Feasibility and Safety of Allied Health Professional Delivered Clinics for Suspected Head and Neck Cancers: A Scoping Review
Neginsadat Mirtorabi, Dimitrios Spinos, Christopher Coulson, Paul Nankivell, Jameel Muzaffar

TL;DR
This study explores the feasibility and safety of using Allied Health Professionals to perform nasoendoscopy clinics for suspected head and neck cancers, with consultant review of recorded videos.
Contribution
The novelty lies in evaluating the use of AHPs in asynchronous clinics for head and neck cancer diagnostics, focusing on safety and efficiency.
Findings
AHP-delivered clinics detected minimal cancers in low-risk patients without missing malignancies.
Remote pathways achieved prompt diagnoses with diagnostically adequate recordings.
ENT surgeons reported improved efficiency but emphasized the need for AHP training and governance.
Abstract
In the UK alone, suspected head & neck cancer referrals exceed a quarter‐million, with a detected malignancy rate of around 2.6%1. This, coupled with the need for urgent assessment and treatment of cancer patients, puts an increasing strain on clinical services. Advances in technology have allowed integration of video‐endoscopy, particularly ‘store and forward’ of clinical media and patient information for deferred consultant review. Building on these, Allied Health Professional (AHP)‐delivered nasoendoscopy clinics emerged: AHPs perform endoscopy and a consultant reviews the video asynchronously. This model, in theory, preserves specialist input while helping to address current clinical pressures. A scoping review was conducted per PRISMA‐ScR guidelines (PROSPERO 1016067). We searched MEDLINE, EMBASE, PubMed, Emcare, and CINAHL for relevant English‐language studies up to April 2025.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
