to confirm the absence of ophthalmological / neurological / psychiatric disorders or regular medication use.
The study was conducted in strict adherence to ethical guidelines. All research procedures were reviewed and approved by the Ethics Committee of Central Hospital of Dalian University of Technology (Approval No: YN2025-234-01). Informed consent was obtained from all participants before data collection, with assurances of data anonymity and confidentiality.
Study variables
The General Self-Efficacy Scale (GSES; Schwarzer, 1995) is a 10-item self-report scale that assesses the self-efficacy displayed by individuals in dealing with various types of challenges. The Chinese version of this scale used in this study has been validated and widely used in Chinese populations^22^. The scale had excellent internal consistency (Cronbach’s α = 0.906) in our sample.
The World Health Organization Quality of Life Brief Version Scale (WHOQOL-BREF; WHO, 1998) is a self-report scale with 26 items designed to assess the quality of an individual’s existence in four domains: physical health, mental health, social relationships, and the environment. The questionnaire was scored via a percentage system in this study. The Chinese version of this scale used in this study has been validated and is widely used in Chinese populations^23^. The scale had excellent internal consistency (Cronbach’s α = 0.911) in our sample.
The Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977) is a self-reported scale with 20 items that measures the level of depressive symptoms in individuals. The Chinese version of the CES-D used in this study has been validated and widely used in Chinese populations^24^. The scale had excellent internal consistency (Cronbach’s α = 0.928) in our sample.
The Beck Suicide Ideation Scale (SSI; Beck, 1979) is a self-report scale used to assess suicidal ideation. The Chinese version of the SSI used in this study has been validated and widely used in Chinese populations^25^. The present study used the first 5 questions of the scale to assess suicidal ideation, which is supported by prior evidence for its validity in measuring suicidal ideation^26^. The scale exhibited acceptable internal consistency, as evidenced by a Cronbach’s alpha coefficient (Cronbach’s α = 0.744) in the current sample.
Statistical analysis
Descriptive statistics of sociodemographic characteristics (age, sex, education), self-efficacy, QOL, depression, and suicidal ideation scores are reported as percentages (%), means ± standard deviations (SD), or medians (interquartile ranges [IQR]), according to variable features. Quantitative data following a normal distribution were compared using t-tests and expressed as means ± standard deviations. Non-normally distributed data were compared using non-parametric rank-sum tests and expressed as medians (IQR). Categorical variables are expressed as counts and percentages and were compared using chi-square tests.
To inspect the correlations between the variables of interest, estimates of Pearson’s bivariate correlations between VSS, self-efficacy, QOL, depression, and suicidal ideation were computed. Variance Inflation Factor (VIF) and Tolerance values were calculated, with VIF < 5 and Tolerance > 0.2 considered indicators of no severe multicollinearity, ensuring the reliability and stability of subsequent regression results.
To explore the pathway relationships between VSS, self-efficacy, QOL, and mental health outcomes (depression and suicidal ideation), multimodel linear regression analyses were conducted. Two adjusted regression models were established: Model 1 was adjusted for age and sex, while Model 2 further incorporated education as a covariate. The analysis focused on quantifying specific path coefficients, including VSS to self-efficacy (Path a1), VSS to QOL (Path a2), self-efficacy to QOL (Path d), VSS to depression (Path c), self-efficacy to depression (Path b1), QOL to depression (Path b2), VSS to suicidal ideation (Path f), self-efficacy to suicidal ideation (Path e1), and QOL to suicidal ideation (Path e2).
Serial mediation models were constructed to examine the mediating roles of self-efficacy and QOL in the association between VSS and mental health outcomes. Mediating effect analysis was performed via Model 6 in the Process 4.1 program compiled by Hayes, with the mediating effect tested by repeated sampling 5000 times through the bootstrap method. The models respectively focused on the mediating effects on the two mental health outcomes (depression and suicidal ideation), following the sequential path framework of VSS → self-efficacy → QOL → mental health outcomes. For each model, coefficients, standard errors, and t-values were calculated for each path to verify significance, and model fit indices (R², F-statistics) were reported to evaluate the validity of the mediation effects. All data analyses were performed using SPSS 23.0, with mediation analysis conducted via the Hayes PROCESS 4.1 macro^27^, and a two-sided p < 0.05 was considered statistically significant.
