A Case of Upper Tract Urothelial Carcinoma With Neuroendocrine Differentiation Successfully Treated With Enfortumab Vedotin and Pembrolizumab
Kosei Taniguchi, Mamoru Hashimoto, Takahito Nakayama, Saizo Fujimoto, Shingo Toyoda, Takashi Kikuchi, Marco Antonio De Velasco, Osamu Maenishi, Takafumi Minami, Kazutoshi Fujita

TL;DR
A rare case of upper tract urothelial carcinoma with neuroendocrine features was successfully treated with a combination of enfortumab vedotin and pembrolizumab.
Contribution
This case demonstrates the potential effectiveness of enfortumab vedotin plus pembrolizumab in treating a rare and aggressive cancer subtype.
Findings
Enfortumab vedotin plus pembrolizumab achieved a complete response in a patient with UC-NE.
Nectin-4 expression was strong in the urothelial component but weak in the neuroendocrine component.
The treatment combination maintained remission after three cycles.
Abstract
Upper tract urothelial carcinoma with neuroendocrine differentiation (UC‐NE) is extremely rare and generally associated with aggressive behavior and poor prognosis. Optimal treatment strategies remain unclear, particularly regarding the role of nectin‐4–targeted therapy. A 61‐year‐old man was diagnosed with UC‐NE of the renal pelvis. Laparoscopic nephroureterectomy revealed invasive UC‐NE with lymphatic invasion (pT1, G2) and carcinoma in situ of the ureter (pTis, G1). Immunohistochemistry showed strong nectin‐4 expression in the urothelial component but only weak to moderate expression in the neuroendocrine component. Ten months after surgery, para‐aortic and bilateral pelvic lymph node recurrence developed. Treatment with enfortumab vedotin (EV) plus pembrolizumab achieved a complete response after 3 cycles, and remission was maintained with continued therapy. This case suggests…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
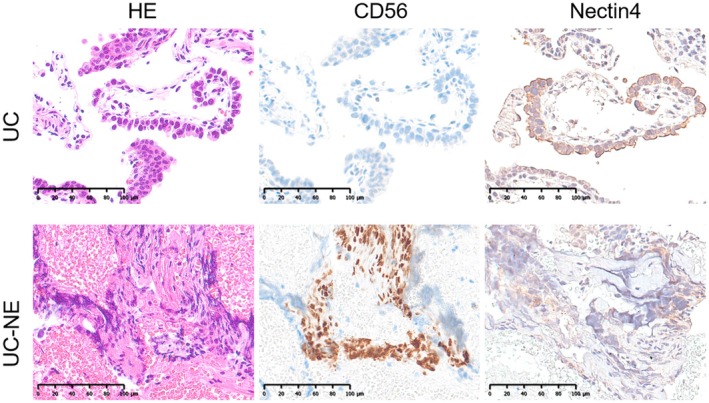 FIGURE 1
FIGURE 1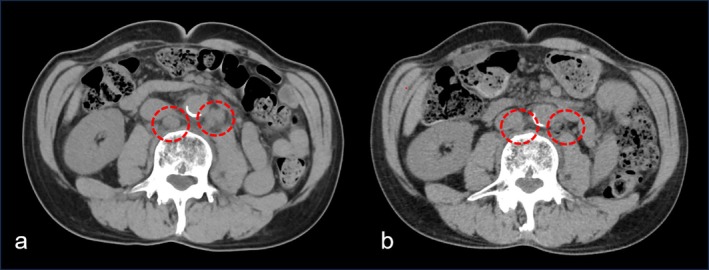 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary and Genital Oncology Studies · Neuroendocrine Tumor Research Advances
Introduction
1
Urothelial carcinoma (UC) is classified into upper tract urothelial carcinoma (UTUC) and lower tract UC. UTUC is relatively uncommon accounting for only 5%–10% of all UC cases and is associated with a poorer prognosis [1, 2]. Within this subset, UC with neuroendocrine differentiation (UC‐NE) is exceedingly rare. Such tumors are frequently diagnosed at advanced stages and are linked to unfavorable clinical outcomes [3].
For neuroendocrine malignancies, cisplatin plus etoposide has been regarded as the standard regimen. However, survival in patients with neuroendocrine bladder cancer remains extremely poor even with this approach [4]. Notably, the efficacy of enfortumab vedotin (EV), an antibody–drug conjugate targeting nectin‐4, largely depends on the level of nectin‐4 expression. Previous studies have demonstrated that nectin‐4 expression is usually minimal or absent in bladder cancer with neuroendocrine differentiation [5, 6], raising concerns about the therapeutic applicability of EV in this histologic subtype.
