Successful Treatment of Paranasal Sinus Metastasis From Renal Cell Carcinoma With Immune Checkpoint Inhibitors and Radiotherapy: A Case Report
Shota Yamada, Tomohiro Matsuo, Ayaka Tsuchiyama, Hiromi Nakanishi, Kensuke Mitsunari, Kojiro Ohba, Yasushi Mochizuki, Ryoichi Imamura

TL;DR
A rare case of kidney cancer spreading to the sphenoid sinus was successfully treated with radiation and immunotherapy drugs.
Contribution
This case report presents a successful treatment approach for a rare and challenging RCC metastasis using radiation and immune checkpoint inhibitors.
Findings
The patient showed a partial response to radiation therapy followed by immunotherapy with nivolumab and ipilimumab.
Blindness caused by the tumor improved during treatment, and tumor reduction was sustained over 37 cycles of maintenance therapy.
Abstract
Renal cell carcinoma (RCC) metastasis to the paranasal sinuses is rare and lacks standard treatment, particularly for unresectable tumors. We report a case of sphenoid sinus metastasis with sarcomatoid differentiation successfully managed with radiation therapy and immunotherapy. A 59‐year‐old male who had undergone left radical nephrectomy for RCC 13 years prior presented with acute left eye pain and tinnitus. Contrast‐enhanced computed tomography (CT) revealed a hyper vascular sphenoid sinus mass with osseous destruction. Biopsy confirmed metastatic RCC with sarcomatoid differentiation. Given rapid symptom progression, intensity‐modulated radiation therapy (39 Gy in 13 fractions) was initiated, followed by immunotherapy with nivolumab and ipilimumab. The patient developed complete blindness, which gradually improved during treatment. Serial CT showed a partial response sustained…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
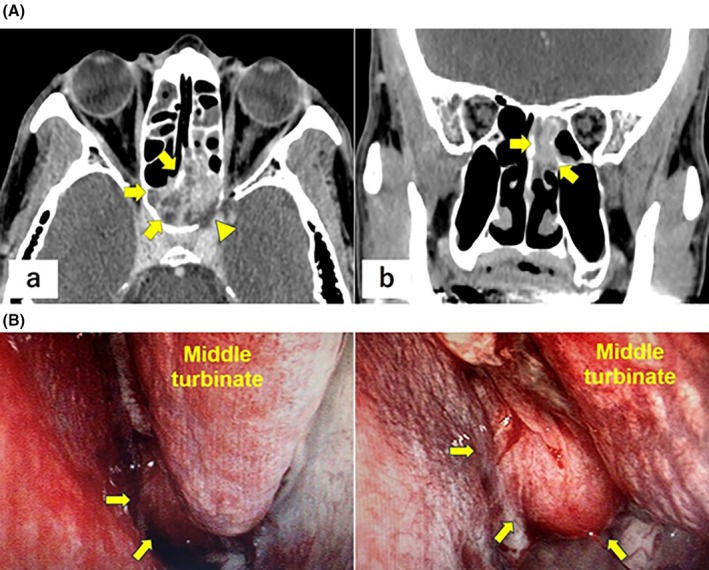 FIGURE 1
FIGURE 1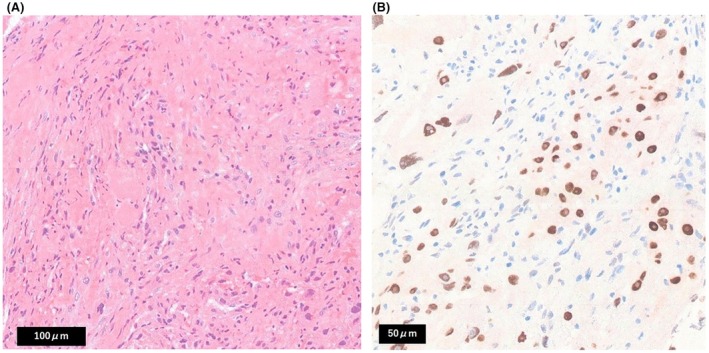 FIGURE 2
FIGURE 2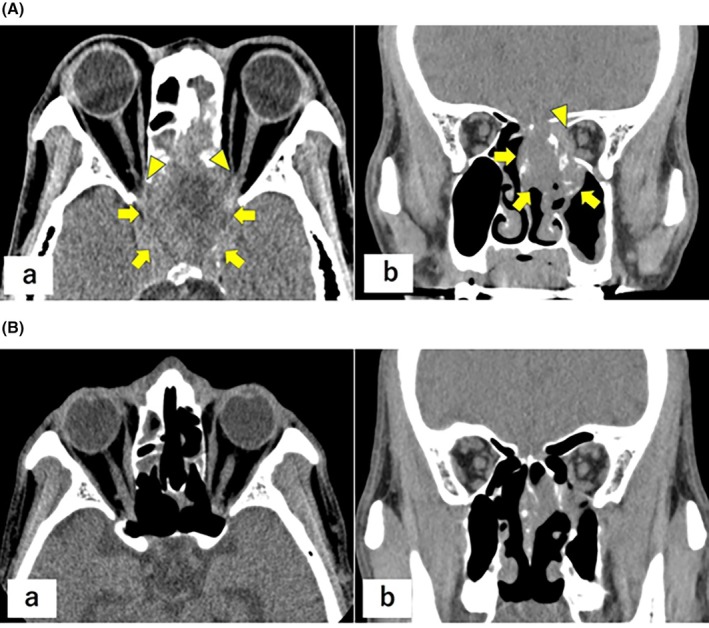 FIGURE 3
FIGURE 3|
| Authors, references | Age/Sex | Time since nephrectomy | Metastatic cites | Systemic therapy | Radiation therapy | Best response | Outcome/follow up |
