Birth weight, ototoxic medication, and surgical history predict individual hearing loss risks: a systematic review and meta-analysis
Hanwen Luo, Jianghua He, Dapeng Chen, Xiaoming Xu, Jing Zhao, Xiaoyan Yang, Jing Shi

TL;DR
This study identifies key risk factors for hearing loss in neonates admitted to the NICU, including very low birth weight and exposure to certain medications.
Contribution
The study provides a systematic review and meta-analysis of neonatal hearing loss risk factors in NICU settings.
Findings
Very low birth weight (<1,500 g) is significantly associated with hearing loss in NICU neonates.
Exposure to ototoxic drugs and surgical ligation of PDA are linked to increased hearing loss risk.
Low Apgar score, prematurity, and sepsis were not significantly correlated with hearing loss.
Abstract
Hearing loss (HL) impairs sound perception and includes sensorineural, conductive, and mixed subtypes. Compared with healthy newborns, infants admitted to the neonatal intensive care unit (NICU) are at substantially increased risk of congenital anomalies and exposure to HL-related risk factors. However, the specific determinants of neonatal HL remain controversial. This systematic review and meta-analysis seeks to identify risk factors linked to HL in neonates admitted to the NICU. PubMed, the Cochrane Library, Embase, and Web of Science were systematically searched from March 26, 1996, to February 25, 2025. Eligible studies were English-language retrospective studies employing multivariate logistic regression to evaluate potential risk factors for HL in NICU neonates. Meta-analyses were conducted using STATA, and pooled estimates were reported as odds ratios or relative risks (OR/RR)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
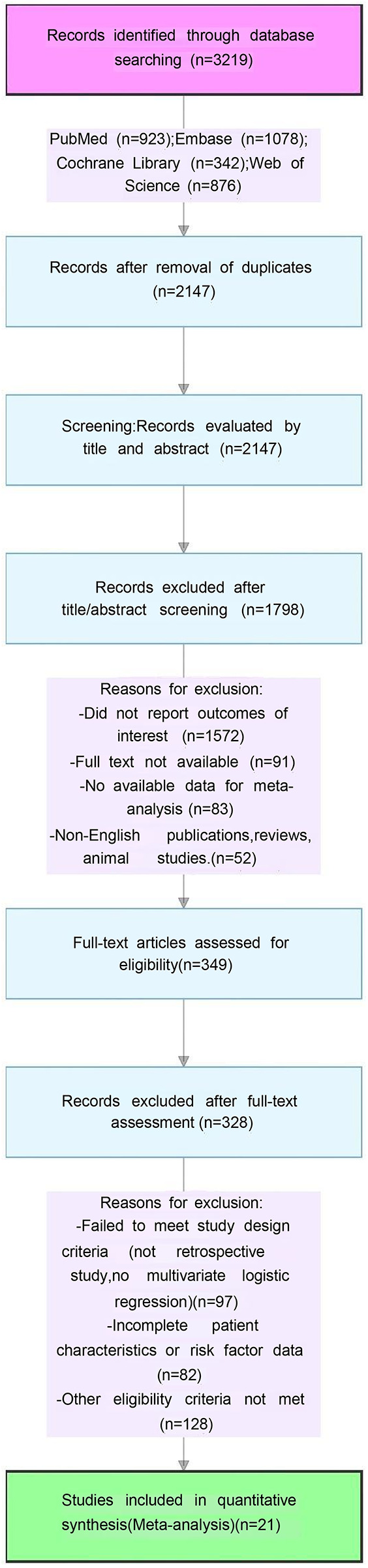 Figure 1
Figure 1| Firstauthor (year) | Newcastle-Ottawa scale | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Is the case definition adequate? | Representativeness of the cases | Selection of Controls | Definition of Controls | Comparability | Ascertainment of exposure | Same method of ascertainment for cases and controls | Non-response rate | Total score | |
| Smith et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Maharani etal. ( | ★ | ★ | ✩ | ✩ | ★★ | ★ | ★ | ✩ | 6 |
| Wang et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| Khairy et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Abdullah et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Hajare and Mudhol ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| Van Dommelen et al. ( | ★ | ★ | ✩ | ✩ | ★★ | ★ | ★ | ✩ | 6 |
| Lima et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| Bhat et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| Gupta et al. ( | ★ | ★ | ✩ | ✩ | ★★ | ★ | ★ | ✩ | 6 |
| Alaee et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| de Hoog et al. ( | ★ | ★ | ✩ | ✩ | ★★ | ★ | ★ | ✩ | 6 |
| Robertson et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Cooper et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Eras et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| Hille et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| Leslie et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Arslan et al. ( | ★ | ★ | ✩ | ✩ | ★★ | ★ | ★ | ✩ | 6 |
| Chant et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Wang et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ✩ | 7 |
| Nair et al. ( | ★ | ★ | ★ | ✩ | ★★ | ★ | ★ | ★ | 8 |
| First author | Year | Country | Study design | Sample size | Follow-up | Statistical Model | Gestational age | Birth weight | Risk factors |
|---|---|---|---|---|---|---|---|---|---|
| RichardJ. H.Smith | 1992 | America | retrospective study | 238 | 6-year period beginning in 1981 | Stepwise Logistic Regression | NS | NS | Family history |
