Chewing efficiency and patient-centered outcomes in maxillary rehabilitation with zygomatic vs. conventional implant-supported fixed restorations
Lijuan Ye, Jie Li, Yuwei Dai, Xiaowan Ling, Lijun Yan, Feng Wang, Yiqun Wu

TL;DR
This study compares chewing efficiency and quality of life outcomes for two dental implant treatments in patients with upper jaw tooth loss.
Contribution
The study provides new evidence that zygomatic implants offer similar chewing efficiency but better quality of life compared to conventional implants.
Findings
Zygomatic and conventional implants showed comparable chewing efficiency based on subjective assessments and color mixing tests.
Patients with zygomatic implants reported better psychological and physical well-being according to OHIP-14 scores.
Implant success rates were high for both treatments, with 100% success at the implant level for zygomatic implants.
Abstract
This study aimed to assess whether zygomatic implant-supported fixed restorations (ZIFRs) provide comparable chewing efficiency and patient-centered outcomes to conventional implant-supported fixed restorations (CIFRs) in edentulous maxilla cases. A total of 29 patients were enrolled in this study. These patients with maxillary edentulism received ZIFR (16) or CIFR (13) treatment between October 2018 and April 2022. Chewing efficiency was evaluated by the subjective assessments of the scales of chewed gums and the variance of the Hue in a two-color chewing gum mixing ability test. In addition, the Oral Health Impact Profile-14 (OHIP-14) was employed to compare the oral health-related quality of life of patients between these two groups. There were no significant differences in chewing efficiency between the ZIFR and CIFR groups according to the results of the subjective assessments (P…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
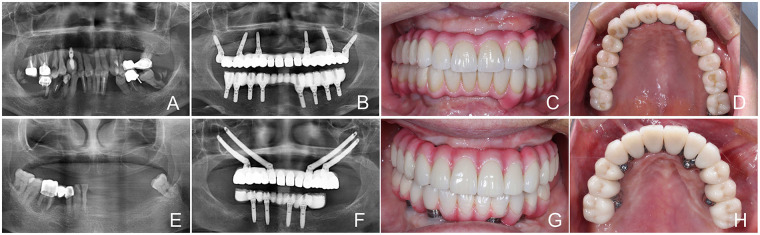 Figure 1
Figure 1 Figure 2
Figure 2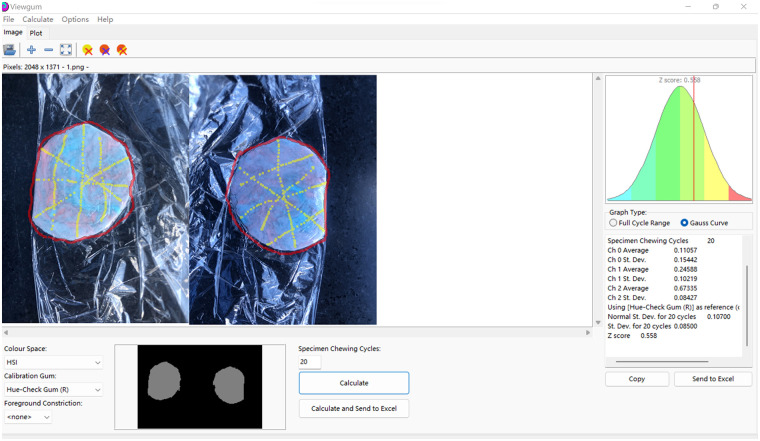 Figure 3
Figure 3| Patients | Age (years) | Gender | Cawood and Howell classification | Smoking | History of systematic disease | Opposing dentition | Immediate loading | No. of implants with BOP+ | No. of crowns | Implant numbers (position) | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Zygomatic implants | Conventional implants | Failed | ||||||||||
| 1 | 45 | Female | VI | No | No | D | Yes | 0 | 12 | 4 (16, 13, 23, 26) | 0 | 0 |
| 2 | 56 | Female | VI | No | Diabetic, Cardiovascular disease | N, D | Yes | 0 | 12 | 4 (15, 12, 22, 25) | 0 | 0 |
| 3 | 50 | Male | VI | Yes | Diabetic, Cardiovascular disease | N, D | Yes | 0 | 13 | 4 (15, 13, 33, 35) | 2 (11, 21) | 0 |