Recently, the combination of EV and pembrolizumab has emerged as a promising first‐line therapy for advanced UC [7]. However, its effectiveness in UTUC harboring neuroendocrine features has not yet been reported. Here, we present a rare case of UC‐NE arising in the upper urinary tract, which recurred shortly after surgery but subsequently achieved a durable remission with EV plus pembrolizumab despite limited nectin‐4 expression.
Case Presentation
2
A 61‐year‐old man was referred to our department due to the microscopic hematuria during routine health screening. Urinary cytology revealed class IV suspicious cells, but cystoscopy did not detect any bladder tumors. Laboratory findings were unremarkable except for microscopic hematuria (10–19 RBC/HPF). The patient had no history of chronic kidney disease, diabetes mellitus, or other renal dysfunction.
Contrast‐enhanced CT showed no apparent lesions, and retrograde pyelography revealed no filling defects. Ureteroscopy, however, demonstrated a papillary tumor localized in the left renal pelvis. Urinary cytology was suspicious in the left renal pelvis/ureter and negative in the right. Ureteroscopic biopsy confirmed the diagnosis of UC‐NE. The tumor predominantly showed typical UC morphology, but focal areas of small cells with nuclear atypia were present. Immunohistochemistry (IHC) demonstrated positivity for CD56 and INSM1, confirming neuroendocrine differentiation. The percentage of neuroendocrine features per cancer cells populations was 16% based on Ai calculation. No distant metastases were identified, and the clinical stage was cT2N0M0. The patient underwent laparoscopic left nephroureterectomy. Invasive UC‐NE of the renal pelvis with lymphatic invasion (pT1, G2) and carcinoma in situ in the left ureter (pTis, G1), without vascular invasion. IHC revealed that the UC area was negative for CD56 but showed strong positivity for nectin‐4. In contrast, the UC‐NE area exhibited strong CD56 positivity and weak to moderate nectin‐4 staining (Figure 1). Nectin‐4 IHC was performed using an anti‐Nectin‐4 monoclonal antibody (dilution 1:1600, clone EPR15613‐68, Abcam, Cambridge, UK). Template‐based lymph node dissection was omitted because the disease was clinically node‐negative, and limited para‐aortic lymph node sampling revealed no malignancy. The patient was placed on surveillance without adjuvant therapy.
Immunohistochemical staining of the tumor. Representative photomicrographs demonstrate distinct expression profiles: The urothelial carcinoma (UC) component was negative for CD56 and strongly positive for nectin‐4, whereas the UC with neuroendocrine differentiation (UC‐NE) component showed strong CD56 positivity and weak to moderate nectin‐4 staining.
Ten months after surgery, follow‐up CT revealed multiple enlarged lymph nodes in the para‐aortic and bilateral pelvic regions, consistent with recurrence (Figure 2a). At the time of recurrence, neuroendocrine tumor‐related serum markers were evaluated, revealing a neuron‐specific enolase (NSE) level of 8.2 ng/mL and a pro–gastrin‐releasing peptide (proGRP) level of 48 pg/mL, neither of which was elevated. No visceral or bone metastases were observed. Systemic therapy with EV plus pembrolizumab was initiated. After three cycles, CT showed a significant reduction in metastatic lymph node size, consistent with a complete response (Figure 2b). After 13 cycles (~12 months), remission was maintained. Adverse events included Grade 2 alopecia and Grade 2 ocular dryness, both manageable with supportive care. No severe adverse events occurred.
CT images showing recurrent lymphadenopathy and response to systemic therapy. Ten months after surgery, CT scans revealed enlarged para‐aortic and bilateral pelvic lymph nodes (a). Following three cycles of enfortumab vedotin plus pembrolizumab, the metastatic lymph nodes showed marked reduction in size consistent with a complete response to systemic therapy (b).
Discussion
3
This case represents a rare case of UC‐NE of the renal pelvis with early nodal recurrence that responded remarkably to EV plus pembrolizumab. The efficacy of EV depends on expression of its target antigen, nectin‐4 [5]. While nectin‐4 expression is generally low in bladder cancer patients with UC‐NE [6], it remains unclear whether patients with UTUC with UC‐NE also exhibit similarly limited nectin‐4 expression. Nectin‐4 is predominantly expressed in luminal subtypes of UC. Previous studies have reported that UTUC patients tend to exhibit luminal rather than basal subtype profiles [8, 9]. However, there are no reports of nectin‐4 expression in UTUC patients with NE differentiation. In our analysis, weak to moderate nectin‐4 staining was observed in the UC‐NE tissue, suggesting that the patient may have been responsive to EV in combination with pembrolizumab therapy.