| Craniofacial anomalies/Congenital head and neck deformity | |||||||||
| Low Apgar scores | |||||||||
| Hyperbilirubinemia | |||||||||
| Ototoxic medication | |||||||||
| Convulsions/Seizure disorder | |||||||||
| Ni Luh Putu Maharani | 2015 | Bali | retrospective study | 54 | From November 2012 to February 2013 | Multivariable logistic regression | NS | 2,732 ± 7.365 g | Hyperbilirubinemia |
| Ototoxic medication | |||||||||
| Meningitis | |||||||||
| Chien-Ho Wang | 2017 | China Taiwan | retrospective study | 309 | From January 2010 to 2011. | Logistic Regression Analysis | 27.5 ± 1.4 | 1,028 ± 180 g | Low birth weight |
| Craniofacial anomalies/Congenital head and neck deformity | |||||||||
| Ototoxic medication | |||||||||
| Intracranial hemorrhage/Intracranial complication | |||||||||
| Prematurity/Shorter gestational length | |||||||||
| PDA surgical ligation | |||||||||
| Oxygen duration | |||||||||
| May Ahmed Khairy | 2018 | Egypt | retrospective study | 260 | From May | Logistic regression | 32.7 weeks | 1,750 gm | Mechanical ventilation |
| From May 2013 to January 2014 | |||||||||
| Asma ABDULLAH | 2020 | Malaysia | retrospective study | 2,713 | From January 2014 to December 2016 | Logistic regression | NS | NS | Low birth weight |
| Craniofacial anomalies/Congenital head and neck deformity | |||||||||
| Mechanical ventilation | |||||||||
| Low Apgar scores | |||||||||
| Hyperbilirubinemia | |||||||||
| Ototoxic medication | |||||||||
| Priti Hajare | 2021 | India | retrospective study | 402 | N | Logistic regression | NS | NS | low birth weight |
| Family history | |||||||||
| Craniofacial anomalies/Congenital head and neck deformity | |||||||||
| Parental consanguinity | |||||||||
| Mechanical ventilation | |||||||||
| Hyperbilirubinemia | |||||||||
| Sex (male) | |||||||||
| Intracranial hemorrhage/Intracranial complication | |||||||||
| Prematurity/Shorter gestational length | |||||||||
| Torch infection | |||||||||
| van Dommelen | 2010 | Netherlands | retrospective study | 10,830 | For 2002–2005 | Multivariate logistic regression | NS | NS | Low birth weight |
| Craniofacial anomalies/Congenital head and neck deformity | |||||||||
| Mechanical ventilation | |||||||||
| Low Apgar scores | |||||||||
| Sex (male) | |||||||||
| Sepsis | |||||||||
| Phototherapy | |||||||||
| Torch infection | |||||||||
| Meningitis | |||||||||
| Chromosomal abnormalities/Positive genetic syndrome/Down syndrome | |||||||||
| Oxygen duration | |||||||||
| Gisele M.L.Lima | 2006 | Brasil | retrospective study | 979 | 2000.1–2003.1 | Multiple analyses by logistic regression | NS | NS | low birth weight |
| Family history | |||||||||
| Craniofacial anomalies/Congenital head and neck deformity | |||||||||
| Mechanical ventilation | |||||||||
| Hyperbilirubinemia | |||||||||
| Chromosomal abnormalities/Positive genetic syndrome/Down syndrome | |||||||||
| Postnatal hypoxia/severe birth asphyxia | |||||||||
| Jehangir Allam Bhat | 2018 | Indian | retrospective study | 195 | From June 2015 to May 2016 | Multivariate logistic regression | NS | NS | Family history |
| Low Apgar scores | |||||||||
| Hyperbilirubinemia | |||||||||
| Chromosomal abnormalities/Positive genetic syndrome/Down syndrome | |||||||||
| A.K. Gupta | 1991 | India | retrospective study | 24 | From March 1989 to July 1989 | Multiple Logistic regression analysis. | NS | NS | Low birth weight |
| Hyperbilirubinemia | |||||||||
| Prematurity/Shorter gestational length | |||||||||
| Ehsan Alaee | 2015 | Iran | retrospective study | 791 | 2010–2011 | Binary logistic regression | NS | NS | low birth weight |
| Hyperbilirubinemia | |||||||||
| aminoglycosides | |||||||||
| Vancomycin | |||||||||
| Vancomycin duration | |||||||||
