Optimal timing of enteral nutrition initiation in critically ill patients: a network meta-analysis
Ming Dai, Hong-Wei Yang, You Zhou, Qian Guo, Yuan Meng, Yun Lei Sun, Pei-Ya Hu

TL;DR
This study compares the best time to start feeding critically ill patients through the gut to improve outcomes like survival and ICU stay.
Contribution
A network meta-analysis comparing five enteral nutrition initiation timings to identify the most effective window for clinical outcomes in critically ill patients.
Findings
Initiating enteral nutrition within 24–48 hours may be associated with lower mortality.
Initiating enteral nutrition beyond 96 hours is most likely to shorten ICU length of stay.
No significant differences in mortality or ICU length of stay were observed between other initiation timings.
Abstract
Nutritional support is pivotal in managing critically ill patients. Enteral nutrition, which preserves intestinal mucosal barrier function and modulates immune-metabolic homeostasis, is the preferred nutritional support strategy. However, the optimal timing for initiating EN remains controversial: some studies advocate early initiation (within 24–48 h), while others suggest delayed initiation (beyond 48 h), resulting in inconsistent clinical practices and conflicting guideline recommendations. This highlights the need for high-quality evidence to clarify the optimal EN initiation window. This network meta-analysis aims to systematically compare the effects of five EN initiation timings on key clinical outcomes in critically ill patients, rank their efficacy, and identify the optimal initiation window, thereby providing evidence-based guidance for clinical practice. We conducted a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
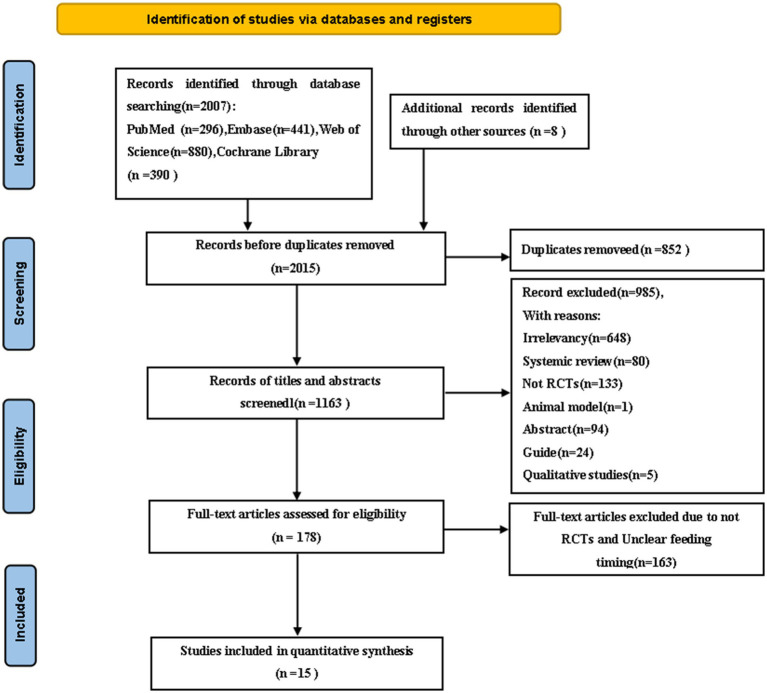 Figure 1
Figure 1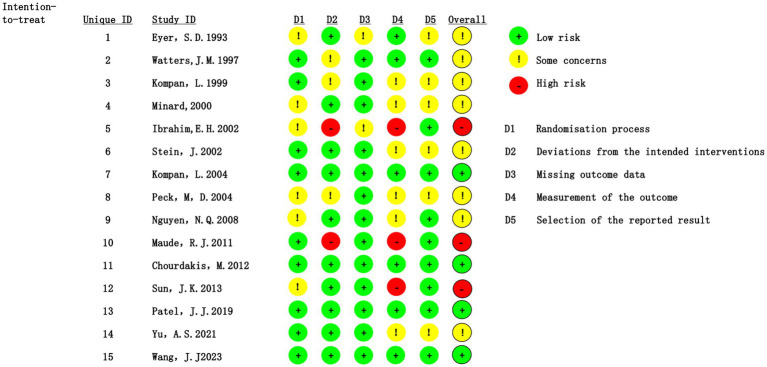 Figure 2
Figure 2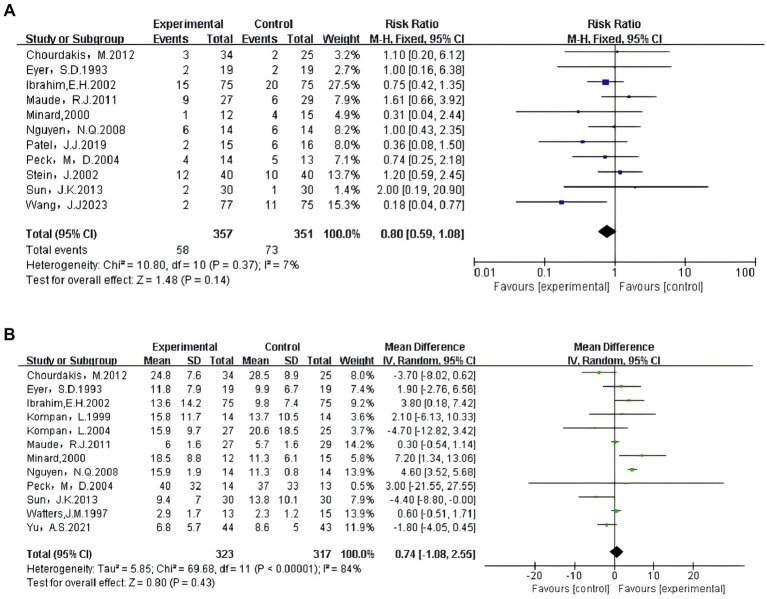 Figure 3
Figure 3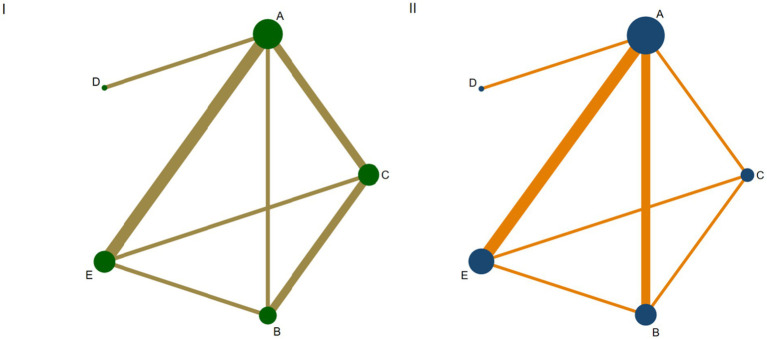 Figure 4
Figure 4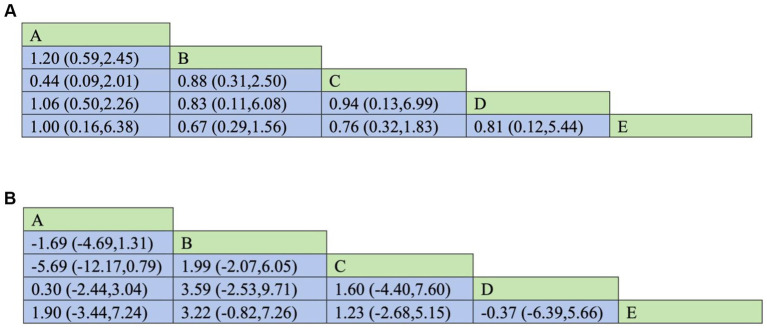 Figure 5