Results
Baseline characteristics of participants
Table 1 presents the baseline characteristics of participants. The VSS group (n = 64) and healthy control group (n = 67) were well-matched on age (VSS: 29 ± 7 years; Controls: 30 ± 6 years; p = 0.515), sex distribution (VSS: 51.6% male; Controls: 47.8% male; p = 0.664), and education level (p = 0.530).
Table 1. Baseline characteristics of participants in the VSS and healthy Controls.CharacteristicControls (n = 67)VSS (n = 64)p-valueAge, Mean ± SD30 ± 629 ± 70.515Sex, n (%)0.664Male32 (47.8%)33 (51.6%)Female35 (52.2%)31 (48.4%)Education, n (%)0.530High School or below8 (11.9%)9 (14.1%)Associate Degree18 (26.9%)21 (32.8%)Bachelor’s Degree32 (47.8%)30 (46.9%)Master’s Degree or above9 (13.4%)4 (6.3%)Self-efficacy30.6 ± 6.023.6 ± 6.2< 0.001QOL73.6 ± 8.862.5 ± 9.5< 0.001Depression11(7, 15)28(21, 34)< 0.001Suicidal ideation5(5, 6)6(5, 7)< 0.01Continuous variables are presented as mean ± standard deviation (SD) and were compared using independent t-tests. Categorical variables are presented as n (%) and were compared using Chi-square tests. This figure shows the baseline demographic and clinical characteristics of participants in the VSS group and the Healthy Controls group. Significant differences were found in Self-efficacy, QOL, Depression, and Suicidal ideation between the two groups. VSS = Visual Snow Syndrome; QOL = Quality of Life.VSS = Visual Snow Syndrome. QOL = Quality of Life.
Compared to healthy controls, VSS patients demonstrated significantly lower self-efficacy (VSS: 23.6 ± 6.2; Controls: 30.6 ± 6.0; p < 0.001) and QOL (VSS: 62.5 ± 9.5; Controls: 73.6 ± 8.8; p < 0.001). VSS patients also reported significantly higher levels of depression (median [IQR]: VSS: 28 [21, 34]; Controls: 11 [7, 15]; p < .001) and suicidal ideation (VSS: 6 [5, 7]; Controls: 5 [5, 6];* p* < 0.01). The median depression score of 28 in the VSS group substantially exceeds the CES-D clinical cutoff of ≥16 [28]—validated in Chinese populations [29,30]—indicating moderate-to-severe depressive symptomatology, while the median score of 11 in healthy controls falls below this threshold, reflecting no clinically significant depression. While the difference in suicidal ideation reached statistical significance, the absolute median difference of 1 point was small, suggesting modest clinical impact.
Correlational analyses
Table 2 presents the Pearson correlation coefficients among VSS, self-efficacy, QOL, depression, and suicidal ideation. VSS was significantly negatively correlated with self-efficacy (r = -0.502, p < 0.001) and QOL (r = -0.522, p < 0.001), while positively correlated with depression (r = 0.675, p < 0.001) and suicidal ideation (r = 0.261, p < 0.01). Self-efficacy showed a strong positive correlation with QOL (r = 0.636, p < 0.001) and inverse correlations with depression (r = -0.690, p < 0.001) and suicidal ideation (r = -0.313, p < 0.01). Additionally, QOL was significantly negatively associated with depression (r = -0.719, p < 0.001) and suicidal ideation (r = -0.512, p < 0.01), whereas depression and suicidal ideation exhibited a positive correlation (r = 0.419, p < 0.001). All correlations were statistically significant at the two-sided p < 0.05 level, confirming robust linear associations among the variables.