| Prematurity/Shorter gestational length | |||||||||
| MATTHIJS DE HOOG | 2003 | Netherlands. | retrospective study | 625 | From November 1998 to November 2000 | Multiple logistic regression | NS | NS | aminoglycosides |
| Vancomycin | |||||||||
| Vancomycin duration | |||||||||
| Loop diuretics/Duration of diuretic use | |||||||||
| CHARLENE M. T. ROBERTSON | 2005 | Canada | retrospective study | 43 | Born January 1994 through | Multivariate forward stepwise logistic regression | NS | NS | aminoglycosides |
| Loop diuretics/Duration of diuretic use | |||||||||
| Aaron C. Cooper | 2011 | USA | retrospective study | 29 | Between February 2003 and January 2008 | Multivariate logistic regression | NS | NS | aminoglycosides |
| Zeynep Eras | 2014 | Turkey | retrospective study | 1,360 | Between September 2009 and December 2011 | Multinomial logistic regression analysis | 29.7 ± 2.3 weeks | 1,317 ± 349.7 g | Mechanical ventilation |
| PDA surgical ligation | |||||||||
| Loop diuretics/Duration of diuretic use | |||||||||
| Elyśee TM Hille | 2007 | Netherlands | retrospective study | 2,186 | Between October 1, 1998, and January 1, 2002 | Multivariate analysis | 28.5 ± 1.6 | 1,039 ± 256 | Mechanical ventilation |
| Postnatal hypoxia/severe birth asphyxia | |||||||||
| GI LESLIE | 1995 | Australia | retrospective study | 102 | From July 1985 through December 1990 | Logistic regression analysis | 26 ± 1.2 | 982 ± 123 | Oxygen duration |
| S. Arslan | 2013 | Turkey | retrospective study | 136 | Between May 2007 and January 2008 | Logistic regression analysis | NS | NS | Parental consanguinity |
| Prematurity/Shorter gestational length | |||||||||
| Kathy Chant | 2022 | UK | retrospective study | 36 | Between 2009 and 2013 | Multiple regressions | NS | NS | sex |
| Birth weight | |||||||||
| Low Apgar scores | |||||||||
| Laura A. Wang | 2018 | USA | retrospective study | 1,020 | Between 2004 and 2013 | Logistic regression model | NS | NS | Loop diuretics/Duration of diuretic use |
| Vrinda Nair | 2021 | England | retrospective study | 122 | 2005–2019 | Binary logistic regression | NS | NS | Craniofacial anomalies/Congenital head and neck deformity |
| Mechanical ventilation | |||||||||
| Hyperbilirubinemia | |||||||||
| aminoglycosides | |||||||||
| Vancomycin | |||||||||
| Sepsis | |||||||||
| Convulsions/Seizure disorder | |||||||||
| Meningitis | |||||||||
| Total | — | — | — | 21,143 | — | — | 28.0 ± 6.1 | 1,475 ± 274 g | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing, Cochlea, Tinnitus, Genetics · Ear Surgery and Otitis Media · Congenital Ear and Nasal Anomalies
Introduction
1
Hearing loss (HL), including sensorineural hearing loss (SNHL), conductive hearing loss (CHL), and mixed hearing loss (MHL), is a congenital or perinatal condition that can profoundly impair language acquisition, cognitive development, and social integration in neonates. Infants admitted to neonatal intensive care units (NICUs) are at substantially increased risk of hearing impairment due to exposure to multiple adverse medical conditions and intensive interventions. Epidemiological evidence indicates that the incidence of SNHL among NICU neonates ranges from 1% to 10%, which is approximately 30-fold higher than the 0.1% prevalence observed in the general newborn population (1, 2). Furthermore, previous studies have reported that 26.3% of affected NICU neonates present with SNHL, 30.4% with CHL, and 20% with MHL (1–3). SNHL in this population is commonly attributed to immature cochlear development and environmental stressors, whereas CHL is more often linked to congenital structural anomalies or acquired inflammatory conditions (4). These alarming statistics underscore the critical need to systematically identify and validate key HL risk factors in NICU neonates.