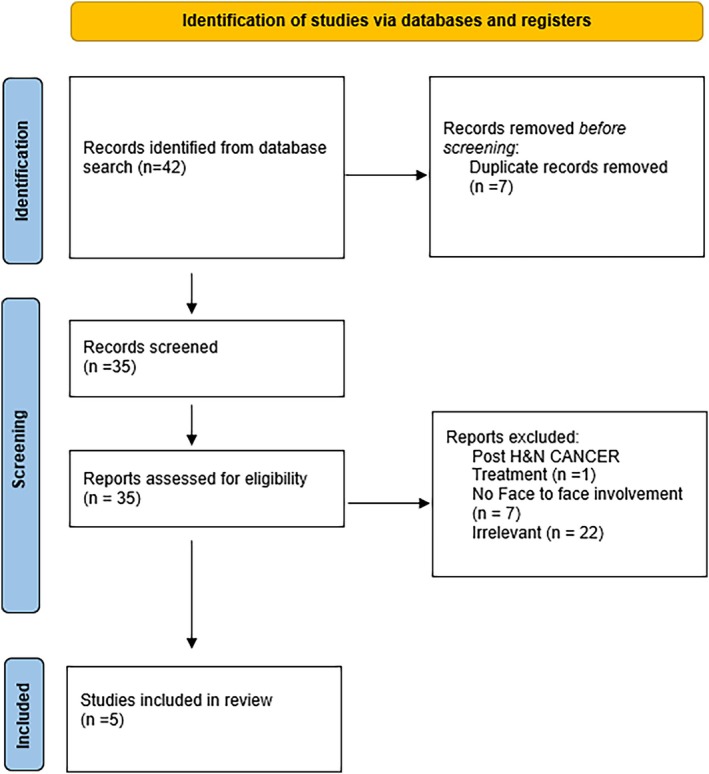 FIGURE 1
FIGURE 1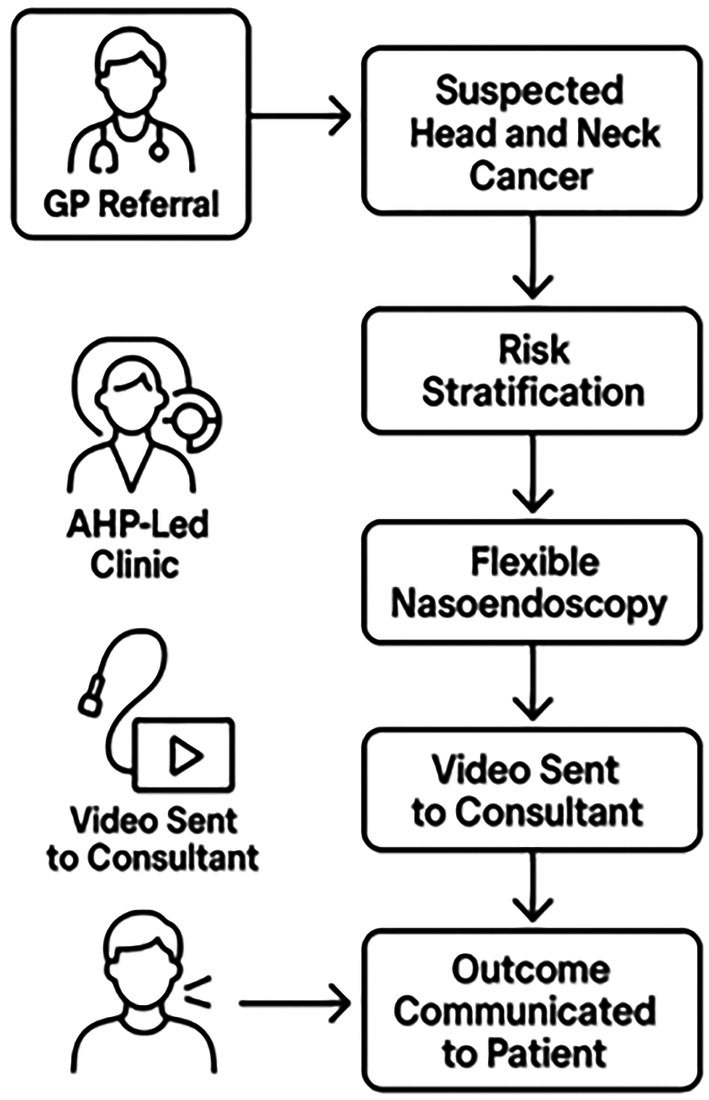 FIGURE 2
FIGURE 2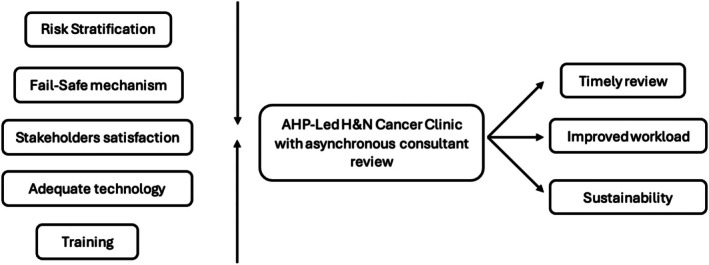 FIGURE 3
FIGURE 3| First author | Year | Country | Number of patients/participants | Modality of service | Type of study |
|---|---|---|---|---|---|
| Christopher Metcalfe | 2022 | United Kingdom | 661 (total referrals, 340 telescopic) | Novel telescopic pathway vs. conventional standard of care | Prospective service evaluation |
| Jen Butler | 2023 | United Kingdom | 218 | SLT‐delivered 2‐week wait assessment clinic | Prospective pilot clinic |
| Christopher Metcalfe | 2024 | United Kingdom | 660 (low‐risk patients) | Nurse‐delivered clinic with asynchronous consultant review | Prospective service analysis |
| Louise C. Occomore‐Kent | 2025 | United Kingdom | 11 ENT surgeons | Exploration of views of ENT surgeons on SLT‐delivered first point of contact clinic | Qualitative study |
| Louise Occomore‐Kent | 2021 | United Kingdom | NA | SLT‐delivered 2‐week wait assessment clinic | Opinion on pilot study |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Cancer Studies · Patient-Provider Communication in Healthcare · Cervical Cancer and HPV Research
Introduction
1
Between 2022 and 2023, 275,354 suspected Head and Neck (H&N) cancer referrals were made in the United Kingdom (UK), with only 2.6% resulting in a cancer diagnosis [1]. The Faster Diagnosis Standard (FDS) for H&N cancer specifies that imaging and multidisciplinary discussion should be completed within 28 days of referral [2]. Given the relatively low cancer conversion rate, the associated anxiety for patients, and the considerable clinical and administrative workload of assessment, there is a clear need for redesigned pathways that deliver safe, streamlined care.