Table 2. Pearson correlations among VSS, Self-Efficacy, QOL, Depression, and suicidal Ideation.VariablesVSSSelf-efficacyQOLDepressionSuicidal ideationVSS1Self-efficacy-0.5021QOL-0.5220.6361Depression0.675-0.690***-0.7191Suicidal ideation0.261-0.313**-0.5120.419*1Correlations were calculated using bivariate Pearson correlation analysis. This figure presents the Pearson correlation analysis used to assess the relationships between VSS, Self-efficacy, QOL, Depression, and Suicidal ideation. The correlations were computed to examine both direct and indirect associations among these variables. Statistical significance for all correlations was determined using a p-value threshold of 0.001 for highly significant correlations, with the results presented in the table showing the strength and direction of these relationships. VSS = Visual Snow Syndrome; QOL = quality of life. Values represent Pearson correlation coefficients. Significance levels: *p < 0.05, **p < 0.01, ***p < 0.001.
Multimodel linear regression analysis
Collinearity diagnosis indicated that the VIF for all predictor variables was < 5 and Tolerance > 0.2, confirming no severe multicollinearity. Table 3 presents the results of multimodel linear regression analyses examining the pathway relationships among VSS, self-efficacy, QOL, depression, and suicidal ideation. The Model 1 (age- and sex-adjusted) and Model 2 (adjusted for age, sex, and education) showed a similar pattern of associations across all pathways. Both models confirmed that VSS significantly negatively predicted self-efficacy (Path a1: B = -7.09, p < 0.001) and QOL (Path a2: B = -11.15, p < 0.001), while self-efficacy positively predicted QOL (Path d: B = 0.94, p < 0.001). Notably, VSS consistently retained a direct positive predictive effect on depression (Path c: B = 16.01 p < 0.001) and suicidal ideation (Path f: B = 0.75, p < 0.01) across both adjusted models. Additionally, self-efficacy negatively predicted depression (Path b1: B = -1.16, p < 0.001) and suicidal ideation (Path e2: B = -0.07, p < 0.01). QOL negatively predicted both depression (Path b2: B = -0.81, p < 0.001) and suicidal ideation (Path e2: B = -0.07, p < 0.01).
Table 3. Multimodel linear regression analysis: relationships between VSS, Self-Efficacy, QOL, and mental health outcomes (Depression/Suicidal Ideation).PathModel 1Model 2B (95% CI)p-valueB (95% CI)p-valuea₁-7.05(-9.15~-4.94)< 0.001-7.09(-9.17~-5.01)< 0.001a₂-11.20(-14.35~-8.06)< 0.001-11.15(-14.24~-8.06)< 0.001D0.97(0.77 ~ 1.18)< 0.0010.94(0.74 ~ 1.15)< 0.001Depressionb₁-1.15(-1.35~-0.94)< 0.001-1.16(-1.38 ~-0.95)< 0.001b₂-0.79(-0.92 -0.66)< 0.001-0.81(-0.95-0.68)< 0.001C15.94(13.00 ~ 18.87)< 0.00116.01(13.04 ~ 18.97)< 0.001Suicidal ideatione₁-0.07 (-0.10 ~ -0.03)< 0.001-0.06 (-0.10 ~ -0.03)0.001e₂-0.07 (-0.10 ~ -0.05)< 0.001-0.07 (-0.09 ~ -0.05)< 0.001f0.79 (0.27 ~ 1.30)0.0030.75 (0.25 ~ 1.26)0.004Model 1: Age and sex adjusted; Model 2: Adjusted for age, sex and education; Path a1 = VSS → Self-efficacy; Path a2 = VSS → QOL; Path d = Self-efficacy → QOL; Path c = VSS → Depression; Path b1 = Self-efficacy → Depression; Path b2 = QOL → Depression; Path f = VSS → Suicidal ideation; Path e1 = Self-efficacy → Suicidal ideation; Path e2 = QOL → Suicidal ideation. This figure presents the linear regression analysis of the associations between VSS, Self-efficacy, QOL, and mental health outcomes (Depression and Suicidal Ideation). Two models were used: Model 1 adjusted for age and sex, and Model 2 adjusted for age, sex, and education. The analysis estimates the direct and indirect effects of each path, including the impact of VSS on Self-efficacy, QOL, Depression, and Suicidal Ideation, as well as the mediating effects of Self-efficacy and QOL. P-values indicate statistical significance for each path.VSS = Visual Snow Syndrome; QOL = quality of life.
