Sustained Complete Response to Brigatinib in a Young Patient With ALK‐Positive NSCLC Harboring I1171N Mutation Post‐Alectinib Resistance
Akhil Kapoor, Ajay Kumar Singh, Mahesh Chaudhary, Anuj Gupta, Bipinesh Sansar, Bal Krishna Mishra, Shashikant Patne, Arvind Suresh

TL;DR
A young patient with ALK-positive lung cancer achieved long-term remission with brigatinib after developing resistance to alectinib.
Contribution
Demonstrates brigatinib's effectiveness against I1171N mutation in ALK-positive NSCLC after alectinib resistance.
Findings
Brigatinib induced a complete and sustained response in a patient with I1171N-mediated alectinib resistance.
Durable intracranial disease control was observed with brigatinib treatment.
Repeat molecular testing was critical in identifying the resistance mutation and guiding treatment.
Abstract
ALK‐rearranged non–small cell lung cancer (NSCLC) represents a paradigm of precision oncology, but acquired resistance to second‐generation ALK tyrosine kinase inhibitors (TKIs) such as alectinib remains inevitable. We report a young, nonsmoker male with ALK‐positive metastatic NSCLC who achieved a sustained complete response (CR) to brigatinib following alectinib resistance mediated by the ALK I1171N mutation. After 22 months of response to alectinib, disease progression prompted repeat molecular profiling, which identified the I1171N alteration. Brigatinib was initiated, and a complete radiologic response was documented within 3 months and has been sustained for over 12 months, including durable intracranial disease control. Sustained CR in I1171N‐mediated alectinib resistance is rare and highlights the critical role of repeat molecular testing to guide ALK TKI sequencing.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
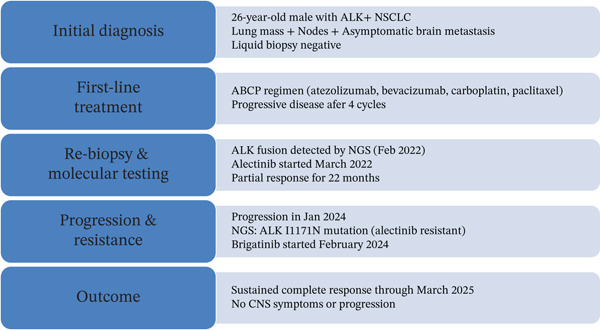 Figure 1
Figure 1 Figure 2
Figure 2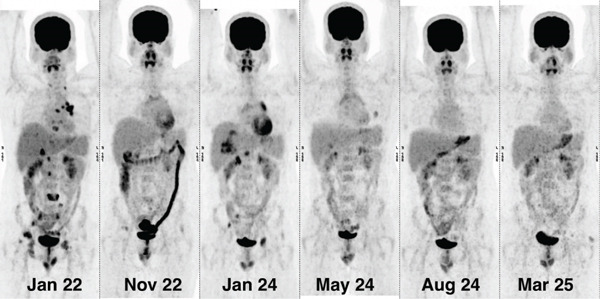 Figure 3
Figure 3| Mutation | Crizotinib | Ceritinib | Ensartinib | Alectinib | Brigatinib | Lorlatinib |
|---|---|---|---|---|---|---|
| I1171N/T/S | × | ± | ± | × | ✓ | ✓ |
| C1156Y | × | ± | ± | × | ✓ | ✓ |
| L1196M | × | ✓ | ✓ | × | ✓ | ✓ |
| V1180L | × | × | ± | × | ± | ✓ |
| G1202R | × | × | × | × | ± | ✓ |
| F1174C/V | × | ✓ | ✓ | ✓ | ✓ | ✓ |
| G1269A | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| S1206Y | × | ± | ± | × | ✓ | ✓ |
| D1203N | × | ± | ± | ± | ✓ | ✓ |
| Compound mutations | × | ± | ± | ± | ✓ | ± |
| Compound mutation | Crizotinib | Alectinib | Ceritinib | Brigatinib | Lorlatinib |
|---|---|---|---|---|---|
| G1202R + L1198F | ✓ | × | × | × | × |
| I1171N + L1198F | ✓ | × | × | ✓ | × |
| I1171N + L1256F | × | ✓ | × | ✓ | × |
| I1171N + L1196M | × | × | ✓ | ✓ | × |
| I1171N + G1269A | × | × | ✓ | ✓ | × |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Research Studies · Lung Cancer Diagnosis and Treatment
1. Introduction
Non–small cell lung cancer (NSCLC) remains the leading cause of cancer‐related mortality globally [1]. ALK‐rearranged NSCLC represents a distinct molecular subset typically affecting younger, nonsmoking individuals with adenocarcinoma histology [2]. The introduction of ALK TKIs has transformed outcomes, with progressively potent agents available across treatment lines.