Figure 5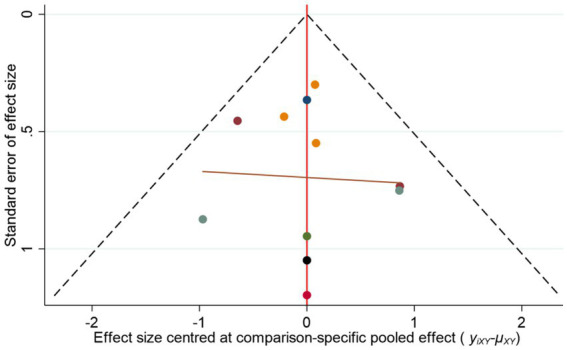 Figure 6
Figure 6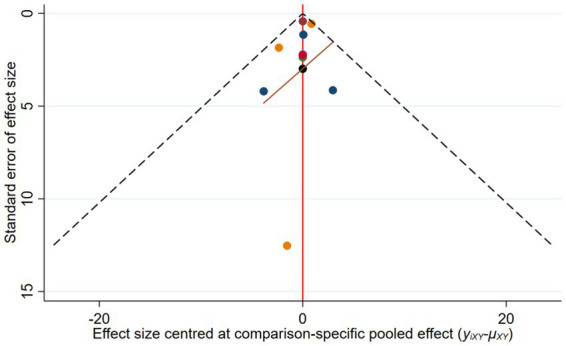 Figure 7
Figure 7| Study | Country | Sample size③ (C/T) | Age③ (C/T) | Gender④ (M/F)③ (C/T) | Disease type | Enteral feeding timing③ (C/T) | Outcome | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| ( | USA | 19 | 19 | 41 ± 18 | 44 ± 22 | 8/11 | 14/5 | Blunt trauma | 72–96 h | <24 h | ① ② |
| ( | Canada | 15 | 13 | 61 ± 12 | 64 ± 11 | 11/4 | 11/2 | Abdominal or thoracic surgery | >96 h | <24 h | ② |
| ( | Slovenia | 14 | 14 | 44.7 ± 15.9 | 38.4 ± 15.6 | 10/4 | 14/0 | Multiple organ failure (MOF) in multiply injured patients. | 24–48 h | <24 h | ② |
| ( | USA | 15 | 12 | 36 ± 11 | 30 ± 13 | 10/5 | 9/3 | Severe closed-head injuries | >96 h | 48–72 h | ①② |
| ( | USA | 75 | 75 | 59.1 ± 19.0 | 56.5 ± 15.6 | 35/40 | 28/47 | Mechanically ventilated patients | >96 h | <24 h | ①② |
| ( | Germany | 40 | 40 | 67 ± 13 | 62 ± 18 | 17/23 | 16/24 | After percutaneous endoscopic gastrostomy | 24–48 h | <24 h | ① |
| ( | Slovenia | 25 | 27 | 41.5 ± 16.8 | 42.6 ± 17.9 | 21/4 | 24/3 | Gastric intolerance and subsequent pneumonia | 24–48 h | <24 h | ② |
| ( | USA | 13 | 14 | 49 ± 19 | 44 ± 24 | 10/3 | 9/5 | Burn injury | >96 h | <24 h | ①② |
| ( | Australia | 14 | 14 | 56.3 ± 3.4 | 54.9 ± 3.3 | 10/4 | 8/6 | Critically ill patients | >96 h | <24 h | ①② |
| ( | Thailand | 29 | 27 | 37.8 ± 53.0 | 36.6 ± 49.3 | 2/27 | 8/19 | Cerebral malaria | 48–72 h | <24 h | ①② |
| ( | Greece | 25 | 34 | 33.30 ± 12.96 | 36.13 ± 14.72 | 21/4 | 26/8 | Traumatic brain injury | 48–72 h | 24–48 h | ①② |
| ( | China | 30 | 30 | 42.8 ± 12.8 | 43.9 ± 13.2 | 18/12 | 20/10 | Severe acute pancreatitis | >96 h | 24–48 h | ①② |
| ( | USA | 16 | 15 | 56 ± 16 | 64 ± 14 | 8/8 | 10/5 | Septic shock | 48–72 h | <24 h | ① |
| ( | China | 43 | 44 | ⑤ | ⑤ | ⑤ | ⑤ | Critically ill patients | 24–48 h | <24 h | ② |