|---|---|---|---|---|---|---|---|---|
| 1 | Present case | 59/M | 13 y | Sphenoid sinus | Nivolmab + Ipilimumab | Yes (39 Gy/13 fr) | PR | Alive at 42 months |
| 2 | Hess AO et al. [ | 73/M | 3 y | Nasal cavity, Ethmoid sinus, Sphenoid sinus, Brain, Adrenal gland | Pembrolizumab | Yes (20 Gy/1 fr) | SD | Alive at 5 months |
| 3 | Arai Y et al. [ | 73/M | 2 y | Ethmoid sinus | Axitinib | No | PR | Alive at 31 months |
| 4 | Parida PK et al. [ | 65/M | 15 y | Frontal sinus, Ethmoid sinus, contralateral kidney | Interferon | No | SD | Alive at 2 months |
| 5 | Parida PK et al. [ | 58/M | 10 y | Ethmoid sinus, Sphenoid sinus, contralateral kidney | Interferon | Yes | SD | Alive at 4 months |
| 6 | Parida PK et al. [ | 40/F | 12 y | Frontal sinus, Ethmoid sinus, contralateral kidney | Interferon | Yes | SD | Alive at 6 months |
| 7 | Marchand‐Crety C et al. [ | 75/M | 9 m | Sphenoid sinus | Sunitinib | Yes (27 Gy/3 fr) | CR | Alive at 5 months |
| 8 | Sawazaki H et al. [ | 58/M | 11 y | Maxillary sinus, contralateral kidney | Interferon | Yes (45 Gy/18 fr) | SD | Alive at 3 months |
| 9 | Ranjan SK et al. [ | 74/F | 0 m | Frontal sinus, Ethmoid sinus | Pazopanib | No | PR | Alive at 6 months |
| 10 | Singh J et al. [ | 48/M | 0 m | Nasal cavity | Sunitinib | No | SD | Alive at 3 months |
| 11 | Kumar R et al. [ | 42/M | 10 y | Frontal sinus, lung | Sunitinib | Yes | SD | Alive at 1 month |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Diagnosis and Treatment · Metastasis and carcinoma case studies · Renal cell carcinoma treatment
Introduction
1
Renal cell carcinoma (RCC) metastasis to the paranasal sinuses is very rare [1]. However, unresectable tumors present substantial therapeutic challenges. Moreover, although systemic therapy has improved over the past decade, with targeted agents and immune checkpoint inhibitors (ICIs) now central to care, the optimal approach for paranasal sinus lesions remains uncertain, especially when rapid symptoms threaten vision or cranial nerves. We report a case of sphenoid sinus metastasis that responded to radiotherapy combined with ICI therapy.