Exploratory serial mediation analyses
Serial model of depression
The serial mediation model (VSS → self-efficacy → QOL → depression) was tested to explore the tenability of this specific theoretical pathway. The model results are presented in Table 4; Fig. 1. The model shows that the group significantly negatively affects self-efficacy, while both group and self-efficacy significantly impact QOL. Furthermore, group, self-efficacy, and QOL all significantly influence depression. Depression is indirectly affected by VSS through both self-efficacy and QOL.
Table 4. Relationships between quality of life-mediated self-efficacy and depression.AntecedentSelf-efficacyQOLDepressionCoeff.SE t p-valueCoeff.SE t p-valueCoeff.SE t p-valueVSS-7.0341.067-6.591< 0.001-5.7521.597-3.603< 0.0018.0201.4035.715< 0.001Self-efficacy----0.7580.1146.651< 0.001− 0.4880.111-4.404< 0.001QOL--------− 0.3890.074-5.248< 0.001Constant37.6461.67622.464< 0.00156.1744.80611.690< 0.00146.9245.7888.108< 0.001R^2^ = 0.252R^2^ = 0.459R^2^ = 0.688F = 43.436, p < 0.001F = 54.316, p < 0.001F = 93.405, p < 0.001This figure presents the results of regression analysis to examine the relationships between QOL-mediated self-efficacy and Depression. The analysis involved multiple models: Self-efficacy and QOL as mediators in the relationship between group and Depression. The regression models also include the adjusted R² values and F statistics, with p-values indicating the statistical significance of each path. Coefficients (Coeff.) and standard errors (SE) are presented for each path. VSS = visual snow syndrome; QOL = quality of life; The mediating effect accounted for 49.9% of the total effect (Total effect = 15.754, Mediating effect = 7.734, Indirect/Total = 49.9%).
Fig. 1. Serial mediation of self-efficacy and quality of life in the effect of Group on Depression. This figure presents the serial mediation model showing the effects of Group on Depression through Self-efficacy and QOL. The standardized regression coefficients (B) are shown for each path. Significant paths are marked with *** (p < 0.001), indicating strong relationships between the variables. *p < 0.05, **p < 0.01, ***p < 0.001.
Percentile bootstrap analyses demonstrated significant effects in the serial mediation model. The total effect of VSS on depression was significant, with a point estimate of 15.754 (SE = 1.516, 95% CI [12.754, 18.754]). This total effect decomposes into a significant direct effect of VSS on depression (Effect = 8.020, SE = 1.403, 95% CI [5.243, 10.797]) and a significant total indirect effect (Effect = 7.734, SE = 1.058, 95% CI [5.638, 9.854]). The total indirect effect was further partitioned into three specific pathways: the indirect effect via self-efficacy alone (VSS → Self-efficacy → Depression) was 3.433, calculated as indirect effect 1 = − 7.034×(− 0.488); the indirect effect via QOL alone (VSS → QOL → Depression) was 2.238, calculated as indirect effect 2 = − 5.752×(− 0.389); and the indirect effect through the sequential pathway (VSS → Self-efficacy → QOL → Depression) was 2.063, calculated as indirect effect 3 = − 7.034 × 0.758×(− 0.389). The proportion of the total effect mediated by these pathways was (7.734/15.754) ×100% ≈ 49.09%, indicating that nearly half of the total effect of VSS on depression was explained by the serial mediation through self-efficacy and QOL.