| ( | China | 75 | 77 | 45.48 ± 9.32 | 46.37 ± 9.94 | 40/35 | 44/33 | Traumatic intracerebral hemorrhage (TICH) | 48–72 h | 24–48 h | ① |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Nutrition and Gastroenterology · Enhanced Recovery After Surgery · Nutrition and Health in Aging
Introduction
1
Critically ill patients are characterized by unstable or potentially unstable vital signs, with one or more organ systems impaired, thereby posing an immediate life threat (1). Advances in critical care have significantly improved ICU treatment standards, contributing to a steady decline in mortality over recent decades (2). However, these patients frequently develop severe malnutrition due to their inherent hypercatabolic and hypermetabolic states, combined with inadequate nutrient intake during critical illness (3). In ICUs, the prevalence of malnutrition ranges from 38 to 78%, which independently exacerbates poor outcomes (4). Specifically, malnutrition in critically ill patients is associated with prolonged mechanical ventilation, impaired wound healing, increased complications, extended hospital stays, and elevated mortality (5, 6). Long-term consequences include reduced quality of life and substantial economic burdens on families (5, 7). Therefore, effective clinical nutritional support is critical for improving malnutrition and clinical outcomes in critically ill patients (8).
Nutritional support modalities include enteral nutrition (EN) and parenteral nutrition (PN). EN delivers nutrients via the gastrointestinal tract, whereas PN provides nutrients intravenously, bypassing the gut (9). EN preserves the structure and function of the gastrointestinal tract by simulating physiological feeding, promoting intestinal motility, supporting digestive enzyme secretion, and reducing bacterial translocation (10). Compared to PN, EN is associated with fewer severe complications (e.g., catheter-related infections, metabolic disturbances, and hepatic dysfunction), though minor adverse events such as diarrhea or bloating may occur (11). Therefore, when the gastrointestinal tract is functioning properly, EN is the preferred method of nutritional support.