| 4 | 46 | Male | V | No | Hypertension | D | Yes | 0 | 12 | 2 (15, 25) | 4 (14, 12, 21, 23) | 0 |
| 5 | 52 | Male | V | No | No | N | Yes | 0 | 12 | 2 (16, 26) | 4 (14, 11, 24, 21) | 0 |
| 6 | 65 | Female | VI | No | No | N | NO | 0 | 12 | 4 (16, 13, 23, 26) | 0 | 0 |
| 7 | 62 | Male | VI | Yes | Hypertension | N | Yes | 4 | 14 | 4 (17, 15, 25, 27) | 0 | 0 |
| 8 | 33 | Female | VI | No | No | D | Yes | 0 | 12 | 4 (16, 13, 23, 26) | 2 (11, 21) | 0 |
| 9 | 43 | Male | V | No | Hypertension | D | Yes | 0 | 13 | 4 (16, 13, 23, 26) | 0 | 0 |
| 10 | 47 | Male | V | No | Depression | N, D | Yes | 0 | 12 | 2 (16, 26) | 4 (13,11,21,23) | 0 |
| 11 | 47 | Female | V | No | No | D | Yes | 6 | 12 | 2 (16, 26) | 4 (13, 11, 21, 23) | 0 |
| 12 | 45 | Female | V | No | No | N | Yes | 4 | 12 | 2 (16, 26) | 2 (13, 23) | 0 |
| 13 | 59 | Female | VI | No | No | N, D | Yes | 6 | 12 | 2 (16, 26) | 4 (13, 11, 21, 23) | 0 |
| Patients | Age (years) | Gender | Cawood and Howell classification | Smoking | History of systemic disease | Opposing dentition | Immediate loading | No. of implants with BoP+ | No. of crowns | Implant numbers (position) | Failed |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 67 | Female | VI | Yes | Diabetes | N | Yes | 6 | 12 | 6 (16, 14, 12, 22, 24, 26) | 0 |
| 2 | 63 | Female | VI | No | Hypertension | D | Yes | 0 | 14 | 6 (17, 14, 12, 22, 24, 27) | 0 |
| 3 | 62 | Male | VI | Yes | Hypertension | N | Yes | 1 | 12 | 7 (17, 15, 13, 11, 23, 25, 27) | 0 |
| 4 | 47 | Male | V | No | Diabetes | D | Yes | 0 | 12 | 6 (16, 14, 12, 21, 24, 26) | 0 |
| 5 | 74 | Female | VI | No | Hypertension, Diabetes | D | Yes | 3 | 12 | 7 (17, 16, 14, 13, 23, 25, 27) | 2 |
| 6 | 57 | Female | V | No | Cardiovascular disease | N | No | 0 | 12 | 6 (16, 14, 12, 22, 24, 26) | 0 |
| 7 | 50 | Male | V | Yes | Hypertension | D | No | 2 | 14 | 7 (16, 15, 12, 21, 22, 26, 27) | 0 |
| 8 | 40 | Female | V | No | No | N | Yes | 0 | 13 | 8 (17, 15, 13, 11, 21, 23, 25, 27) | 0 |
| 9 | 56 | Male | VI | Yes | No | N, D | Yes | 0 | 12 | 8 (17, 15, 13, 11, 21, 23, 25, 27) | 0 |
| 10 | 55 | Male | V | Yes | Hypertension | D | Yes | 0 | 13 | 6 (13, 11, 21, 23, 25, 27) | 0 |
| 11 | 59 | Female | VI | Yes | No | N, D | Yes | 1 | 12 | 6 (16, 14, 12, 22, 24, 26) | 0 |
| 12 | 50 | Male | V | Yes | No | D | Yes | 0 | 12 | 6 (16, 14, 12, 22, 24, 26) | 0 |
| 13 | 58 | Male | V | No | No | N, D | Yes | 0 | 12 | 6 (16, 14, 12, 22, 24, 26) | 0 |
| 14 | 40 | Female | VI | No | No | D | Yes | 0 | 12 | 6 (17, 15, 12, 22, 25, 27) | 0 |