Serial model of suicidal ideation
A key finding was the significant indirect association of VSS with suicidal ideation through self-efficacy and QOL, in the absence of a significant direct effect (see Table 5; Fig. 2). Percentile bootstrap analyses revealed a significant total effect (Effect = 0.794, SE = 0.258, 95% CI = 0.283 to 1.304), a nonsignificant direct effect (Effect = − 0.010, SE = 0.281, 95% CI = − 0.565 to 0.546), and a significant indirect effect (Effect = 0.803, SE = 0.211, 95% CI = 0.385 to 1.224). Notably, none of the 95% confidence intervals included zero, strongly supporting the significance of the mediating effect. Methodologically, a significant indirect effect does not require a significant total direct effect, and such a pattern can indicate that the influence of the independent variable is fully accounted for by the mediating mechanism. This result underscores the potential importance of the self-efficacy-QOL pathway in understanding suicidal ideation in VSS, even in the absence of a strong direct link between the diagnosis and ideation.
Table 5. Relationships between quality of life-mediated self-efficacy and suicidal ideation.AntecedentSelf-efficacyQOLSuicidal ideationCoeff.SE t p-valueCoeff.SE t p-valueCoeff.SE t p-valueVSS-7.0341.067-6.591< 0.001-5.7521.597-3.603< 0.001− 0.0100.281− 0.0340.973Self-efficacy----0.7580.1146.651< 0.0010.0050.0220.2030.840QOL--------− 0.0750.015-5.085< 0.001Constant37.6461.67622.464< 0.00156.1744.80611.690< 0.00111.0151.1589.510< 0.001R^2^ = 0.252R^2^ = 0.459R^2^ = 0.688F = 43.436, p < 0.001F = 54.316, p < 0.001F = 93.405, p < 0.001This figure presents the hierarchical regression analysis of the effects of Group, Self-efficacy, and Quality of Life (QOL) on Suicidal ideation. Three variables, Self-efficacy, QOL, and Group, are tested in relation to Suicidal ideation in the regression model. The t-values and p-values indicate the statistical significance of each path, with p < 0.001 showing strong relationships.VSS = visual snow syndrome; QOL = quality of life. Coefficients (Coeff.) and standard errors (SE) are presented for each path.
Fig. 2. Serial mediation of self-efficacy and quality of life in the effect of Group on suicidal Ideation. This figure presents a serial mediation model illustrating the effects of Group on Suicidal Ideation through Self-efficacy and QOL. The unstandardized regression coefficients (B) are presented for each path. Significant paths are marked with *** (p < 0.001), indicating strong relationships between the variables. *p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
This study revealed that VSS patients exhibited widespread significantly lower self-efficacy and QOL scores, along with higher levels of depressive symptoms and suicidal ideation compared with healthy controls at baseline: significantly lower self-efficacy and QOL scores, coupled with elevated levels of depressive symptoms and suicidal ideation (p < 0.01). Serial mediation analysis further elucidated the pathways among variables. The effect of VSS on depression demonstrated partial mediation, operating through both a significant direct effect (p < 0.01) and an indirect pathway via the sequential chain of “diminished self-efficacy → compromised QOL.” In contrast, VSS showed no significant direct effect on suicidal ideation (p = 0.973), with the relationship being fully mediated through the same sequential pathway. The novelty of this study lies in documenting the elevated prevalence of suicidal ideation among VSS patients—a finding not systematically reported in prior VSS literature. Moreover, this represents the first demonstration that self-efficacy and QOL mediate the relationship between VSS and mental health outcomes, independent of age, sex, and educational attainment. While research in other disease populations has revealed similar mechanisms whereby reductions in self-efficacy and QOL influence mental health through complex psychological processes, such pathways have not been systematically characterized in VSS populations.
