Prevalence and associated factors of skin disease among school-age children of rural district of eastern zone of Tigray, Ethiopia, 2024
Mulugeta Abraha Gebregiorgis, Almaz Berhe, Haftom Gebrehiwot, Mamush Gidey Abrha, Binyam Gebrehiwet Tesfay, Fiseha Abadi Gebreanenia, Binyam Tsegay Hagos, Willi Bahre, Guesh Teklu Woldemariam, Mearg Alemu Halefom, Tesfay Gebreslassie Gebrehiwot, Dawit Getachew Gebeyehu

TL;DR
This study found a high rate of skin diseases among school-age children in rural Ethiopia and identified factors like poor hygiene and sharing personal items as contributors.
Contribution
The study provides new prevalence data and identifies specific risk factors for skin diseases in postwar rural Ethiopia.
Findings
The prevalence of skin disease among school-age children was 68.2% in the study area.
Factors like living in IDP and poor hand hygiene were strongly associated with skin diseases.
Sharing personal items and family history of skin disease significantly increased risk.
Abstract
Skin diseases are conditions that affect the skin. Skin diseases encompass various conditions, including infections, allergies, inflammatory disorders, and infestation. Skin diseases are a significant public health concern, particularly among school-age children, as they can cause discomfort, and social stigma, and influence overall well-being. There is limited research conducted specifically among school-age children, especially in the postwar period, hindering the understanding of the extent of the problem and the identification of potential contributing factors. In Ethiopia, a study conducted on primary schoolchildren shows that the prevalence of skin diseases was 61.2%. A school-based cross-sectional study was employed from September 10 to October 30, 2024, in selected schools of Eastern Tigray. A multi-stage sampling technique was used to choose Woredas and schools. Subsequently,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
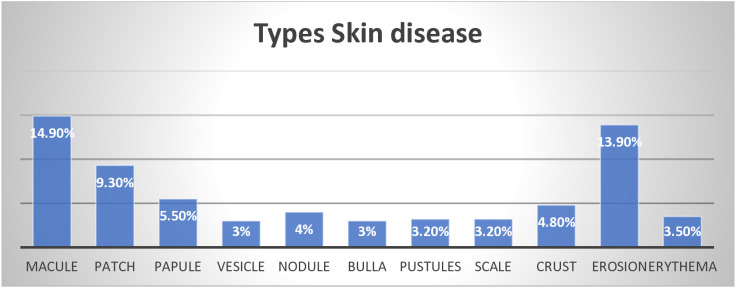 Fig 1
Fig 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatological diseases and infestations · Neonatal skin health care · Nail Diseases and Treatments
Introduction
Skin diseases are conditions that affect the skin. These diseases may cause rashes, inflammation, itchiness or other skin changes. Some skin conditions may be genetic, while lifestyle factors may cause others. Skin disease treatment may include medications, creams, ointments, or lifestyle changes [1,2].
Skin conditions incorporate various disorders, including infectious diseases, allergic reactions, inflammatory problems, and infestations [1]. These skin issues can manifest with varying degrees of severity, from minor irritations to chronic and disabling conditions. School-age children are especially susceptible to developing skin diseases due to their maturing immune systems, close interactions within the school setting, and participation in outdoor activities [1,2].
Skin and subcutaneous diseases were responsible for 41.6 million Disability Adjusted Life Years (DALYs) and 39.0 million years lost due to Disability (YLDs) which makes them the 18th leading cause of global DALYs. Excluding mortality, skin diseases were the fourth leading cause of disability worldwide [3].
Dermatological conditions are a common problem in school-age children. Contact between classmates is an important cause of skin infections and infestations. The occurrence and pattern of skin diseases have been seen to vary depending on the socio-economic and cultural factors related to hygiene and treatment-seeking behavior. Skin diseases cause discomfort, and social stigma, and impact overall well-being [4,5].
Dermal issues are one of the most important health matters with significant impacts on school-aged children and cause nonfatal disabilities worldwide, particularly in low-resource regions [6].