Case Presentation
2
A 59‐year‐old male patient presented with acute‐onset left eye pain and tinnitus. The medical history included hypertension and a left laparoscopic radical nephrectomy for clear cell RCC (pT1bN0M0, G3 < G2, INFα, v0) 13 years earlier. Routine non‐contrast chest/abdominal computed tomography (CT) showed no recurrence, whereas contrast‐enhanced head CT revealed an approximately 4‐cm hyper vascular mass centered in the sphenoid sinus with osseous destruction of the sella turcica and clivus (Figure 1A). [Correction added on 20 March 2026, after first online publication: Figure 1B was deleted in the preceding sentence.] An endoscopic transnasal biopsy was performed (Figure 1B); however, the symptoms rapidly worsened, necessitating urgent admission. [Correction added on 20 March 2026, after first online publication: Figure 1B was added in the preceding sentence.] Repeat CT showed progressive sphenoid destruction and invasion of the left optic canal. Histopathological examination confirmed the presence of metastatic RCC with sarcomatoid differentiation. (Figure 2A). [Correction added on 20 March 2026, after first online publication: Figure 2A has been added in the preceding sentence.] Immunohistochemistry showed Paired box gene 8 (PAX8) positivity, supporting the diagnosis of metastatic renal cell carcinoma (Figure 2). [Correction added on 20 March 2026, after first online publication: The preceding sentence has been added.]
Contrast‐enhanced head computed tomography images at presentation demonstrating an approximately 4‐cm hyper vascular mass centered in the sphenoid sinus with osseous destruction involving the sellar floor and clivus. (A) Axial image. (B) Coronal image. Arrows: Tumors; arrowheads: Osseous destruction. (B) Nasal endoscopic view demonstrating a tumor located posterior to the left middle turbinate. Arrows: tumors. [Correction added on 20 March 2026, after first online publication: Figure 1 and its caption have been corrected to show previously missing bottom panels.]
Intensity‐modulated radiotherapy (IMRT; 39 Gy in 13 fractions) was administered. Upon completion, the patient's visual acuity had declined to light perception only. Given the ongoing deterioration and poor International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) risk (Karnofsky 40%, thrombocytosis 429 × 10^3^/μL, corrected calcium 10.6 mg/dL), nivolumab (240 mg flat dose) and ipilimumab (1 mg/kg) were initiated. On day 3 of treatment, vision showed no light perception, with CT showing evidence of bilateral optic nerve invasion (Figure 3A). [Correction added on 20 March 2026, after first online publication: ‘Figure 2A,B’ has been corrected to ‘Figure 3A’ in the preceding sentence.] From day 20, visual function gradually improved. Visual acuity in the right eye recovered to a level sufficient for independent ambulation, while vision in the left eye returned to light perception. [Correction added on 20 March 2026, after first online publication: The preceding sentence has been added.] Follow‐up CT showed no further growth. The patient was discharged after the second cycle of treatment. CT in the second and fourth cycles revealed tumor reduction (Figure 3B), consistent with a partial response. [Correction added on 20 March 2026, after first online publication: ‘Figure 3A,B’ has been corrected to Figure 3B in the preceding sentence.] After four cycles of nivolumab plus ipilimumab, the patient was transitioned to maintenance nivolumab and completed 37 cycles. The partial response has been maintained, and the patient remains alive 3.5 years after treatment initiation.