Otoacoustic emissions (OAE) and auditory brainstem response (ABR) are mainstream tools for neonatal HL screening (3, 5, 6): OAE assesses cochlear function with high sensitivity (7), while ABR evaluates central auditory pathway integrity and behavioral thresholds. Per JCIH recommendations, a two-stage screening protocol, initial OAE followed by ABR for infants who fail OAE, is widely implemented in NICUs and well-baby nurseries. OAE is preferred as a first-line screening tool for its simplicity, cost-effectiveness, and time efficiency (8). The OAE-ABR combination is regarded as the gold standard for NICU hearing screening, enabling the detection of auditory neuropathy spectrum disorders (9) and highlighting the necessity of early HL detection and intervention.
Over the past decades, the JCIH has proposed 10 major risk factors for neonatal HL, including very low birth weight (<1,500 g), exposure to ototoxic medications, and mechanical ventilation for more than five days [Joint Committee on Infant Hearing (JCIH), 1994 Position Statement] (10). However, subsequent studies have yielded inconsistent results regarding the predictive value of these factors. For example, Wang et al. (11)and Lima et al. (12) confirmed a significant association between low birth weight and SNHL, while Abdullah et al. (13) found no such correlation. Arslan et al. (14) identified ototoxic drug exposure as a strong predictor of HL, while Alaee et al. (15) and Hille et al. (16) reported contradictory findings. With respect to surgical history, ductus arteriosus ligation, a common NICU procedure, has been suggested to increase the risk of central nervous system-related hearing impairment in extremely preterm infants (5), but evidence remains limited, and large-scale validation is lacking.
Notably, several critical gaps persist in the existing literature. Most studies have analyzed NICU neonates together with community-born newborns, potentially obscuring NICU-specific risk profiles. Moreover, no meta-analysis to date has systematically evaluated the associations between core risk factors, like birth weight, ototoxic medication exposure, and surgical history, and HL specifically in NICU populations. Therefore, this systematic review and meta-analysis aim to synthesize evidence from retrospective studies using multivariate logistic regression to quantify the strength of associations between these risk factors and HL in NICU neonates. By providing robust pooled estimates, this study seeks to facilitate early identification of high-risk infants and inform targeted screening and preventive strategies.
Materials & methods
2
The findings of this paper were presented under the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (17) and the Cochrane Handbook for Systematic Reviews of Interventions (18). The study protocol was registered with PROSPERO (CRD420250653476).
Eligibility criteria
2.1
Study type
2.1.1
Retrospective studies published in English between March 26, 1996, and February 25, 2025, were eligible. Included studies were required to employ multivariate logistic regression analyses to investigate risk factors for HL in NICU neonates and to report effect estimates as odds ratios (ORs) or relative risks (RRs) with corresponding 95% confidence intervals (CIs).
Study subjects
2.1.2
Inclusion criteria were: (1) neonates admitted to the NICU within 28 days after birth; (2) HL diagnosed within 3 months after birth using OAE or ABR (defined as failure of OAE twice or ABR once); (3) patient characteristics and candidate risk factors, as detailed in Table 1, were reported; (4) multivariate logistic regression was performed with complete statistical results available.
Definition of exposure and control
2.1.3
Exclusion criteria were: (1) animal studies; (2) duplicate publications, studies with inaccessible data, or those unsuitable for meta-analysis; (3) reviews, expert commentaries, guidelines, or opinion articles; (4) incomplete full-text availability; (5) non-English publications.
The exposure group consisted of NICU neonates diagnosed with HL who were exposed to one or more target risk factors, including ototoxic medications, low birth weight, surgical history (surgical procedures may increase HL risk through combined effects of anesthetic neurotoxicity, perioperative cerebral hemodynamic alterations, and congenital organ malformations (19), sex (sex hormone regulation, genetic architecture differentiation, and cochlear structural-functional specialization account for variations in hearing impairment), and other potential factors.