Skin-related ailments affect people of all ages, yet children are one of the most common victims of it [3]. Skin diseases represent an important part of the morbidity among children and are possibly influenced by, social, and economic factors [7].
Understanding the prevalence and potential factors associated with the occurrence of skin diseases is crucial for effective prevention and management strategies [8]. The most epidemiologically important seems to be the infectious types because of their transmissibility and amenability to simple school-health measures [9].
It is increasingly recognized that schools play an important role in coaching healthy and hygienic habits among the younger generations, by take-home messages, which create awareness among the children, parents, or guardians on healthy living. [4].
The Rural District of Eastern Zone in the Tigray Region of Ethiopia has distinct environmental, cultural, and socioeconomic factors that may affect the prevalence and risk factors associated with skin diseases among school-age children in the area. The Tigray Region has experienced conflict, resulting in many displaced and orphaned children in the local population. However, there is limited research that has specifically focused on this particular post-conflict population, hindering the understanding of the extent of skin disease issues and the identification of potential contributing factors in this community [10].
Methods and materials
Study design, population, area and period
A cross-sectional institutional study was conducted among 603 school-age children in three district Rural districts Eastern zone of Tigray, Regional State of Ethiopia. Data were collected from September 10, 2024, to October 30, 2024.
Eligibility criteria
All school-age children between the ages of 6 and 12-years children
Inclusion Criteria.
School-age children between the ages of 6 and 12 years and children who attend primary schools within the study were included.
Exclusion Criteria.
Children whose parents or guardians do not provide informed consent for their participation in the study were excluded.
Sampling procedure and technique
This study utilized a multi-stage sampling approach, which involved dividing the population into clusters and randomly selecting clusters for sampling. Within each selected cluster, schools were sampled using simple random sampling. The final sample of students was then selected using systematic random sampling, where the interval (K) for selection was determined.
Initially, the primary schools providing education to school-age children in the Rural Districts of the Eastern Zone of Tigray were identified. Subsequently, the sample size necessary for each school was determined through proportional allocation. A systematic selection process was employed to choose school-age children from each institution.
Data collection method and tools
Ten nurses and one supervisor without affiliation with the study school collected data using a structured interviewer-administered questionnaire and physical examination. The questionnaire included four main sections. The trained health professionals (nurses or health officers) clinically examined the exposed parts of the body in a well-illuminated private classroom to document the findings.
Variables
Dependent variables.
Skin diseases
Independent variable.
Socio-demographic information: Age, Sex, Grade, Resident….
Medical history: Family history of previous skin disease, Diagnosis of skin disease Receipt of treatment for skin disease
Hygiene and sanitary conditions: Bathing frequency, Use of soap, Cloth change frequency
Statistical analysis and management
Data were coded and entered into Epi Info version 7.2 and cross-checked for consistency and accuracy. After data cleaning, it was exported to SPSS version 27 for statistical analysis. Descriptive statistics were performed, and results were summarized using tables, texts, and figures. Frequency distribution and percentages were employed for categorical variables. Binary logistic regression was used to determine the magnitude and strength of association between a set of independent variables and the outcome variable at a p < 0.20 significance level. Variables significant at p < 0.20 with the outcome variable were selected for multivariate analysis. An odds ratio with a 95% confidence level was computed, and a p-value < 0.05 was used as the significance level. The Hosmer-Lemeshow goodness-of-fit model coefficients test procedure was used to test for model fitting.
Data quality assurance
To ensure data quality, a questionnaire was adapted from published literature, translated, and pretested. Data collectors received training and were supervised during data collection. Completed questionnaires were checked for errors. Reliability was assessed using inter-rater reliability and Cronbach’s alpha, while face validity was evaluated.