(A) Hematoxylin and eosin–stained section shows atypical spindle to pleomorphic tumor cells with marked nuclear atypia, consistent with sarcomatoid features. (B) Immunohistochemical staining demonstrates Paired box gene 8 (PAX8) positivity, supporting the diagnosis of metastatic renal cell carcinoma derived from clear cell renal cell carcinoma. [Correction added on 20 March 2026, after first online publication: Figure 2 and its caption have been corrected.]
Non‐contrast head computed tomography images showing interval enlargement of the sphenoid sinus tumor with involvement of both optic canals, consistent with optic pathway compromise. (a) Axial image. (b) Coronal image. Arrows: tumor; arrowheads: optic canals. Non‐contrast head computed tomography images during follow‐up demonstrating interval shrinkage of the sphenoid sinus lesion after radiotherapy and immunotherapy, consistent with a partial response. (a) Axial image. (b) Coronal image. [Correction added on 20 March 2026, after first online publication: Figure 3 and its caption have been corrected.]
Discussion
3
Metastatic RCC involving the paranasal sinuses is rare. Metastases occur in the head and neck in approximately 3.3% of cases, with the paranasal sinuses, larynx, and mandible being the most frequent subsites [1, 2]. Potential routes of spread include Batson's valveless vertebral venous plexus, which may permit craniofacial seeding while bypassing pulmonary filtration [3]. Because late recurrence beyond 5 years occurs in approximately 8%–10% of cases, prolonged surveillance remains relevant even after long disease‐free intervals [4, 5]. In our case, a 59‐year‐old male developed a hyper vascular sphenoid sinus mass 13 years after nephrectomy, presenting with acute ocular pain and rapid visual decline, consistent with the anatomic vulnerability of the sphenoid sinus and the adjacent optic apparatus. To contextualize clinical features, treatments, and outcomes in the literature, we summarized previously reported cases (Table 1).
Epistaxis is the most common presentation, whereas headache, diplopia, and nasal obstruction can also occur depending on the tumor location [2, 13]. Our patient mainly reported ocular pain and tinnitus. Imaging confirmed left optic canal invasion, underscoring the propensity for vision‐threatening progression of sphenoid disease. Diagnosis requires histopathology; in this case, biopsy confirmed metastatic RCC with sarcomatoid differentiation, highlighting the aggressive biology that can drive rapid neurologic compromise and necessitate expedited decision‐making.
When resectable, surgery provides local control. One review reported complete control in 17 of 22 operated cases (77%) [13]. For disseminated or unresectable diseases, care is typically limited to diagnostic biopsy with meticulous attention to bleeding risk, given tumor hypervascularity. Blood loss > 500 mL during sinonasal biopsy has been reported; thus, preoperative embolization may mitigate intraoperative hemorrhage [2, 13]. Our case was deemed unresectable because of skull base invasion and poor risk profile by IMDC, which guided a nonoperative strategy prioritizing urgent local control and early systemic therapy.
Over the past two decades, treatment has shifted from interferon‐based regimens to tyrosine kinase inhibitors, and more recently, ICIs, with case‐level responses to axitinib and a broader adoption of ICIs in metastatic protocols [2, 6, 7]. Radiotherapy, including stereotactic body radiotherapy for sphenoid diseases, is frequently integrated for local control, with favorable responses reported [2, 7, 8, 9]. We administered IMRT (39 Gy in 13 fractions) to the sphenoid lesions. Although vision had declined to no light perception by completion, visual function began to improve on treatment day 20 after initiating nivolumab plus ipilimumab. Serial CT after cycles 2 and 4 demonstrated measurable tumor reduction, consistent with a partial response (Figure 3). These observations parallel reports of sequential modern systemic therapy and focal radiotherapy to balance rapid symptom control with systemic disease management [2, 6, 7, 8, 9, 10, 11, 12]. Our timeline suggests that rapid local debulking with radiotherapy can stabilize the anatomical risk while systemic therapy is mobilized, an approach that may be especially valuable when optic pathway compromise is imminent.