A landmark meta-analysis found that EN initiated within 24 h of ICU admission significantly improved outcomes and reduced mortality (12). In contrast, a recent meta-analysis reported that EN started within 24–48 h did not significantly shorten ICU or hospital stays in critically ill patients (13), highlighting conflicting evidence. Guidelines also differ: the 2016 SCCM/ASPEN guidelines emphasize that EN better preserves intestinal mucosal integrity, stabilizes gut microbiota, and regulates immune-metabolic function compared to PN, advocating EN as the preferred route (14–17). They recommend initiating EN within 24–48 h of ICU admission once hemodynamic stability is achieved (18). Conversely, the European Society for Clinical Nutrition and Metabolism (ESPEN) guidelines suggest considering nutritional support for ICU patients hospitalized beyond 48 h (3), reflecting inconsistent recommendations.
Network meta-analysis extends traditional pairwise meta-analysis by enabling simultaneous comparison of multiple interventions and ranking their effectiveness and safety based on integrated direct and indirect evidence (19). This approach enhances the accuracy of results by leveraging a broader evidence network, making it well-suited to resolve controversies involving multiple time windows. Accordingly, we conducted a network meta-analysis to systematically compare the effects of five EN initiation timings on clinical outcomes in critically ill patients, aiming to identify the optimal window and provide evidence-based guidance for clinical practice.
Methods
2
Our study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA-NMA) statement for network meta-analyses (20). The study protocol was registered on the PROSPERO platform (registration number: CRD42024581390; Registration Date: September 4, 2024). The full registration protocol and study details are publicly accessible at: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024581390.
Inclusion and exclusion criteria
2.1
The inclusion and exclusion criteria were developed according to the PICOS principle. Included studies were: (1) Population: Adult patients (aged ≥ 18 years) admitted to the ICU who required EN. We included studies enrolling a broad spectrum of critically ill patients, such as those with trauma (e.g., blunt trauma, traumatic brain injury), post-operative status (e.g., abdominal or thoracic surgery), severe infections (e.g., septic shock), neurological injuries, severe acute pancreatitis, and burns. (2) Intervention: The interventions in this study included different timing points for initiating enteral nutrition in critically ill patients, specifically categorized as <24 h, 24–48 h, 48–72 h, 72–96 h, and >96 h. (3) Outcomes: mortality rate; ICU length of stay. (4) Study design: randomized controlled trials (RCTs). Excluded studies were: (1) Those failing to clearly delineate the timing of enteral feeding initiation; (2) Those involving patients receiving parenteral nutrition or enteral feeding combined with parenteral nutrition; (3) Studies written in a language other than English; (4) Studies with incomplete data or source data or full-text files could not be obtained after contacting the corresponding author; (5) Conference abstracts duplicated across multiple events or published excessively. Detailed baseline characteristics of the included patients, including the distribution of clinical conditions, are summarized in Table 1.
Search strategy
2.2
We conducted a network meta-analysis by searching four databases: PubMed, Embase, Web of Science, and Cochrane Library databases were searched from inception to September 2024. Only English-language articles published during this timeframe were included. Reference lists from all selected primary studies and review articles were also examined for additional relevant citations. A detailed search strategy is outlined in Appendix 1. The main search strategies were as follows: (“Intensive Care Units”[MeSH] OR”critical care unit”[Text Word]) AND (“Enteral Nutrition”[MeSH] OR “Enteral Feeding”[Text Word]) AND (“Randomized controlled trial”[Text Word]).
Study selection
2.3
After removing duplicate records, two researchers (MD and YM) separately screened the titles and abstracts of the related articles in the initial stage. Then, the full-text articles were assessed to check if they met all the inclusion and exclusion criteria. Any disagreement or uncertainty between the two researchers was solved by discussion or consultation with a third researcher (PYH).
Data extraction
2.4
Two researchers (MD and HWY) separately extracted data using a Excel 2021 form, which was designed based on the guidelines from the Cochrane Handbook for Systematic Reviews of Interventions (21). Any disagreements were resolved through rechecking the original research and discussion with another researcher (PYH). For each study, we extracted the following information: author(s), age, gender, year of publication, title, study design, sample size, timing of initiating enteral nutrition, and corresponding outcome variables.
Risk of bias and grade of evidence assessment
2.5
Two researchers (MD and YM) used the revised Cochrane Risk of Bias tool (version 2), and any disagreements were resolved through discussion with another reviewer (PYH) (22). Bias was assessed across five domains. The risk of bias for each domain was assessed as high risk, low risk, or some concern. We used the Grading of Recommendation, Assessment, Development, and Evaluation criteria to evaluate the overall evidence quality in five aspects: (1) bias risk, (2) inconsistency, (3) indirectness, (4) imprecision, and (5) publication bias. The evidence quality can be divided into high, moderate, low, or very low levels (23).