Ethical considerations
An official ethical clearance letter was obtained from the Mekelle University College of Health Sciences Institutional Review Board (IRB) on 30 July 2024 with Protocol of Approval MU-IRB 2278/2024. Moreover, the members of the IRB or ethics committee who approved this study were Professor Haftu Berhe Gebru, Dr Tesfay Gebregzabher Gebrehiwot, Dr Mengistu Welday Gebremihael, Dr Meskelu Kidu Weldetensae, Dr Abraha Hailu Weldegerima, Dr Gebretsadik Berhe, and Gidey Gebremeskel. A formal letter for permission and support was written to the respective administrator’s office. The purpose of the study was clearly explained, informed oral consent was maintained, confidentiality was ensured, and assent was obtained from the study subjects who are greater than eight years old. Parents were given consent forms for their written approval before data collection began. Detailed information about the child was subsequently gathered from their parents. Parents who were unwilling to participate from the beginning or any part of the interview were allowed to do so. There was no risk of danger or hazardous procedures putting the participants in harm.
Result
In this study, a total of 603 out of 603 samples were included, yielding a response rate of 100%.
Socio demographic characteristics of study participants
The response rate was 100% (603), among them, 289 (47.9%) were male. The mean age of the participants was 9.41 years (±1.66 SD), and the average number of rooms in their households was 1.51 (±1.04). The total number of beds in the school-aged children’s home ranged from a minimum of 1 to a maximum of 4. Out of 603 participants, 416 (69%) lived with their mother and father. Additionally, the educational status of caregivers, with the category of illiterate, accounted for 459 (76.1%). Furthermore, 208 (65.5%) of the participants were from the host community, and 483 (80.1%) caregivers identified as farmers (Table 1).
Table 1: Socio-demographic status of study participants in the prevalence of skin disease and associated factors among school-age children of Rural District of Eastern Zone, Northern Ethiopia, 2024.
Medical History
From the total of 603 participants, 212 (35.2%) caregivers had a previous history of skin disease. Among these caregivers, 65 (10.8%) had skin disease for less than one month, while 89 (14.8%) caregivers had skin disease for a duration of 1–6 months, and 46 (7.6%) caregivers noted that the condition had persisted for more than one year. Of the 168(28%) family members diagnosed with a skin disease, 167 (27.7%) received treatment. Finally, 20 (3.3%) of the children had underlying health conditions. (Table 2).
Table 2: Medical History of Participants in the Prevalence of Skin Disease and Associated Factors among School-age Children of Rural District of Eastern Zone, Northern Ethiopia, 2024.
Hygiene and sanitary conditions
Among 603 participants, 519 (86.1%) take a bath or shower fewer than four times a month. The use of soap during bathing was reported by 595 (98.7%) individuals. From the total of 603 participants, 4 (6.6%) distinguished that they never shared personal items, while 60 (10.0%) indicated they always did. Only 187 (31.0%) participants wash their hands after using the restroom, and 84 (13.9%) wash their hands before meals, with the remaining 144 (23.9%) participants not washing their hands regularly. Regarding the frequency of changing clothes, 162 (26.9%) changed clothes daily, while 285 (47.3%) changed them once a week. Access to clean water for bathing and washing was available to 568 (94.2%) participants. Lastly, only 17 (2.8%) reported using tap water, while 80 (13.3%) stated they used river water (Table 3).
Table 3: Hygiene and sanitary conditions of participants in the prevalence of skin disease and associated factors among school-age children of Rural District of Eastern Zone, Northern Ethiopia, 2024.
Prevalence of skin disease
The prevalence of skin disease among the school-aged children in Rural Districts of the Eastern Zone of Tigray was 411 (68.2%) (95% CI: 64.2–72.0).
The common types of skin diseases identified
The frequency of various types of skin diseases reveals a diverse spectrum of conditions. Based on the three categories of skin disease specified in this study, infections account for 36%, allergic dermatitis for 12.8% and trauma related conditions for 18.7% (Fig 1).
Types of skin disease among school-aged children of rural district of Eastern Zone of Tigray Ethioipia 2024.
Variables with p value less than 0.2 in the bivariate analysis were included in the multivariable logistic regression. These variables were: community living residence status (IDP or Host), living arrangements (with mother, father, or caregiver), caregiver’s educational status and occupation, family history of skin disease, frequency of bathing, cloth sharing habits, hand washing practices, frequency of cloth changing, sharing of personal items, presence of domestic animals, and type of water used (Table 4).