Alectinib remains widely used as first‐line therapy; however, acquired resistance inevitably emerges. While lorlatinib—now preferred in contemporary guidelines—offers broad coverage against diverse ALK resistance mutations, its neurocognitive and metabolic toxicities may limit real‐world use [3–5]. Consequently, many patients initially treated with alectinib still require molecularly informed sequencing upon progression.
The ALK I1171N mutation is a clinically significant secondary resistance alteration, arising in the αC‐helix of the kinase domain. It confers resistance to alectinib but retains sensitivity to brigatinib and lorlatinib. Identifying this mutation at progression is therefore essential to optimize treatment selection.
2. Case Presentation
A 26‐year‐old nonsmoker male presented in late 2021 with cough and chest discomfort. Imaging demonstrated a left lung mass, mediastinal lymphadenopathy, and a single subcentimeter asymptomatic cerebral metastasis. Given the lesion size and risk of radionecrosis, upfront radiotherapy was deferred.
3. Baseline Molecular Testing
A plasma‐based liquid biopsy assessing EGFR, ALK, ROS1, and other alterations was negative. The patient received four cycles of ABCP (atezolizumab, bevacizumab, carboplatin, and paclitaxel), but follow‐up imaging showed progressive pulmonary disease.
4. Tissue NGS Assessment
A tissue rebiopsy followed by next‐generation sequencing (Illumina platform, mean target coverage > 350×; hybrid capture panel covering major oncogenic drivers) revealed an EML4–ALK fusion (Variant 3). The negative liquid biopsy was attributed to low tumor DNA shedding, a recognized limitation of plasma assays.
5. First‐Line Targeted Therapy
Alectinib was initiated in March 2022. Figure 1 summarizes the case timeline, molecular evolution, and treatment transitions. A partial radiologic response occurred within 3 months, with a 42% reduction in target lesion size (Figure 2). Disease control was maintained for 22 months, as evidenced by serial scans (Figure 3).
Figure summarizing the case timeline, molecular evolution, and treatment transitions.
Response of PET‐CT scan of the patient showing comparison of (a) January 2024 scan images with (b) May 2024 scans. To note, brigatinib was started in February 2024 after the patient had progressive disease in the liver, nodes, and bones on alectinib.
Serial scout images of FDG PET‐CT showing progressive liver, nodes, and bony lesions on January 24, which responded completely in the scan of May 24 after starting brigatinib, and the response was maintained in scans of August 24 and March 25.
6. Progression and Repeat Molecular Testing
In January 2024, imaging revealed progressive liver, nodal, and osseous lesions, while the brain remained stable. Repeat NGS (same platform and coverage) demonstrated the persistence of ALK fusion along with a newly acquired ALK I1171N mutation (VAF 24%). Brain MRI confirmed no intracranial progression. SRS/WBRT was not indicated.
7. Brigatinib Therapy and Treatment Response
Brigatinib was initiated in February 2024 (90 mg lead‐in ×7 days → 180 mg daily). Treatment was well tolerated, with only Grade 1 CPK elevation.
Follow‐up PET‐CT at 12 weeks showed a complete metabolic response with an approximately 90% reduction in overall tumor size, including near‐complete resolution of hepatic, nodal, and osseous lesions. Serial imaging in August 2024 and March 2025 confirmed a sustained complete response, with persistent metabolic inactivity and stable intracranial disease.
8. Discussion
ALK‐rearranged NSCLC exemplifies the success of precision oncology, with multiple generations of ALK TKIs offering sequential lines of targeted therapy. However, despite impressive responses to first‐line alectinib, most patients eventually develop acquired resistance. Resistance to alectinib is heterogeneous, arising from both ALK‐dependent and ALK‐independent mechanisms. Secondary ALK kinase domain mutations account for 30%–40% of cases and include alterations such as I1171N/T/S, V1180L, and G1202R [6]. The I1171N substitution in the αC‐helix alters the kinase conformation, reducing alectinib binding affinity. Importantly, preclinical and clinical data show preserved sensitivity to brigatinib and lorlatinib.