Typical UC often exhibits an “inflamed” phenotype characterized by abundant intratumoral infiltration of CD8^+^ T cells [10]. In contrast, UC‐NE more frequently displays an “immune‐excluded” pattern, which suggests a potentially limited efficacy of immunotherapy [11]. However, independently of PD‐L1 status, the tumor immune microenvironment plays a critical role in determining treatment responses [10, 11]. Several studies have shown that platinum‐based chemotherapy combined with an immune checkpoint inhibitor is effective in NE tumors, inducing the expansion of CD8^+^ T‐cell clones and correlating with improved survival [12, 13]. Furthermore, inhibition of nectin‐4 signaling not only triggers cytotoxic effects against tumor cells but also activates natural killer cells, enhancing antitumor immunity [14]. A previous study further revealed that T cells are capable of eliminating both antigen‐positive and neighboring antigen‐negative tumor cells through a mechanism known as bystander killing, which helps the clearance of heterogeneous tumors [15]. Based on these findings, it is plausible that an immune response was initiated in the UC regions following EV plus pembrolizumab therapy, which subsequently extended to adjacent UC‐NE regions, contributing to overall tumor control.
Several limitations should be acknowledged. First, we were unable to perform immunohistochemical evaluation of nectin‐4 in the recurrent lymph node lesions, leaving uncertainty about the antigen status in the metastatic sites. Second, it remains possible that the recurrent tumors contained predominantly conventional UC rather than neuroendocrine components, which could have contributed to the favorable response to EV plus pembrolizumab.
In summary, this case underscores the importance of evaluating nectin‐4 expression when considering therapeutic strategies for UC‐NE. Further study is warranted to validate the efficacy of EV plus pembrolizumab therapy in UTUC patients with UC‐NE.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1E. Tomiyama , K. Fujita , M. Hashimoto , et al., “Comparison of Molecular Profiles of Upper Tract Urothelial Carcinoma vs. Urinary Bladder Cancer in the Era of Targeted Therapy: A Narrative Review,” Transl Androl Urol 11, no. 12 (2022): 1747–1761.36632153 10.21037/tau-22-457PMC 9827402 · doi ↗ · pubmed ↗
- 2M. Hashimoto , K. Fujita , T. Nakayama , et al., “Higher Neutrophil‐To‐Lymphocyte Ratio After the First Cycle of the First‐Line Chemotherapy Is Associated With Poor Cancer Specific Survival of Upper Urinary Tract Carcinoma Patients,” Transl Androl Urol 10, no. 7 (2021): 2838–2847.34430386 10.21037/tau-21-185PMC 8350230 · doi ↗ · pubmed ↗
- 3M. R. Alharbi , A. Meliti , and A. Alomran , “Mixed Neuroendocrine Carcinoma and Urothelial Carcinoma of the Upper Urinary Tract: A Case Report and Literature Review,” Cureus 17, no. 3 (2025): e 80275, 10.7759/cureus.80275.40201869 PMC 11976323 · doi ↗ · pubmed ↗
- 4A. Bex , J. A. Nieuwenhuijzen , M. Kerst , et al., “Small Cell Carcinoma of Bladder: A Single‐Center Prospective Study of 25 Cases Treated in Analogy to Small Cell Lung Cancer,” Urology 65, no. 2 (2005): 295–299, 10.1016/j.urology.2004.09.049.15708041 · doi ↗ · pubmed ↗
- 5C. E. Chu , M. Sjöström , E. A. Egusa , et al., “Heterogeneity in NECTIN 4 Expression Across Molecular Subtypes of Urothelial Cancer Mediates Sensitivity to Enfortumab Vedotin,” Clinical Cancer Research 27, no. 18 (2021): 5123–5130, 10.1158/1078-0432.CCR-20-4175.34108177 PMC 8634828 · doi ↗ · pubmed ↗
- 6J. H. Hoffman‐Censits , K. A. Lombardo , V. Parimi , et al., “Expression of Nectin‐4 in Bladder Urothelial Carcinoma, in Morphologic Variants, and Nonurothelial Histotypes,” Applied Immunohistochemistry & Molecular Morphology 29, no. 8 (2021): 619–625, 10.1097/PAI.0000000000000938.33901032 PMC 8429050 · doi ↗ · pubmed ↗
- 7J. E. Rosenberg , P. H. O'Donnell , A. V. Balar , et al., “Pivotal Trial of Enfortumab Vedotin Plus Pembrolizumab for Advanced Urothelial Carcinoma,” New England Journal of Medicine 389, no. 14 (2023): 1283–1293.
- 8M. Hashimoto , K. Fukiage , T. Minami , et al., “Treatment Strategies for Locally Advanced and Metastatic Urothelial Carcinoma Based on Molecular Profiles: A Review,” Histology and Histopathology 24 (2025): 18972, 10.14670/HH-18-972.40762043 · doi ↗ · pubmed ↗