Table 4: Bivariate analysis of factors associated with skin disease among school-age children of Rural District of Eastern Zone, Northern Ethiopia, 2024.
Factors associated with skin diseases among school-aged children
According to the multivariate logistic regression analysis, four (Community status, Family history of skin disease, Hand-washing practices, and sharing of personal items) variables were significantly associated with the occurrence of skin disease. Therefore, the odds of having skin disease were 2.96 (95% CI: 1.86–4.7) higher among the school-aged children living in IDP compared to the school aged children living in the host community. The odds of having skin disease is 8.22(95% CI: 5.19–13) higher among families with a history of skin disease compared to families without a history of skin disease. The odds of having skin disease is 3.89 (95% CI: 2.11–7.17) higher among children who share personal items compared to children who did not share personal items. The odds of having skin disease is 4.93 (95% CI: 2.66–9.11) higher among those who never wash their hands regularly compared to those who always wash their hands after using the toilet. (Table 5).
Table 5: Multivariate analysis of factors associated with skin disease among school-age children of rural district of eastern zone, northern Ethiopia, 2024.
Discussion
The primary objective of this study is to assess the prevalence and factors associated with the occurrence of skin diseases among school-age children in the Rural District of the Eastern Zone of Tigray, Ethiopia. Understanding the prevalence and associated factors is vital for developing targeted interventions to mitigate skin diseases in this vulnerable population. The findings of this study revealed a notable prevalence of skin diseases among school-age children, recorded at 68.2%. This high prevalence underscores the urgent need for public health initiatives aimed at improving skin health in rural communities. Additionally, several factors were identified as significantly associated with the occurrence of skin diseases, including community status as Internally Displaced Persons (IDP), a previous family history of skin disease, hand-washing practices, and the sharing of personal equipment. Each of these factors highlights critical areas for intervention and further investigation to reduce the burden of skin diseases in this population.
The findings revealed that the prevalence of skin disease among school-age children was 68.2%. Moreover, community residence status as IDP, previous family history of skin disease, sharing of personal items, and never washing their hands regularly were significantly associated variables in this study. However, the occupation of the parent as a farmer was not associated, as the high proportion of farmers may dilute the impact of occupation on skin health, which could be because over 80% of the parents were farmers.
The findings of this study have a higher prevalence of skin disease than the findings in Sri Lanka (63.9%) [4], India (60.59%) [11], Southern Co∘te d’Ivoire (25.6%) [12], Colombia (42.8%) [7], Ethiopia (61.2%) [3]. The possible explanation for this high prevalence may be due to the conflict in Tigray, which damaged hygiene and sanitary facilities in schools and communities. Moreover, due to the conflict, people were displaced from their residences and became vulnerable to skin diseases due to a lack of access to clean water, soap, latrines, and even shelter. All of these factors may contribute to the higher prevalence of skin diseases among school-age children. This explanation is supported by a study on water supply infrastructure [13].
The hand hygiene practice was also found to increase the odds of never washing hands regularly compared to those who washed their hands regularly, with an Adjusted Odds Ratio of 4.93. This finding was higher than a study conducted in Northern Ethiopia, where the Adjusted Odds Ratio was 1.78. [1]. The possible reason could be Limited access to clean water, soap, and proper hand-washing facilities can significantly affect hand hygiene practices in rural communities. Additionally, a lack of educational programs promoting the importance of hand hygiene may result in low awareness and poor practices among children and families. Without both the necessary resources and the knowledge of their importance, maintaining consistent hand washing habits becomes challenging [14,15].
This study found that sharing personal items, such as clothes and towels, significantly increased the odds of having skin diseases compared to those who did not share any personal items, with an adjusted Odds Ratio of 3.89. This finding was higher than a study conducted in Northern Ethiopia (Debre Berhan town) where the Odds Ratio was 1.5 [3]. The possible reason for the high Odds of skin diseases due to sharing personal items could be a lack of clothes and other personal items like towels. This might be because this study was conducted among school-age children living in rural areas, and the effects of post-war conditions [16].