Statistical analysis
2.6
First, pairwise meta-analyses were performed using RevMan 5.4 to conduct direct comparisons. In data analysis, binary variables were expressed using RR (risk ratio) values, and continuous variables were expressed using MD (mean difference) values (21). To assess between-study heterogeneity, researchers used the I^2^ statistic and visually inspected forest plots. When I^2^ = 0, it indicated that no heterogeneity was present. Low, medium, and high degrees of heterogeneity were defined by I^2^ values of 25, 50, and 75%, respectively (24). When p > 0.1 and I^2^ < 50%, heterogeneity was considered low, and the fixed effects model was used for analysis. If I^2^ > 50%, significant heterogeneity was present, and the random effects model was applied for the combined analysis.
Second, network meta-analysis was performed using STATA 16.0, with data analyzed under the frequentist framework (25). In the network plot, each node represents an intervention, and the line connecting any two nodes indicates direct comparisons between these interventions. The width of each line corresponds to the number of studies comparing the two interventions. Multiple closed loops are formed among interventions. Overall inconsistency was evaluated using the inconsistency factor (IF) and its 95% confidence interval (95%CI), while local inconsistency was detected using the node-splitting method. Local inconsistency was considered to exist when p < 0.05. Various intervention types were ranked based on cumulative probabilities derived from the surface under the cumulative ranking curve (SUCRA). SUCRA values range from 0 to 1, with higher values indicating a greater likelihood of being the most effective intervention (26).
Results
3
Search results
3.1
The literature screening process and results are shown in Figure 1. Initially, we identified a total of 2015 studies. After eliminating duplicates in articles, titles, and abstracts, we selected 178 full-text articles for detailed review. Finally, 15 studies were included in the network meta-analysis.
Flowchart of all studies identified, included, and excluded following the PRISMA 2020 statement.
Characteristics of the included studies
3.2
The characteristics of the included RCTs were summarized in Table 1. A total of 15 RCTs, involving 903 patients from nine countries, were included, and five different time points of enteral feeding in critically ill patients were considered.
Risk of bias and grade of evidence
3.3
Using the ROB 2.0 tool, we assessed the risk of bias as follows: 20% of studies were rated as high risk, 53.3% had some concerns, and 26.7% were considered low risk. The randomization process was generally well conducted, with 60% of studies rated as low risk. However, concerns remained for 40% of studies, primarily due to insufficient details on allocation concealment. Issues related to deviations from the intended interventions were noted, with 13.3% of studies rated as high risk—mainly because blinding of researchers or participants was not implemented, potentially leading to performance bias. Regarding outcome measurement bias, 20% of studies were rated as high risk, largely because it was unclear whether outcome assessors were aware of the interventions received by the participants, as illustrated in Figure 2. The results of the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) are presented in Appendix Table 2.
Assessment of the risk of bias summary.
Traditional pairwise meta-analysis
3.4
The results of the traditional pairwise meta-analysis are shown in Figures 3A,B.
(A) Traditional pairwise meta-analysis of mortality rate. (B) Traditional pairwise meta-analysis of length of ICU stay.
A total of 15 studies were included in this systematic review, 11 of which assessed the impact of different enteral feeding timings on mortality in critically ill patients. The meta-analysis of these 11 studies, comprising 357 participants in the treatment group and 351 in the control group, revealed a risk ratio of 0.80 (95% CI: 0.59, 1.08; I^2^ = 7%; p = 0.14). Given the low heterogeneity observed in this outcome, all eligible studies were then included in the network meta-analysis for further comparative analyses. Additionally, 12 studies reported the effects of different enteral feeding timings on ICU length of stay for critically ill patients. The meta-analysis of these studies, which included 323 participants in the treatment group and 317 in the control group, showed a mean difference of 0.74 (95%CI: −1.08, 2.55; I^2^ = 84%; p = 0.43).
Sensitivity analysis revealed that after excluding Study 9 (27), the heterogeneity decreased to I^2^ = 55%. Quality assessment using the ROB 2.0 tool indicated that this study was at high risk of bias, suggesting it might be the primary source of heterogeneity. Consequently, we excluded this study and incorporated the remaining qualified studies into the final network meta-analysis.
Network meta-analysis
3.5
Network plots
3.5.1
The network plot illustrates the network structure and the number of studies on interrelationship among different enteral feeding timing. The most common enteral feeding timing was A, while the least frequent was D. A total of 15 studies reported on various timings of enteral feeding in critically ill patients, involving five intervention times, which collectively formed eight triangular closed loops, as shown in Figures 4I,II.
(I,II) Network plot of outcome indicators. (I) Mortality rate; (II) Length of ICU stay; A: <24 h; B: 24–48 h; C: 48–72 h; D: 72–96 h; E: >96 h.