The control group included NICU neonates without exposure to the specified risk factors and without a diagnosis of HL, with baseline characteristics comparable between groups.
Literature search strategy
2.2
PubMed, Cochrane Library, Embase, and Web of Science were retrieved from March 26, 1996, to February 25, 2025. Medical Subject Headings (MeSH) terms were combined with free-text keywords, and the detailed search strategy is provided in Supplementary File S1. Core search terms included “newborns,” “HL,” “NICU,” “ototoxic medication,” and “surgical history,” ensuring comprehensive identification of relevant studies.
Data extraction and quality assessment
2.3
Data extraction
2.3.1
Data were independently extracted by two investigators (Dapeng Chen and Jianghua He). Extracted information included study characteristics (first author, publication year, country, sample size, and follow-up duration), participant characteristics (gestational age and birth weight), types of risk factors, statistical models, and main outcomes (OR/RR, 95% CI, and P values). Discrepancies were resolved through discussion with a third reviewer (Jing Shi).
Risk of bias assessment
2.3.2
The risk of bias in the included studies was assessed via the Newcastle-Ottawa Scale (NOS), which evaluates eight domains: (1) adequacy of case definition; (2) representativeness of cases; (3) selection of controls; (4) definition of controls; (5) comparability between groups; (6) ascertainment of exposure; (7) consistency of exposure assessment between cases and controls; and (8) adequacy of the non-response rate. Assessments were conducted independently by two reviewers, with disagreements resolved by consensus. Quality assessment results are shown in Table 1.
To minimize subjectivity in quality appraisal, two additional measures were implemented. First, a standardized operational guideline for judgment was established to reduce inter-reviewer variability. Second, sensitivity analyses were performed to compare pooled estimates derived from high-quality studies with those from all included studies, thereby evaluating the robustness of the conclusions against potential bias.
Statistical analysis
2.4
STATA was used for data analysis, with pooled effect sizes presented as odds ratios (OR) or relative risk (RR) and 95% confidence interval (CI). Heterogeneity between studies was first assessed using the I^2^ statistic and P-value: if P < 0.05 and/or I^2^ > 50%, significant heterogeneity was indicated, and the DerSimonian-Laird random-effects model was used for data pooling [weight W_i_ = 1/(V_i_ + τ^2^), where V_i_ is the within-study variance and τ^2^ is the between-study variance estimated by the restricted maximum likelihood method]; otherwise, the fixed-effects model was adopted. Sensitivity analyses were conducted by sequentially omitting individual studies to assess the stability of pooled results. Publication bias was evaluated using funnel plots and Begg's test, and the trim-and-fill method was applied when bias was detected.
Outcome measures
2.5
1. P-value;2. OR/RR and 95% CI.
Results
3
3,219 records were identified from PubMed (n = 923), Embase (n = 1,078), the Cochrane Library (n = 342), and Web of Science (n = 876). After removal of duplicates, 2,147 records underwent title and abstract screening, of which 1,798 were excluded (1,572 for irrelevant outcomes, 91 for unavailable full text, 83 for insufficient data for meta-analysis, and 52 for non-English publications, reviews, or animal studies). The remaining 349 articles were assessed in full text, leading to the exclusion of 328 studies (97 for inappropriate study design, 82 for incomplete patient or risk factor data, and 128 for failure to meet other eligibility criteria). Ultimately, 21 observational studies were included in the meta-analysis (Figure 1). [Smith et al. (20); Maharani et al. (21); Wang et al. (11); Khairy et al. (9); Abdullah et al. (13); Hajare et al. (22); Dommelen et al. (23); Lima et al. (12); Bhat et al. (24); Gupta et al. (25); Alaee et al. (15); Hoog et al. (26); Robertson et al. (27); Cooper et al. (28); Eras et al. (29); Hille et al. (16); Leslie et al. (30); Arslan et al. (14); Chant et al. (31); Wang et al. (11); Nair et al. (32)] were included. Characteristics of these studies are listed in Table 2.
PRISMA flow diagram of the study process. PRISMA, preferred reporting items for systematic review and meta-analysis.
Quality assessment results are displayed in Supplementary Table S1.