| 15 | 58 | Male | V | Yes | No | D | No | 0 | 12 | 6 (16, 14, 12, 22, 24, 26) | 0 |
| 16 | 65 | Male | V | No | No | D | Yes | 0 | 14 | 8 (17, 15, 14, 12, 22, 24, 26, 27) | 0 |
| Strokes | SA | VOH | ||||
|---|---|---|---|---|---|---|
| ZIFR | CIFR | ZIFR | CIFR | |||
| First stroke | ||||||
| Mean/ | / | / | 0.59 | 0.401 | 0.456 | 0.55 |
| 95% CI | [0.294; 0.525] | [0.348; 0.557] | ||||
| Median | 4 | 3 | 0.383 | 0.464 | ||
| SD | / | / | 0.214 | 0.203 | ||
| Min | 3 | 2 | 0.064 | 0.136 | ||
| Max | 4 | 5 | 0.813 | 0.794 | ||
| Second stroke | ||||||
| Mean/ | / | / | 0.19 | 0.358 | 0.477 | 0.28 |
| 95% CI | [0.239; 0.503] | [0.365; 0.592] | ||||
| Median | 4 | 3 | 0.322 | 0.495 | ||
| SD | / | / | 0.233 | 0.214 | ||
| Min | 3 | 2 | 0.064 | 0.174 | ||
| Max | 5 | 5 | 0.794 | 0.843 | ||
| Dimensions | ZIFR | CIFR | Difference between ZIFR and CIFR | ||||
|---|---|---|---|---|---|---|---|
| Mean/ | SD | Mean/ | SD | Mean/ | SD | ||
| Functional limitations | 1 | 0.82 | 0.94 | 1 | 0.41 | −0.135 | 0.34 |
| [0.65; 1.35] | [0.56; 1.34] | [−0.706, 0.436] | |||||
| Physical pain | 0.62 | 0.64 | 0.75 | 1.04 | 0.01 | −0.24 | 0.32 |
| [0.35; 0.88] | [0.34; 1.22] | [−0.798, 0.318] | |||||
| Psychological discomfort | 0.77 | 0.63 | 0.94 | 1.33 | 0.01 | −0.192 | 0.38 |
| [0.46; 1.08] | [0.50; 1.47] | [−0.751, 0.367] | |||||
| Physical disability | 0.62 | 0.71 | 0.78 | 1.1 | 0.37 | −0.067 | 0.34 |
| [0.31; 0.92] | [0.41; 1.22] | [−0.637, 0.503] | |||||
| Psychological disability | 0.65 | 0.72 | 0.84 | 1.38 | 0.04 | −0.192 | 0.4 |
| [0.38; 0.96] | [0.38; 1.38] | [−0.751, 0.367] | |||||
| Social disability | 0.27 | 0.48 | 0.69 | 1.04 | 0.34 | −0.096 | 0.29 |
| [0.08; 0.50] | [0.31; 1.16] | [−0.655, 0.463] | |||||
| Handicap | 0.35 | 0.47 | 0.88 | 1.13 | 0.06 | −0.192 | 0.31 |
| [0.15; 0.58] | [0.44; 1.34] | [−0.751, 0.367] | |||||
| Global | 4.28 | 3.63 | 5.82 | 7.66 | <0.01 | −0.159 | 2.16 |
| [1.96; 6.58] | [1.98; 9.27] | [−5.72; 3.01] | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTemporomandibular Joint Disorders · Dental Implant Techniques and Outcomes · Dental materials and restorations
Introduction
Dental implants have been widely applied to repair dentition defects due to their considerable long-term success rates (1). Nevertheless, this strategy faces challenges in edentulous cases with severely atrophic maxillae, owing to inadequate bone volume surrounding dental implants (2). To overcome this issue, various approaches, such as maxillary sinus floor elevation, short implants, pterygoid implants, and zygomatic implants (3–7), have been proposed for dental implant-supported rehabilitations.