Basic hypothesis testing
3.5.2
Loop inconsistency tests, inconsistency models, and node splitting methods were employed to examine the inconsistency of each outcome indicator. A consistency inspection showed that most p > 0.05, indicating good agreement and no significant overall inconsistency, as shown in Appendix 2.
Effect on mortality rate
3.5.3
Pairwise comparisons evaluating the impact of different enteral feeding timings on the primary outcome (mortality) in critically ill patients are presented in Figure 5. Results indicated no statistically significant differences in mortality between the following enteral feeding timings: <24 h vs. 24–48 h; 24–48 h vs. 48–72 h; 48–72 h vs. 72–96 h; 72–96 h vs. > 96 h; and <24 h vs. > 96 h. The respective results were: (RR = 1.20, 95%CI: 0.59, 2.45), (RR = 0.88, 95%CI: 0.31, 2.50), (RR = 0.94, 95%CI: 0.13, 6.99), (RR = 0.81, 95%CI: 0.12, 5.44), and (RR = 1.00, 95%CI: 0.16, 6.38).
(A) Revised. Network meta-analysis results of different intestinal nutrition timing on mortality in critically ill patients [RR (95% CI)]. A: <24 h; B: 24–48 h; C: 48–72 h; D: 72–96 h; E: >96 h. (B) Revised. Network meta-analysis results of different enteral nutrition timing on the length of hospital stay for critically ill patients [MD (95% CI)]. A: <24 h; B: 24–48 h; C: 48–72 h; D: 72–96 h; E: >96 h.
Effect on ICU length of stay
3.5.4
Pairwise comparisons evaluating the impact of different enteral feeding timings on the primary outcome (ICU length of stay) in critically ill patients are presented in Figure 5. Results indicated no statistically significant differences on ICU length of stay between the following enteral feeding timings: <24 h vs. 24–48 h; 24–48 h vs. 48–72 h; 48–72 h vs. 72–96 h; 72–96 h vs. >96 h; and <24 h vs. >96 h. The respective results were: (MD = −1.69, 95%CI: −4.69, 1.31); (MD = 1.99, 95%CI: −2.07, 6.05); (MD = 1.60, 95%CI: −4.04, 7.60); (MD = −0.37, 95%CI: −6.39, 5.66); (MD = 1.90, 95%CI: −3.44, 7.24).
Analysis using the Surface Under the Cumulative Ranking Curve (SUCRA) revealed distinct population-specific trends and ranking probabilities. For mortality outcomes, the SUCRA values for the five EN initiation timings were as follows: <24 h (SUCRA = 51.7%), 24–48 h (SUCRA = 67.0%), 48–72 h (SUCRA = 55.4%), 72–96 h (SUCRA = 49.8%), and >96 h (SUCRA = 26.1%). For ICU length of stay, the SUCRA values were: <24 h (SUCRA = 41.3%), 24–48 h (SUCRA = 12.3%), 48–72 h (SUCRA = 49.4%), 72–96 h (SUCRA = 71.8%), and >96 h (SUCRA = 75.2%).
Publication bias analysis
3.6
A funnel plot was generated to assess publication bias for the mortality outcome. The results showed that study points were approximately symmetrically distributed on both sides of the central axis, suggesting a low likelihood of publication bias, as shown in Figure 6.
Funnel plot for mortality rate.
A funnel plot was generated to assess publication bias for the ICU length of stay. The results showed that study points were approximately symmetrically distributed on both sides of the central axis, suggesting a low likelihood of publication bias, as shown in Figure 7.
Funnel plot for the length of ICU stay.
Discussion
4
This study found no statistically significant differences in mortality or ICU length of stay across the five EN initiation timings in critically ill patients (all p > 0.05). However, SUCRA rankings revealed notable population-specific trends: initiating EN within 24–48 h may reduce mortality in certain patient subgroups, while delaying EN initiation beyond 96 h might shorten ICU length of stay in some populations.
The advantage of initiating EN within 24–48 h stems from the dual mechanisms of “stress regulation and gut protection.” Animal studies have demonstrated that guinea pigs with experimental burns who were fed within 2 h of injury exhibited significantly lower 24 h urinary vanillylmandelic acid excretion levels compared to those with delayed feeding at 72 h. This biomarker difference directly indicates that early feeding can suppress the overactivation of the sympathetic-adrenal medullary system, reduce catecholamine secretion, and thereby alleviate the prolonged hypermetabolic stress state post-trauma, preventing metabolic disturbances and immune dysregulation (28). This mechanism has been indirectly validated in human trauma patients. Clinical studies have shown that patients who initiated EN within 24–48 h after trauma had significantly lower serum catecholamine levels and a 30% reduction in the incidence of immune dysregulation compared to the delayed feeding group (29).