Association between ototoxic medications and HL
3.1
Five studies examined the association between exposure to ototoxic medications and HL in neonates admitted to the NICU. Meta-analysis demonstrated a significant association between ototoxic medication exposure and increased HL risk (OR = 2.00, 95% CI: 1.52–2.63, I^2^ = 65.2%, P < 0.001) (Supplementary Figure S1).
Aminoglycosides: Data from four studies demonstrated a significant link to HL [OR = 1.95, 95% CI (1.35, 2.82), I^2^ = 74.8%, P < 0.01] (Supplementary Figure S13).
Loop diuretics: Two studies confirmed that loop diuretic use was related to an elevated risk of HL [OR = 3.26, 95% CI (2.04, 5.14), I^2^ = 50.0%, P = 0.00] (Supplementary Figure S6).
Vancomycin: Analysis of two studies suggested a potential relation of vancomycin exposure to HL [OR = 1.65, 95% CI (0.97, 2.82), I^2^ = 84.9%, P = 0.06]. No significant association was found across vancomycin treatment duration and HL [OR = 1.32, 95% CI (0.89, 1.96), I^2^ = 78.4%, P = 0.17] (Supplementary Figures S19 and S20).
Association between birth weight and HL
3.2
Eight studies explored the impact of low birth weight on HL in NICU neonates. Overall meta-analysis showed a potential association between low birth weight and HL [OR = 1.31, 95% CI (0.99, 1.74), I^2^ = 65.6%, P = 0.06]. Stratified analysis by birth weight category revealed:
Very low birth weight (<1,500 g): Data from 4 studies indicated a significantly increased risk of HL in this weight group [OR = 0.94, 95% CI (0.22, 1.66), I^2^ = 72.8%, P = 0.01].
Low birth weight (1,500 g–2,500 g): Two studies showed an insignificant association between this weight range and HL [OR = 1.29, 95% CI (0.79, 2.13), I^2^ = 15.0%, P = 0.31) (Supplementary Figures S15–S17).
Association between surgical history and HL
3.3
Two studies evaluated the association between patent ductus arteriosus (PDA) surgical ligation and HL. Neonates with a history of PDA ligation had a significantly higher risk of HL [OR = 4.92, 95% CI (2.43, 9.95), I^2^ = 0.00%, P = 0.00] (Supplementary Figure S10).
Other relevant risk factors
3.4
Craniofacial anomalies/congenital head and neck deformities (six studies) were significantly linked to HL [OR = 6.55, 95% CI (4.91, 8.73), I^2^ = 46.3%, P = 0.00] (Supplementary Figure S2).
Family history of HL (four studies) was identified as a key risk factor for HL [OR = 7.35, 95% CI (3.29, 16.45), I^2^ = 0.00%, P = 0.00] (Supplementary Figure S3).
Hyperbilirubinemia (eight studies) was significantly related to HL [OR = 3.11, 95% CI (2.24, 4.31), I^2^ = 57.3%, P = 0.00] (Supplementary Figure S4).
Intracranial hemorrhage (two studies) was significantly linked to HL [OR = 2.57, 95% CI (1.36, 4.84), I^2^ = 0.00%, P < 0.01] (Supplementary Figure S5).
Regarding duration of oxygen therapy (three studies), prolonged oxygen therapy increased HL risk [OR = 2.00, 95% CI (1.30, 3.09), I^2^ = 83.8%, P < 0.01] (Supplementary Figure S9).
Meningitis (two studies) was significantly linked to HL [OR = 2.06, 95% CI (1.21, 3.51), I^2^ = 0.00%, P < 0.01] (Supplementary Figure S12).
TORCH infection (two studies) was significantly correlated with HL [OR = 5.27, 95% CI (2.00, 13.93), I^2^ = 0.00%, P < 0.01] (Supplementary Figure S14).
Mechanical ventilation (seven studies) was linked to HL [OR = 0.75, 95% CI (0.53, 0.98), I^2^ = 60.1%, P = 0.00) (Supplementary Figure S8).
Postnatal hypoxia/severe birth asphyxia (two studies) was linked to HL [OR = 0.81, 95% CI (0.42, 1.20), I^2^ = 68.7%, P = 0.00] (Supplementary Figure S18).
Risk factors with No significant association
3.5
Low Apgar score (four studies) has no significant association with HL [OR = 0.96, 95% CI (0.81, 1.13), I^2^ = 70.1%, P = 0.62] (Supplementary Figure S7).