Among these approaches, zygomatic implants have gained increasing attention because of their high success rate and predictability in extremely atrophic maxillae (8). A systematic review documented a 12-year cumulative success rate of 95.21% across 4,556 zygomatic implants in 2,161 patients (9). However, some concerns remain regarding the complications of zygomatic implants, for example, maxillary sinusitis, infra-orbital paresthesia, oroantral fistula, and orbital perforations (10, 11). Although most studies have focused on these severe complications, chewing efficiency and patient-centered outcomes—the two main parameters for evaluating the efficacy of implant therapy after zygomatic implant treatment—have rarely been investigated.
Some characteristics of zygomatic implants may influence chewing efficiency and patient-centered outcomes. For potentially decreased chewing efficiency, zygomatic implant-supported fixed restorations (ZIFRs) involve short-span arch designs. Thus, the prostheses may even eliminate one or two premolars due to an aberrant form of the maxillary arch in patients with severely atrophic maxillae. In addition, ZIFRs frequently require a long cantilever in anterior areas to tackle complicated soft and hard tissue defects. ZIFRs may also lead to compromised postoperative quality of life for patients—for instance, by narrowing the space for tongue movement.
Whether these characteristics will negatively affect the chewing and postoperative subjective outcomes of patients remains unclear. Therefore, this study was designed to distinguish the chewing efficiency and patient-centered outcomes between ZIFRs and conventional implant-supported fixed restorations (CIFRs) in edentulous maxilla patients. The results of this study indicate that while chewing efficiency of ZIFRs is comparable with CIFRs, the patient-centered outcomes of ZIFRs are superior.
Materials and methods
Ethical approval
This study complied with the requirements of the Declaration of Helsinki requirements and was approved by the local ethics committee at Shanghai Ninth People's Hospital, Shanghai Jiao Tong University of Medicine, China (SH9H-2022-T25-1). All patients provided written informed consent.
Patient enrollment
A total of 29 edentulous maxilla patients were enrolled in this study according to the inclusion and exclusion criteria. These patients received either ZIFR or CIFR treatment in the Department of Second Dental Center, Shanghai Ninth People's Hospital, between October 2018 and April 2022. The inclusion criteria were as follows: (i) patients ≥18 years who provided written informed consent; (ii) edentulous maxilla patients [Cawood and Howell classification V and VI (12)] who had received ZIFR or CIFR treatment, including one-piece restorations and segmental bridges; (iii) prosthesis delivery completed more than one year prior to enrollment; and (iv) patients with intact mandibular dentition consisting of natural teeth, implant-supported restorations, or a combination of both. The exclusion criteria were as follows: (i) suffering due to uncontrolled systemic and/or mental diseases; (ii) impaired mandibular dentition; (iii) mandibular removable (partial/full) dentures and/or implant-supported overdentures; and (iv) malocclusal deformities and aberrant occlusal relationships.
Implant placement and success rate analysis
All implant placement procedures were performed by a senior specialist in dental implantology, Y. W., with the assistance of F. W. (Figure 1). In the ZIFR group, the quad zygoma protocol was applied that involved the following: Four zygomatic implants were bilaterally placed, or alternatively, a single zygomatic implant on each side combined with 2–4 conventional dental implants was applied, depending on the bone defect in the posterior areas of the maxillae (13). Success rates were evaluated at both the implant and patient levels, by the percentage of functional prostheses at the end of the last follow-up. Furthermore, mechanical complications, such as chipping, fracture of restorations, or loosening of abutment screws, were also recorded.
Representative cases of CIFR (A–D) and ZIFR (E–H). (A) Preoperative panoramic radiograph of a CIFR case; (B) panoramic radiograph after prosthesis delivery; (C) intraoral photograph; (D) intraoral photographs of the occlusal surface; (E) preoperative panoramic radiograph of a ZIFR case; (F) panoramic radiograph after prosthesis delivery; (G) intraoral photograph; and (H) intraoral photographs of the occlusal surface.