Given the proximity of the paranasal sinuses to the orbits and skull base, progression commonly causes visual impairment and pain, which impacts patient quality of life. Therefore, radiotherapy is a rational adjunct to systemic therapy for unresectable presentations [2, 8, 13]. The emergence of ICIs has renewed interest in their potential abscopal effect, wherein local irradiation augments systemic antitumor immunity [14, 15]. In our patient, the sequence of local radiotherapy followed by ICIs and subsequent systemic radiological improvement paralleled a recent RCC report consistent with the abscopal phenomenon [16]. Although such responses are uncommon, converging evidence indicates that they can occur with ICI exposure and may be potentiated by radiotherapy [14, 15]. Accordingly, our experience supports the careful integration of radiotherapy with systemic immunotherapy, with individualized treatment based on resectability, overall disease burden, anticipated bleeding risk, and urgency to preserve vision or neurological function. In our case, multidisciplinary management led to improved quality of life and comparatively long survival (3.5 years since treatment initiation). Therefore, continuous therapy with regular and careful follow‐up is warranted.
Conclusion
4
This case highlights the potential benefits of integrating radiotherapy with ICIs for unresectable sphenoid sinus metastases from RCC. Because this condition is rare, further accumulation of cases is warranted.
Consent
Written informed consent was obtained.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Lieder , T. Guenzel , S. Lebentrau , C. Schneider , and A. Franzen , “Diagnostic Relevance of Metastatic Renal Cell Carcinoma in the Head and Neck: Evaluation of 22 Cases Among 671 Patients,” International Brazilian Journal of Urology 43 (2017): 202–208, 10.1590/S 1677-5538.IBJU.2015.0665.27649110 PMC 5433357 · doi ↗ · pubmed ↗
- 2A. O. Hess , R. S. Terry , B. C. Lobo , and J. M. Justice , “Sinonasal and skull base metastatic renal cell carcinoma: a case series,” Cureus 15 (2023): e 48757, 10.7759/cureus.48757.38094536 PMC 10719062 · doi ↗ · pubmed ↗
- 3M. D. Gottlieb and J. T. Roland, Jr. , “Paradoxical Spread of Renal Cell Carcinoma to the Head and Neck,” Laryngoscope 108 (1998): 1301–1305, 10.1097/00005537-199809000-00007.9738745 · doi ↗ · pubmed ↗
- 4Y. H. Park , C. Lee , J. H. Kim , et al., “Late Recurrence of Renal Cell Carcinoma > 5 Years After Surgery: Clinicopathological Characteristics and Prognosis,” BJU International 110, no. 11 Pt B (2012): E 553–E 558, 10.1111/j.1464-410X.2012.11246.x.22578274 · doi ↗ · pubmed ↗
- 5S. H. Lee , J. K. Kim , J. Park , et al., “Which Patients Should We Follow Up Beyond 5 Years After Definitive Therapy for Localized Renal Cell Carcinoma?,” Cancer Research and Treatment: Official Journal of Korean Cancer Association 46 (2014): 374–381, 10.4143/crt.2014.013. · doi ↗
- 6Y. Arai , K. Ito , K. Tachi , et al., “Metastatic Renal Cell Carcinoma in the Paranasal Sinus Effectively Managed With a Periodic Axitinib Withdrawal Schedule: A Case Report,” Hinyokika Kiyo 62 (2016): 465–471, 10.14989/Acta Urol Jap_62_9_465.27760971 · doi ↗ · pubmed ↗
- 7P. K. Parida , “Renal Cell Carcinoma Metastatic to the Sinonasal Region: Three Case Reports With a Review of the Literature,” Ear, Nose, & Throat Journal 91 (2012): E 11–E 16, 10.1177/014556131209101113. · doi ↗
- 8C. Marchand‐Crety , E. Vigneau , and C. Invernizzi , “Stereotactic Body Radiotherapy of a Solitary Metachronous Sphenoid Metastasis From Renal Cell Carcinoma: A Case Report,” Case Reports in Oncology 14 (2021): 269–273, 10.1159/000514950.33776715 PMC 7983564 · doi ↗ · pubmed ↗