Brigatinib′s distinct structural and biochemical properties enable it to overcome resistance conferred by mutations such as I1171N, C1156Y, and L1196M. Additionally, brigatinib demonstrates robust central nervous system (CNS) penetration, a frequent site of disease progression in ALK‐positive NSCLC, making it a particularly effective option following alectinib failure [5, 7, 8]. The third‐generation ALK inhibitor, lorlatinib, offers the broadest coverage of ALK resistance mutations to date, including activity against the notoriously refractory G1202R mutation and several compound mutations [9]. However, its use may be constrained in certain patients by CNS‐related adverse effects, including cognitive and mood alterations, as well as dyslipidemia, which can limit its tolerability in real‐world settings. These considerations further elevate the need for precise molecular characterization at progression.
This case is noteworthy due to the patient′s young age and excellent long‐term responsiveness to sequential ALK‐targeted therapies. High‐quality tissue NGS confirmed I1171N‐mediated alectinib resistance, enabling a precise, mutation‐guided therapeutic shift. Following the initiation of brigatinib, the patient achieved a complete radiologic response within 3 months, which has been sustained for over 12 months, including continued intracranial disease stability. Durable complete responses in I1171N‐mediated alectinib resistance are rare, highlighting the unique clinical relevance of this case. However, it should be noted that this report lacks serial circulating tumor DNA (ctDNA) monitoring, prohibiting dynamic assessment of molecular evolution. Additionally, only single‐site tissue biopsies were analyzed, potentially underestimating tumor heterogeneity.
Table 1 summarizes the spectrum of resistance mutations in the ALK kinase domain and their differential sensitivity profiles. While lorlatinib retains efficacy against many single and compound mutations, recent data highlight that certain compound mutations involving I1171N or G1202R + L1196M may exhibit reduced sensitivity even to lorlatinib [10]. Intriguingly, earlier‐generation agents like brigatinib may retain activity in select lorlatinib‐resistant scenarios, particularly when compound mutations include I1171N. Table 2 details the mutation‐specific activity of brigatinib and lorlatinib, underscoring the complementary roles these agents play in sequential ALK inhibition.
Tailoring the sequence of ALK TKIs based on the molecular landscape at resistance is not only clinically rational but is increasingly supported by guideline recommendations and expert consensus. In our previously reported experience using a molecular tumor board approach, incorporation of repeat molecular testing—including tissue‐ or plasma‐based NGS—allowed for informed treatment selection and improved patient outcomes [9, 11].
Therefore, performing a repeat biopsy or ctDNA analysis at the time of disease progression is not merely a research endeavor—it is a clinical necessity. Without this, empiric sequencing of ALK TKIs may result in suboptimal outcomes, premature exposure to later‐line agents, and increased toxicity. Personalized therapy based on molecular resistance mechanisms represents the next frontier in maximizing outcomes in ALK‐positive NSCLC, and biopsy at progression is the gateway to that paradigm and may significantly improve outcomes when molecularly matched therapies are selected.
Author Contributions
A.K. conceptualized the manuscript, drafted the manuscript, and provided the oncologic care. A.K.S. obtained the necessary images, provided the oncologic care, and contributed to editing the manuscript. M.C., A.G., B.S., B.K.M., S.P., and A.S. contributed to editing. B.K.M., A.G., and B.S. contributed to providing clinical care to the patient.
Funding
No funding was received for this manuscript.
Disclosure
All the authors approved the final manuscript. The manuscript does not have any identifiers of the patient. No other sources were utilized for the writing of this manuscript.
Ethics Statement
Ethical approval was waived off by the institute since this is a case report of a patient treated as per the multidisciplinary tumor board.
Consent
The patient provided written informed consent for the publication of this case report.
Conflicts of Interest
The authors declare no conflicts of interest.