Chewing efficiency assessment
Chewing efficiency was evaluated using a two-color chewing gum mixing ability test (14). Each patient received a chewing gum strip consisting of blue and red gums (Mars Wrigley Confectionery, Guangzhou, China) (Figure 2). Patients were instructed to chew for 20 cycles, equally distributed between the left and right sides (stroke 1). After a 3-min rest, a second chewing cycle (stroke 2) was performed. The chewing cycles were counted by the investigators and patients. After chewing, the gum was collected in a transparent plastic pouch, avoiding any saliva accumulation within the pouch. Afterward, the collected chewing gums were flattened to a uniform 1 mm thickness for sequential scanning and visual analysis by Y. D. using Viewgum (http://www.dhal.com) (15) (Figure 3). Chewing efficiency was quantified based on the variance of the Hue (VOH) within the image (14). In addition, subjective assessments (SAs) of how much gum was mixed were performed by L. Y. and categorized into five scales: SA1, the chewing gum strip was unmixed, had cusp impressions, or was folded once; SA2, large chunks of unmixed chewing gum remained; SA3, bolus was partially mixed but contained traces of the original color that had not been mixed; SA4, well-combined bolus but not uniform in color; and SA5, uniform color with perfect mixing of the bolus.
Chewing gums and SAs. (A) Chewing strip consists of two gums with different colors; (B) SA2, most of chewing gum unmixed; (C) SA3, bolus slightly mixed, but bits of unmixed original color; (D) SA4, bolus well mixed, but color not uniform; and (E) SA5, bolus perfectly mixed with uniform color. White arrow: blue gum; yellow arrow: orange gum.
The Hue of images of chewed gum analyzed using Viewgum.
Patient-centered outcomes: OHRQoL assessed by OHIP-14 questionnaire
The Oral Health Impact Profile-14 (OHIP-14) was used to evaluate oral health-related quality of life (OHRQoL). The questionnaire assessed functional limitation, pain, physical and psychological incapacity, psychological discomfort, handicap, and social disability. Participants rated the frequency of these items utilizing a 5-point Likert scale: 0, 1, 2, 3, and 4 referring to “never,” “hardly ever,” “occasionally,” “fairly often,” and “very often,” respectively.
Statistical analysis
The statistical analyses included descriptive statistics and inferential statistics. Descriptive statistics—including means, medians, SD, minimum and maximum values, and 95% confidence intervals (CI)—were used to characterize the SA, VOH, and OHIP. A Mann–Whitney U test compared the VOH, SA, and OHIP values. In addition, cumulative implant survival rates were calculated and expressed as percentages. Statistical analyses were performed using SPSS Statistics 26 (IBM, Armonk, NY, USA), with significance set at P < 0.05.
Results
Demography information
A total of 29 patients were recruited for this study. The details of patient characteristics are summarized in Table 1. The ratio of patients with natural dentition, implant-supported fixed restorations, and a mix of the two in the mandible was 4:5:4 in the ZIFR group and 1:9:6 in the CIFR group. According to the Cawood and Howell classification, the distribution of patients of Classes V and VI in the ZIFR and CIFR groups was 6:7 and 9:7, respectively, demonstrating a comparable baseline of the atrophy of maxillae.
Survival and success rates of implants
All patients underwent follow-up 25.8 ± 3.6 months (mean ± SD, range: 12–48 months). In the ZIFR group, seven patients received the quad approach, while the others received bilaterally single ZIFR with 2–4 conventional dental implants (Table 1). The implant success rate in the ZIFR group was 100% at both the implant and patient levels (66/66 implants and 13/13 patients). In the CIFR group, 13 patients received 105 conventional dental implants (Table 2), and the success rate in the group was 98.1% at the implant level (103/105 implants) and 93.75% at the patient level (15/16 patients).
Rehabilitation strategy
After taking into consideration patient preference and budget, in the ZIFR group, five patients obtained a titanium framework and all-ceramic crowns; six individuals received a titanium framework and polymeric porcelain resin; and two received a titanium framework and acrylic resin prosthetic teeth. In the CIFR group, 11 participants received a one-piece titanium framework and all-ceramic crowns; four had a titanium framework alongside polymeric porcelain resin; and one participant had a titanium framework as well as acrylic resin prosthetic teeth.
Complications
Two patients in the CIFR group experienced chipping after 1 year of follow-up. Two patients in both the ZIFR group (2/13) and the CIFR group (2/16) complained about bruxism after prosthesis delivery, after which a night guard was provided.