This study confirmed that participants with a family history of skin disease were at an increased Odds of skin disease compared to their counterparts, with an adjusted odds ratio of 8.22. The possible explanation might be due to the war in Tigray damaged health services and the living conditions of the community such as sleeping in one room [1].
According to this study, the Odds of having skin disease were significantly increased among IDPs as compared with the host community, with an Adjusted Odds Ratio of 2.96. This finding was in line with the study conducted in Armachiho district, 3.47 [17]. The possible explanation is that both studies included internally displaced People, who are vulnerable to skin disease due to a lack of access to clean water, detergents, Living conditions, Economic status, hygiene, and sanitary facilities [18].
The study highlights a high prevalence of skin diseases among school-age children in the Rural District of the Eastern Zone of Tigray, emphasizing the urgent need for public health interventions. Contributing factors include community status as Internally Displaced Persons, family history of skin disease, poor hand hygiene, and sharing personal items. The impact of conflict has disrupted sanitation and access to clean water, exacerbating these issues. These findings underscore the necessity for targeted strategies to improve skin health in this vulnerable population.
Strength and limitations of the study
Strength of the study.
The cross-sectional design of the study prevented the determination of causal relationships.The study was conducted over a limited timeframe, which may have overlooked seasonal variations in skin diseases that could influence the findings
Conclusion
The prevalence of skin disease among school-aged children in the Rural District of the Eastern Zone was found to be remarkably high, representing nearly two-thirds of the population. Community residence status as IDP, previous family history of skin disease, sharing of personal items, and children who never wash their hands, were significantly associated variables in this study. The prevalence of skin disease among school-age children was high. The majority of identified skin diseases were Macule and Erosion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tefera S, et al. Prevalence of scabies and associated factors among primary school children in Raya Alamata District, Tigray, Ethiopia, 2017/2018. J Infect Dis Epidemiol. 2020;6:154.
- 2Hay R. Skin diseases. Disease Control Priorities in Developing Countries. 2nd ed. 2006.21250309 · pubmed ↗
- 3Mengist Dessie A. Prevalence of skin disease and its associated factors among primary schoolchildren: A cross-sectional study from a northern Ethiopian town. Clinical, Cosmetic and Investigational Dermatology. 2022;791–801.35521561 10.2147/CCID.S 361051 PMC 9063791 · doi ↗ · pubmed ↗
- 4Gunathilaka N, Chandrasena N, Udayanga L. Prevalence of Ectoparasitic Infections and Other Dermatological Infections and Their Associated Factors among School Children in Gampaha District, Sri Lanka. Can J Infect Dis Med Microbiol. 2019;2019:5827124. doi: 10.1155/2019/5827124 31019612 PMC 6452534 · doi ↗ · pubmed ↗
- 5Khalifa KA, Al-Hadithi TS, Al-Lami FH, Al-Diwan JK. Prevalence of skin disorders among primary-school children in Baghdad governorate, Iraq. East Mediterr Health J. 2010;16(2):209–13. doi: 10.26719/2010.16.2.209 20799576 · doi ↗ · pubmed ↗
- 6Tempark T, Whaidee K, Bongsebandhu-Phubhakdi C, Suteerojntrakool O. Prevalence of skin diseases in school-age children. Fam Pract. 2022;39(3):340–5. doi: 10.1093/fampra/cmab 164 34871400 · doi ↗ · pubmed ↗
- 7García E, Halpert E, Borrero E, Ibañez M, Chaparro P, Molina J, et al. Prevalence of skin diseases in children 1 to 6 years old in the city of Bogota, Colombia. World Allergy Organ J. 2020;13(12):100484. doi: 10.1016/j.waojou.2020.100484 33294116 PMC 7689333 · doi ↗ · pubmed ↗
- 8Schmitz R, Atzpodien K, Schlaud M. Prevalence and risk factors of atopic diseases in German children and adolescents. Pediatr Allergy Immunol. 2012;23(8):716–23. doi: 10.1111/j.1399-3038.2012.01342.x 22882467 · doi ↗ · pubmed ↗