Prematurity/shorter gestational age (4 studies) is not significantly associated with HL [OR = −1.10, 95% CI (−0.31, 0.11), I^2^ = 71.9%, P = 0.34] (Supplementary Figure S11).
Sex (three studies) is not significantly associated with HL [OR = 0.99, 95% CI (0.77, 1.28), I^2^ = 0.0%, P = 0.93] (Supplementary Figure S21).
Sepsis (two studies) has no significant association with HL [OR = 0.03, 95% CI (−0.31, 0.37), I^2^ = 0.00%, P = 0.86] (Supplementary Figure S22).
Supplementary Figures S23–S44 show the overall and individual results of the risk of bias assessment. No publication bias was noted, so no further elimination or revision was conducted for these studies.
Discussion
4
The incidence of HL among neonates admitted to the NICU (1%–10%) is substantially higher than that observed in healthy neonates (approximately 0.1%) (1, 2). As the first comprehensive meta-analysis to systematically evaluate risk factors for HL in NICU neonates, this study provides robust evidence to inform clinical risk stratification and surveillance strategies. Our findings reinforce that genetic susceptibility and environmental injury constitute the two principal dimensions underlying HL in NICU neonates. Genetic risk is exemplified by a family history of HL and pathogenic variants like GJB2 mutations, with previous reports indicating that up to 56% of nonsyndromic HL cases have a positive family history (33). Environmental factors identified in this meta-analysis include prolonged mechanical ventilation and hyperoxia exposure, which may damage cochlear hair cells through hypoxia, oxidative stress, and excessive noise exposure (12, 34). In addition, hyperbilirubinemia (total serum bilirubin >10 mg/dL) exerts neurotoxic effects on retrocochlear auditory pathways, significantly increasing HL risk (35), supporting enhanced auditory monitoring in these neonates.
Subgroup analyses based on birth weight revealed that very low birth weight (VLBW) infants (<1,500 g) have a significantly elevated risk of HL, whereas infants with birth weights ≥1,500 g do not demonstrate a statistically significant increase in hearing impairment. This disparity likely reflects differences in biological maturity and cumulative exposure to pathological and iatrogenic insults. VLBW infants are predominantly premature, with incomplete maturation of cochlear hair cells and delayed myelination of the auditory nerve, rendering them particularly vulnerable to hypoxia and oxidative stress. These infants frequently experience complications like respiratory distress syndrome and severe hyperbilirubinemia, which may disrupt cochlear microcirculation and induce neurotoxic injury to brainstem auditory nuclei. Moreover, the frequent need for prolonged mechanical ventilation and high-concentration oxygen therapy further exacerbates inner ear injury through acoustic trauma and free radical accumulation. However, newborns with a birth weight of >1,500 g, due to higher developmental maturity and less exposure to pathological and iatrogenic injuries, do not show obvious hearing risks (36, 37).
With respect to ototoxic medications, loop diuretics are widely used in the NICU for fluid management, yet their potential contribution to HL warrants careful consideration. Pooled analysis of studies by Eras, Hoog, and Robertson indicated that loop diuretic exposure may increase the risk of HL in premature NICU neonates. Experimental and clinical data suggest that intravenous administration at concentrations exceeding 50 μg/mL can alter endolymph composition and impair cochlear function (38, 39). Similarly, our meta-analysis confirmed a statistically significant association between aminoglycoside exposure and HL, reflecting their well-established ototoxic potential. Aminoglycosides induce cochlear injury primarily through disruption of cell membranes and interference with cellular metabolism (40). Ototoxicity varies by agent, with amikacin and netilmicin exhibiting relatively lower toxicity. Importantly, drug-induced HL is strongly modulated by genetic susceptibility, most notably the mitochondrial 12S rRNA m.1555A>G mutation, and by physiological vulnerability associated with prematurity and systemic inflammation, which can markedly amplify ototoxic effects (41). In adult studies, Vancomycin's HL risk shows a concentration dependence feature (42). When the serum concentration exceeds 40 mg/L, it may cause temporary SNHL, while a concentration of ≥80 mg/L may lead to permanent damage (43). Given the prolonged drug clearance and heightened vulnerability of extremely low birth weight infants, particularly those <1,000 g, subgroup analyses stratified by birth weight are likely essential for accurately evaluating vancomycin-associated HL risk in neonates. However, current evidence remains insufficient, highlighting a critical gap in the literature.