Chewing efficiency assessment
Images of chewed gums were collected (Figure 3), and SAs and VOH values are provided in Table 3. Although the SA scores and VOH values of the CIFR group were higher, there was no significant difference after stroke 1 and stroke 2 chewing.
OHRQoL assessed by the OHIP-14 questionnaire
Following prosthesis delivery, all patients completed the OHIP-14 questionnaire. The ZIFR group demonstrated lower OHIP-14 scores than the CIFR group. Table 3 presents the seven dimensions of the OHIP-14 and related OHRQoL variables. With regard to the dimension of physical pain, the ZIFR group scored 0.62, while the CIFR group scored 0.75. Similarly, on the dimension of psychological discomfort and disability, the ZIFR group scored less than the CI group, which indicates that the zygomatic technique exerted less negative effect on patients' social life (Table 4).
Discussion
To our knowledge, this present study is the first one to explore chewing efficiency and postoperative quality of life of patients who have undergone ZIFR treatment for edentulous maxillae. Our findings suggest that the chewing efficiency of ZIFRs is comparable with that of CFRIs. In addition, ZIFRs present better postoperative quality of life for patients than CIFRs. Both ZIFR and CIFR strategies achieved considerable success rates for implants, with no severe complications identified. Taken together, ZIFRs represent an approach for reconstructing thoroughly impaired maxillary dentition, particularly in cases with extremely severe posterior bone defects.
The promising success rate of zygomatic implants has been well studied. A multicenter randomized clinical trial reported that zygomatic implants with immediate loading led to a significant increase in both prosthetic and implant success compared with sinus augmentation and delayed implant positioning after 1 year of follow-up (16). Similarly, Sales et al. reported a 96.7% success rate of ZIFRs after reviewing seven systematic reviews involving 2,313 patients with 4,812 zygomatic implants (17). In the present study, ZIFRs achieved a success rate consistent with a 17-year retrospective follow-up analysis. Although two failed implants occurred in the CIFR group (18), both were in a female patient—the oldest age among the 29 patients—who had two systemic diseases (hypertension and diabetes mellitus). These conditions could disturb normal osseointegration. The failure emphasizes the challenges and requirement for comprehensive evaluation when offering dental implant treatment to patients.
Based on the classification of atrophic maxillae, both the quad zygoma approach and single zygomatic implant with conversational implants were administered in the present study. The quad zygoma approach can reduce cantilever length and confer prosthetic stability, even allowing immediate prosthetic loading in severely atrophic edentulous maxillae (19). In this study, seven patients received quad zygoma implants due to severely resorbed maxillae. The chewing efficiency and postoperative reactions of these patients were not compared due to complicated influencing factors.
While ZIFRs demonstrated appealing clinical outcomes, their indications are restricted, as mentioned in abundant studies (20, 21). Owing to the long path that is adjacent to vital anatomic structures, it is imperative to manage and address mechanical and biological complications, such as pain, bruise, and recurrent maxillary sinusitis (22, 23). In the present study, various alternatives to ZIFR treatment were offered to patients, including lateral window sinus floor evaluation, onlay bone grafting, split bone block technique, and guided bone regeneration. In line with concerns regarding prolonged healing, unpredictable outcomes, and social needs, some patients opted for ZIFRs with immediate loading. Meanwhile, in some of the complicated ZIFR cases, dynamic navigation was employed to reduce surgical risks and achieve significant rehabilitation outcomes. No severe complications were observed during follow-up, and a prolonged evaluation is ongoing.
Although chewing gum has been widely used in evaluating chewing efficiency of implant-supported overdentures (24), there have been no studies comparing the efficiency of ZIFRs and CIFRs. Chewing gum is a time-saving, straightforward, and economical approach, enabling its application in geriatric wards or private practices in the absence of specific equipment or trained staff. In addition, gum has an elastic consistency, facilitating maximum muscle activation.