A mechanistic study on SAP (severe acute pancreatitis) rats demonstrated that early EN significantly upregulated the expression of mucosal address in cell adhesion molecule-1 (MAdCAM-1) in the intestinal mucosa and increased the infiltration of CD4^+^ and CD8^+^ T cells. This change directly alleviated pathological intestinal damage in SAP rats, reduced serum endotoxin levels and bacterial translocation, and ultimately correlated with decreased mortality (30). This mechanism is also applicable to human SAP patients: clinical studies have shown that SAP patients who initiated EN within 48 h of onset had significantly lower rates of enterogenous infections and a reduced incidence of multiple organ dysfunction syndrome (MODS) compared to the delayed feeding group (31). This supports the mortality benefit of initiating EN within 24–48 h for SAP patients, which is fully consistent with the SUCRA trend of reduced mortality in the 24–48 h group in this study. The potential advantages of initiating EN within 24–48 h primarily manifest in hemodynamic stability, relatively normal gastrointestinal function, and the capacity to reduce mortality by protecting the intestinal barrier and suppressing stress responses.
The advantage of initiating EN beyond 96 h lies in avoiding aspiration pneumonia, shortening the infection control cycle, and reducing feeding-related complications. For cerebral malaria patients in resource-limited settings who cannot undergo endotracheal intubation and remain comatose within the first 24 h of admission, the core risk of initiating EN is “aspiration leading to aspiration pneumonia.” From a pathophysiological perspective, in a state of deep coma, the swallowing reflex is impaired, and the lower esophageal sphincter tone is reduced. Early EN can cause gastric retention, and vomiting without airway protection may result in the aspiration of gastric contents into the lungs, triggering aspiration pneumonia. Such complications can prolong the infection control period and the duration of mechanical ventilation dependence, ultimately extending ICU length of stay (32).
For septic shock patients requiring high-dose vasopressors, the risk of early EN lies in “insufficient gastrointestinal perfusion leading to intestinal ischemia and feeding intolerance,” while delaying EN beyond 96 h significantly reduces this risk. The core pathophysiological mechanism is that in shock, the body prioritizes blood supply to the heart and brain, leaving the gastrointestinal mucosa in a state of “relative ischemia.” Early EN increases intestinal oxygen demand, exacerbates mucosal ischemic injury, and may even induce non-occlusive intestinal ischemia. Additionally, high stress inhibits gastrointestinal motility, resulting in an EN retention rate of over 40%, which can lead to gastric retention, intestinal distension, and increased risk of enterogenic infections. By delaying EN until beyond 96 h, when the patient’s circulatory status stabilizes and gastrointestinal perfusion improves, the rate of feeding intolerance decreases from 42% in the early group to 18%, and the incidence of enterogenous infections drops from 25 to 10% (33). This significantly avoids prolonged ICU stays due to nutrition-related complications, further supporting the benefit of initiating EN beyond 96 h for septic shock patients in reducing ICU length of stay. The potential advantage of initiating EN beyond 96 h lies in delaying to avoid complications such as aspiration and intestinal ischemia, with nutritional support initiated only after the patient’s physiological condition stabilizes, thereby shortening ICU hospitalization time.
The optimal timing for initiating EN in critically ill patients remains a contentious issue in clinical practice. This controversy has led to conflicting recommendations in clinical guidelines (e.g., some guidelines suggest initiating EN within 24–48 h after achieving hemodynamic stability, while others recommend delaying until after the acute phase). Such inconsistencies directly result in a lack of standardized clinical decision-making, potentially compromising the efficacy and safety of nutritional support in critically ill patients (34). Some researchers argue that early initiation of EN can protect intestinal mucosal barrier function, modulate immune-metabolic homeostasis, and thereby reduce infection risks and improve patient outcomes. Conversely, proponents of delayed EN initiation emphasize that critically ill patients may experience gastrointestinal dysfunction and hemodynamic instability during the acute phase, initiating EN too early could thus increase the risk of complications such as aspiration, diarrhea, or intestinal ischemic injury. This controversy not only reflects differing understandings of the pathophysiological state of critically ill patients but also exacerbates inconsistencies in clinical practice and guideline recommendations. Our network meta-analysis aims to reveal, potential trends and provides new evidence-based perspectives on this debate, while further highlighting the complexity of the conflict.
This study addresses the “early vs. delayed” controversy by systematically comparing the effects of different EN initiation timings via network meta-analysis and revealing potential stratified benefits. However, the credibility of the pooled effect sizes across studies may be limited due to several limitations. First, inadequately described allocation concealment may have introduced selection bias, leading to imbalances in baseline characteristics between groups. Second, the absence of blinding in outcome assessment might have amplified between-group differences due to subjective judgments. These factors collectively reduce the reliability of the combined effect estimates. Additionally, significant heterogeneity in the definitions of “early” and “delayed” across studies—for example, some studies define “early” as <24 h, which differs from the 24–48 h early window proposed in this study—directly increased statistical heterogeneity during evidence synthesis and reduced comparability between studies.