Beyond pharmacological factors, surgical ligation of PDA emerged as an important risk factor for HL. This association may reflect the combined effects of anesthetic neurotoxicity, intraoperative cerebral hemodynamic fluctuations, and underlying congenital vulnerabilities. The impact appears especially pronounced in extremely premature infants, consistent with previous reports (19).
This study has several notable strengths and innovations. First, it systematically validates the applicability of the JCIH risk indicators within the NICU population, clearly demonstrating the clinical relevance of core factors like craniofacial anomalies and family history of HL. Second, it expands the existing risk factor framework by identifying specific ototoxic agents (loop diuretics, aminoglycosides, and vancomycin) and NICU-specific interventions (e.g., PDA surgical ligation) not explicitly addressed in current JCIH guidelines, thereby filling an important gap in neonatal HL risk assessment.
Nevertheless, several limitations should be acknowledged. The limited number of eligible studies precluded subgroup analyses distinguishing sensorineural from conductive HL. Additionally, the small sample sizes in studies examining vancomycin exposure and PDA ligation possibly cause bias. Due to insufficient data, the association between small-for-gestational-age status and HL could not be evaluated, nor could the potential synergistic ototoxic effects of combined aminoglycoside and diuretic therapy be assessed. Future research should prioritize large-scale, multicenter prospective studies to elucidate the synergistic pathogenic interactions among genetic susceptibility, ototoxic medications, and hypoxic injury. Such studies are essential to define safe exposure thresholds for interventions like vancomycin administration and PDA surgery and to establish a more comprehensive, evidence-based risk assessment framework for HL in NICU neonates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lin CY Huang CY Lin CY Lin YH Wu JL. Community-based newborn hearing screening program in Taiwan. Int J Pediatr Otorhinolaryngol. (2004) 68(2):185–9. 10.1016/j.ijporl.2003.10.00714725985 · doi ↗ · pubmed ↗
- 2Wroblewska-Seniuk K Chojnacka K Pucher B Szczapa J Gadzinowski J Grzegorowski M. The results of newborn hearing screening by means of transient evoked otoacoustic emissions. Int J Pediatr Otorhinolaryngol. (2005) 69(10):1351–7. 10.1016/j.ijporl.2005.03.02315904979 · doi ↗ · pubmed ↗
- 3Zhou X Wang L Jin F Guo Y Zhou Y Zhang X The prevalence and risk factors for congenital hearing loss in neonates: a birth cohort study based on CHALLENGE study. Int J Pediatr Otorhinolaryngol. (2022) 162:111308. 10.1016/j.ijporl.2022.11130836116180 · doi ↗ · pubmed ↗
- 4Leigh JR Dettman SJ Dowell RC. Evidence-based guidelines for recommending cochlear implantation for young children: audiological criteria and optimizing age at implantation. Int J Audiol. (2016) 55(Suppl 2):S 9–18. 10.3109/14992027.2016.115726827142630 · doi ↗ · pubmed ↗
- 5Grasty MA Ittenbach RF Knightly C Solot CB Gerdes M Bernbaum JC Hearing loss after cardiac surgery in infancy: an unintended consequence of life-saving care. J Pediatr. (2018) 192:144–51.e 1. 10.1016/j.jpeds.2017.09.04929246336 PMC 6447030 · doi ↗ · pubmed ↗
- 6Wroblewska-Seniuk K Dabrowski P Greczka G Szabatowska K Glowacka A Szyfter W Sensorineural and conductive hearing loss in infants diagnosed in the program of universal newborn hearing screening. Int J Pediatr Otorhinolaryngol. (2018) 105:181–6. 10.1016/j.ijporl.2017.12.00729447811 · doi ↗ · pubmed ↗
- 7Maung M Lwin Y Aung N Tar T Phyu K. Diagnostic accuracy of distortion product otoacoustic emissions (DPOAE) and transient evoked otoacoustic emissions (TEOAE) in high risk newborn: a comparative study. Clin Pediatr. (2016) 1:2. 10.4172/2572-0775.1000110 · doi ↗
- 8Shang Y Hao W Gao Z Xu C Ru Y Ni D. An effective compromise between cost and referral rate: a sequential hearing screening protocol using TEOA Es and AAB Rs for healthy newborns. Int J Pediatr Otorhinolaryngol. (2016) 91:141–5. 10.1016/j.ijporl.2016.10.02527863628 · doi ↗ · pubmed ↗