Although many questionnaires have been used to assess the quality of life, not all are suitable for evaluating OHRQoL. Among these questionnaires, OHIP is the prevailing one in OHRQoL evaluation (25). Originally proposed by Slade and Spencer in 1994 (26), OHIP aims to provide comprehensive data on patient attitudes regarding influence on their wellness. However, not all studies employ the full suite of 49 questions. Compared to the full OHIP, OHIP-14 has demonstrated excellent consistency, accuracy, and precision, making it more practical in clinical practice (27). Therefore, OHIP-14 has become widespread in dental research. In this study, the OHIP-14 scores of patients revealed a statistical difference between these two groups. In terms of physical pain, the ZIFR group scored lower than the CIFR group, which may be attributed to the use of general anesthesia to some extent. Similarly, on the dimension of psychological discomfort and disability, the ZIFR group performed better than the CIFR group, indicating that ZIFRs exert less negative impact on patients’ social life. However, the observed differences may not reflect authentic clinical discrepancies. A change of ≥3 points in OHIP-14 is generally considered meaningful (28); however, in this study, the change was less than 1, which may be attributed to the small sample size.
All procedures and analyses were conducted under realistic conditions in this study, providing clinical and instructive insights for future research. The data indicate that chewing efficiency between ZIFRs and CIFRs is comparable. In addition, postoperative quality of life is better in the ZIFR group. Nonetheless, caution should be exercised while interpreting outcomes due to the limited sample size. To generate stronger evidence, prolonged follow-ups and randomized controlled trials should be scheduled.
Conclusions
Preliminary data reveal that the chewing efficiency of ZIFRs does not statistically differ from CIFRs. Moreover, ZIFRs are associated with higher patient satisfaction in the rehabilitation of edentulous maxillae compared with CIFRS. These findings suggest that ZIFRS represent a promising alternative to CIFRs in certain conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rojas M Chauca Bajaña L Rodríguez Tates M Poussin L Velásquez Ron B. Oral health-related quality of life in patients rehabilitated with dental implants. Healthcare (Basel). (2025) 13:813. 10.3390/healthcare 1307081340218110 PMC 11989169 · doi ↗ · pubmed ↗
- 2Mertens C Freier K Engel M Krisam J Hoffmann J Freudlsperger C. Reconstruction of the severely atrophic edentulous maxilla with calvarial bone grafts. Clin Oral Implants Res. (2017) 28:749–56. 10.1111/clr.1287327198206 · doi ↗ · pubmed ↗
- 3Nguyen TTH Eo MY Kuk TS Myoung H Kim SM. Rehabilitation of atrophic jaw using iliac onlay bone graft combined with dental implants. Int J Implant Dent. (2019) 5:11. 10.1186/s 40729-019-0163-930887237 PMC 6423193 · doi ↗ · pubmed ↗
- 4Araujo RZ Santiago Júnior JF Cardoso CL Benites Condezo AF Moreira Júnior R Curi MM. Clinical outcomes of pterygoid implants: systematic review and meta analysis. J Craniomaxillofac Surg. (2019) 47:651–60. 10.1016/j.jcms.2019.01.03030799134 · doi ↗ · pubmed ↗
- 5Esfahrood ZR Ahmadi L Karami E Asghari S. Short dental implants in the posterior maxilla: a review of the literature. J Korean Assoc Oral Maxillofac Surg. (2017) 43:70–6. 10.5125/jkaoms.2017.43.2.7028462189 PMC 5410430 · doi ↗ · pubmed ↗
- 6Pieri F Caselli E Forlivesi C Corinaldesi G. Rehabilitation of the atrophic posterior maxilla using splinted short implants or Sinus augmentation with standard-length implants: a retrospective cohort study. Int J Oral Maxillofac Implants. (2016) 31:1179–88. 10.11607/jomi.437027632276 · doi ↗ · pubmed ↗
- 7Agliardi EL Romeo D Panigatti S de Araújo Nobre M MalóP. Immediate full arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: a prospective clinical study with minimum follow-up of 6 years. Int J Oral Maxillofac Surg. (2017) 46:1592–9. 10.1016/j.ijom.2017.05.02328655434 · doi ↗ · pubmed ↗
- 8Andre A Dym H. Zygomatic implants: a review of a treatment alternative for the severely atrophic maxilla. Atlas Oral Maxillofac Surg Clin North Am. (2021) 29:163–72. 10.1016/j.cxom.2021.04.00134325806 · doi ↗ · pubmed ↗