To resolve the “early vs. delayed” controversy and improve the quality of evidence, future research should focus on addressing the following key issues: First, multicenter, large-sample randomized controlled trials (RCTs) should be conducted, providing higher-level evidence through unified study designs and rigorous quality control. Second, collaboration with authoritative institutions is needed to standardize the definitions of EN initiation timings, clarifying criteria for “early” (e.g., within 24–48 h, hemodynamic stability) and “delayed” (e.g., beyond 96 h, high-risk populations) to reduce heterogeneity. Ultimately, these efforts will enable more precise decision-making in nutritional support for critically ill patients.
Limitations
5
First, methodological transparency was insufficient across most included trials, particularly regarding allocation concealment (a key determinant of randomization integrity) and blinding of participants, providers, or outcome assessors. These gaps led to an “unclear risk of bias” rating for critical methodological domains, which may introduce imprecision into effect estimates and downgrade evidence certainty per the GRADE framework. Secondly, due to the limited number of included studies and the lack of disease-specific stratification of critically ill patients, this study could only rely on pooled data analysis. This approach prevented a thorough exploration of potential heterogeneity and its impact on the results, thereby limiting the precision of the conclusions and their generalizability to specific clinical subpopulations. Future research should prioritize disease-stratified studies and explore potential treatment effect modifiers to optimize personalized clinical guidance.
Conclusion
6
This study provides valuable insights for determining the optimal timing of EN initiation in critically ill patients. EN started within 24–48 h of ICU admission was most effective in reducing mortality. EN initiated after 96 h shortened ICU stays but had low evidence quality and is not recommended. Healthcare providers should integrate patient-specific factors into EN timing decisions, rather than relying solely on evidence-based guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elke G Hartl WH Kreymann KG Adolph M Felbinger TW Graf T . Clinical nutrition in critical care medicine - guideline of the German Society for Nutritional Medicine (DGEM). Clin Nutr ESPEN. (2019) 33:220–75. doi: 10.1016/j.clnesp.2019.05.002, 31451265 · doi ↗ · pubmed ↗
- 2Vincent JL Marshall JC Namendys-Silva SA François B Martin-Loeches I Lipman J . Assessment of the worldwide burden of critical illness: the intensive care over nations (ICON) audit. Lancet Respir Med. (2014) 2:380–6. doi: 10.1016/S 2213-2600(14)70061-X, 24740011 · doi ↗ · pubmed ↗
- 3Wu J Lu AD Zhang LP Zuo YX Jia YP. Study of clinical outcome and prognosis in pediatric core binding factor-acute myeloid leukemia. Zhonghua Xue Ye Xue Za Zhi. (2019) 40:52–7. doi: 10.3760/cma.j.issn.0253-2727.2019.01.01030704229 PMC 7351698 · doi ↗ · pubmed ↗
- 4Mc Clave SA Martindale RG Vanek VW Mc Carthy M Roberts P Taylor B . Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine (SCCM) and American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.). JPEN J Parenter Enteral Nutr. (2009) 33:277–316. doi: 10.1177/0148607109335234, 19398613 · doi ↗ · pubmed ↗
- 5Cardenas D Bermúdez C Pérez A Diaz G Cortes LY Contreras CP . Nutritional risk is associated with an increase of in-hospital mortality and a reduction of being discharged home: results of the 2009-2015 nutrition Day survey. Clin Nutr ESPEN. (2020) 38:138–45. doi: 10.1016/j.clnesp.2020.05.014, 32690148 · doi ↗ · pubmed ↗
- 6Lee MJ Sayers AE Drake TM Singh P Bradburn M Wilson TR . Malnutrition, nutritional interventions and clinical outcomes of patients with acute small bowel obstruction: results from a national, multicentre, prospective audit. BMJ Open. (2019) 9:e 029235. doi: 10.1136/bmjopen-2019-029235, 31352419 PMC 6661661 · doi ↗ · pubmed ↗
- 7Inciong JFB Chaudhary A Hsu HS Joshi R Seo JM Trung LV . Economic burden of hospital malnutrition: a cost-of-illness model. Clin Nutr ESPEN. (2022) 48:342–50. doi: 10.1016/j.clnesp.2022.01.020, 35331511 · doi ↗ · pubmed ↗
- 8Gostyńska A Stawny M Dettlaff K Jelińska A. Clinical nutrition of critically ill patients in the context of the latest ESPEN guidelines. Med Kaunas. (2019) 55:770. doi: 10.3390/medicina 55120770, 31810303 PMC 6955661 · doi ↗ · pubmed ↗