Our findings corroborate and extend existing literature on mental health outcomes in VSS. Consistent with prior reports^7,8^, we observed significantly elevated depression levels and diminished QOL among VSS patients compared with healthy controls. These patterns mirror those documented across diverse chronic disease populations, where QOL impairment has been consistently identified as a robust predictor of psychological distress^30–33^. Similarly, accumulating evidence indicates that compromised self-efficacy confers heightened vulnerability to depressive symptoms and suicidal ideation^9,27,34–36^ though the specific pathways linking these constructs in VSS have remained unexplored.
The differential mediation patterns for depression versus suicidal ideation provide important insights into the mechanisms linking VSS to mental health outcomes. For depression, the significant direct effect alongside the mediation pathway suggests VSS operates through dual mechanisms: (1) abnormal thalamocortical connectivity and hyperexcitability in visual processing regions reported in neuroimaging studies^2,37,38^—which may directly contribute to mood dysregulation, and (2) indirect psychological pathways through impaired self-efficacy and QOL reflecting the cumulative burden of chronic visual disturbances on daily functioning^39^. This dual-pathway model aligns with research on other chronic conditions showing that depression can arise both from disease-specific neurobiological processes and from psychosocial consequences of chronic illness^40^. In contrast, the complete mediation pattern observed for suicidal ideation—where the direct effect was not significant—suggests that VSS influences suicidal ideation primarily through its downstream effects on self-efficacy and QOL rather than through direct disease-specific mechanisms. This finding is consistent with theoretical models positing that suicidal ideation typically develops through accumulation of psychosocial risk factors, particularly impaired QOL and loss of functional capacity, rather than being a direct consequence of specific disease pathology^41,42^. The literature on suicide risk in chronic illness supports this interpretation, demonstrating that suicidal ideation is more strongly predicted by psychosocial factors such as quality of life, social isolation, and hopelessness than by disease severity or specific symptoms^43,44^. In VSS populations, the loss of self-efficacy resulting from uncontrollable symptoms may progressively erode QOL, and this deteriorated QOL—manifesting as impaired physical functioning, psychological distress, compromised social relationships, and environmental limitations—creates the proximal risk conditions for suicidal ideation^45^. This conceptual framework has important clinical implications, suggesting that interventions targeting self-efficacy and QOL may be effective in preventing suicidal ideation in VSS patients, even if the underlying visual symptoms cannot be fully resolved^14^.
Several limitations should be noted. First, the cross-sectional design precludes causal inference regarding the directionality of relationships among variables. Second, while the sample size (N = 131) is adequate for rare disease research, it remains modest for complex mediation analyses. Third, the Chinese sample may limit generalizability to other cultural contexts. Fourth, self-report measures may introduce response bias. Fifth, the study does not account for the severity of VSS symptoms. Sixth, we did not assess other factors that may influence the relationship between VSS and mental health, such as employment status, income level, social support, and symptom severity. Seventh, potential selection bias should be considered. VSS participants were recruited primarily through a patient support group, which may have resulted in a sample of individuals who are more actively seeking information or are more distressed by their symptoms compared to the broader VSS population. This might lead to an overestimation of the prevalence and severity of psychological distress in our findings. Therefore, caution is warranted when generalizing these results to all individuals with VSS. Nevertheless, this recruitment strategy was necessary and efficient for accessing a rare disease population for this exploratory study. Despite these limitations, this study provides evidence for the roles of self-efficacy and QOL in VSS-related mental health outcomes. Future longitudinal studies are needed to establish temporal relationships, and randomized controlled trials might evaluate interventions targeting self-efficacy and QOL to improve mental health outcomes in VSS patients.
Conclusions
This study provides novel evidence that VSS patients exhibit elevated depression and suicidal ideation alongside deficits in self-efficacy and QOL. Serial mediation analysis revealed that self-efficacy and QOL sequentially mediate the relationship between VSS and mental health outcomes. While the cross-sectional design precludes causal interpretation, these findings suggest that interventions targeting self-efficacy and QOL may help improve mental health outcomes in VSS patients. Future longitudinal research is needed to examine the temporal relationships and evaluate targeted interventions for this underserved population.
The reference list from the paper itself. Each links out to its DOI / PubMed record.