General Statement
Key Clinical Message. This case emphasizes the utility of rebiopsy and molecular testing at progression to guide next‐line ALK TKI sequencing, resulting in a sustained and clinically meaningful response.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gainor J. F. , Dardaei L. , Yoda S. , Friboulet L. , Leshchiner I. , Katayama R. , Dagogo-Jack I. , Gadgeel S. , Schultz K. , Singh M. , Chin E. , Parks M. , Lee D. , Di Cecca R. H. , Lockerman E. , Huynh T. , Logan J. , Ritterhouse L. L. , Le L. P. , Muniappan A. , and Shaw A. T. , Molecular Mechanisms of Resistance to First- and Second-Generation ALK Inhibitors in ALK-Rearranged Lung Cancer, Cancer Discovery. (2016) 6, no. 10, 1118–1133, 27432227, 10.1158 · doi ↗ · pubmed ↗
- 2Kapoor A. , Noronha V. , Patil V. , Menon N. , Joshi A. , Kumar A. , Singh A. K. , Mahajan A. , Janu A. , Kumar R. , Pai T. , Chougule A. , Shetty O. , and Prabhash K. , Clinical Profile, Practice Pattern, and Outcomes With First-Line Therapy in ALK-Positive Lung Cancer: Real-World Data From Resource-Constrained Settings, JTO Clinical and Research Reports. (2023) 4, no. 1, 100443, 10.1016/j.jtocrr.2022.100443, 36654881.36654881 PMC 9841022 · doi ↗ · pubmed ↗
- 3Shaw A. T. , Bauer T. M. , de Marinis F. , Felip E. , Goto Y. , Liu G. , Mazieres J. , Kim D. W. , Mok T. , Polli A. , Thurm H. , Calella A. M. , Peltz G. , Solomon B. J. , and CROWN Trial Investigators , First-Line Lorlatinib or Crizotinib in Advanced ALK-Positive Lung Cancer, New England Journal of Medicine. (2020) 383, no. 21, 2018–2029, 10.1056/NEJ Moa 2027187, 33207094.33207094 · doi ↗ · pubmed ↗
- 4Solomon B. J. , Liu G. , Felip E. , Mok T. S. K. , Soo R. A. , Mazieres J. , Shaw A. T. , de Marinis F. , Goto Y. , Wu Y. L. , Kim D. W. , Martini J. F. , Messina R. , Paolini J. , Polli A. , Thomaidou D. , Toffalorio F. , and Bauer T. M. , Lorlatinib Versus Crizotinib in Patients With Advanced ALK-Positive Non-Small Cell Lung Cancer: 5-Year Outcomes From the Phase III CROWN Study, Journal of Clinical Oncology : Official Journal of the American Society of Clinic · doi ↗ · pubmed ↗
- 5Lin J. J. , Zhu V. W. , Schoenfeld A. J. , Yeap B. Y. , Saxena A. , Ferris L. A. , Dagogo-Jack I. , Farago A. F. , Taber A. , Traynor A. , Menon S. , Gainor J. F. , Lennerz J. K. , Plodkowski A. J. , Digumarthy S. R. , Ou S. I. , Shaw A. T. , and Riely G. J. , Brigatinib in Patients With Alectinib-Refractory ALK-Positive NSCLC, Journal of Thoracic Oncology : Official Publication of the International Association for the Study of Lung Cancer. (2018) 13, no. 10, 15 · doi ↗ · pubmed ↗
- 6Remon J. , Pignataro D. , Novello S. , and Passiglia F. , Current Treatment and Future Challenges in ROS 1- and ALK-Rearranged Advanced Non-Small Cell Lung Cancer, Cancer Treatment Reviews. (2021) 95, 102178, 10.1016/j.ctrv.2021.102178, 33743408.33743408 · doi ↗ · pubmed ↗
- 7Kim H. J. , Lee E. A. , Park J. H. , and Lee H. W. , Real-World First-Line Outcomes of Alectinib and Brigatinib in Anaplastic Lymphoma Kinase-Positive Non-Small Cell Lung Cancer: A Nationwide South Korean Cohort Study Using the Health Insurance Review and Assessment Data, Translational Lung Cancer Research. (2025) 14, no. 11, 4811–4823, 10.21037/tlcr-2025-983, 41367570.41367570 PMC 12683494 · doi ↗ · pubmed ↗
- 8Sánchez-Herrero E. , Blanco Clemente M. , Calvo V. , Provencio M. , and Romero A. , Next-Generation Sequencing to Dynamically Detect Mechanisms of Resistance to ALK Inhibitors in ALK-Positive NSCLC Patients: A Case Report, Translational Lung Cancer Research. (2020) 9, no. 2, 366–372, 10.21037/tlcr.2020.02.07, 32420077.32420077 PMC 7225153 · doi ↗ · pubmed ↗