The COVID‐19 pandemic accelerated the development of alternative referral models, including telephone triage [3], risk‐stratification calculators [4], and one‐stop neck lump clinics [5]. Technological advances also enabled wider use of video‐endoscopy, particularly store‐and‐forward systems for uploading clinical media for delayed consultant review [6]. Building on these innovations, increasing attention has been directed toward expanding the role of Allied Health Care Professionals (AHPs) in initial assessment pathways. Under this model, AHPs conduct the clinical examination and consultants subsequently review the recorded images and videos asynchronously. With only 2.19 otolaryngology–head and neck consultants per 100,000 population globally [7], consultant time is an increasingly scarce resource. Asynchronous review models preserve specialist oversight while reducing pressure on consultant‐led clinics. Comparable approaches have been successfully piloted in other ENT subspecialties, including otology and rhinology [6].
Introducing such pathways requires careful planning to safeguard clinical standards. Logistical considerations—including triage criteria, digital image handling and transfer, long‐term follow‐up arrangements, and comprehensive AHP training—must be addressed to ensure quality and safety. This scoping review evaluates the feasibility and diagnostic safety of AHP‐delivered clinics with asynchronous consultant review. It further examines the range of remote formats trialed, their adherence to clinical governance standards, and their acceptability to clinicians and patients.
Material and Methods
2
A scoping review was conducted and reported based on the PRISMA‐ScR checklist. This scoping review is registered on PROSPERO with registration number 1016067.
A literature search was conducted across Medline, EMBASE, Emcare, PubMed, and CINAHL. Search terms included, but were not limited to: “FNE,” “2‐week wait,” “head and neck cancers,” “allied health care professionals,” “remote review” and “video review” (Appendix A). These terms were used in various combinations to ensure the retrieval of relevant studies across all selected databases. The review focused on studies published in English, within the past 25 years, with an end‐date on April 2025.
All retrieved records that met the inclusion criteria were independently screened for relevance and quality by two reviewers. Any discrepancies were resolved through discussion, facilitated by a third reviewer. Data extraction focused on study characteristics, participant demographics, methodology, and outcomes. The primary outcomes of interest were risk stratification, stakeholder satisfaction, and clinical feasibility and safety. The heterogeneous nature of included papers with respect to methods and outcomes meant analysis was restricted to qualitative synthesis of themes, following principles of grounded theory.
Results
3
Forty‐two papers were identified, with seven duplicate results. Two results were returned through EMBASE, 19 through Ovid MEDLINE, and 21 through PubMed (Figure 1). Exclusion criteria included any paper that did not specifically relate to H&N cancer pathology, did not include remote assessment by clinicians, and those which did not include use of video imaging. To ensure review of the most relevant studies, inclusion criteria consisted of any papers published between 2000 and 2025, in English, involving H&N cancer adult patients. Based on these criteria, five papers were included in the study.
PRISMA flow chart.
Five papers were included in the study, with the publication date ranging from 2019 to 2025 (Table 1). All papers were published within the UK. Overall, three studies [8, 9, 10] focused on use of Speech and Language Therapists (SLTs) while the other two [11, 12] looked at use of nurses in H&N cancer clinics. One paper [10] focused on the scope of SLTs in their ability to initiate management for specific red flag symptoms such as hoarseness of voice.
Across the reported studies, three used a triage system [9, 12] or the Head and Neck Cancer Risk Calculator (Version 2 (HaNC‐RC v.2)) [11] prior to assigning patients to traditional clinician‐led clinic models or to remote/asynchronous review.
One study [8] specifically assessed stakeholders' satisfaction by looking at the acceptability of AHP‐delivered clinics by ENT consultant surgeons. In this paper, thematic analysis revealed that the surgeons identified potential benefits, including improved governance, early cancer detection, cost savings, reduced workload for ENT surgeons, and the utilization of existing SLT resources [8]. However, concerns were raised regarding the legal authority for SLTs to make independent mucosal diagnoses, variable levels of SLT competence in differentiating benign from concerning symptoms, and patient expectations [8].
In terms of outcome measures, 3 studies [9, 11, 12] focused on the cancer diagnostic yield and review within a short time frame. The diagnostic rate was reported to be less than 1% for 715 patients [11, 12]. Butler et al. [9] had a higher cancer diagnostic yield of 5%, with high‐grade dysplasia detected in 3% of cases. Images and management plans could be reviewed and formulated in almost 1 week [9] and the mean waiting time was demonstrated to align with the NHS cancer pathway targets [2, 11]. Metcalfe et al. further demonstrated a shorter time to diagnosis compared to the standard pathway [11].
Cancer detection rate and re‐referral was low across the reviewed papers. In Metcalfe et al. prospective analysis, six head and neck cancers were diagnosed (0.9% conversion rate) from the 660 low risk patients [12]. Remote videos were deemed adequate in 98.9% [12]. During a mean follow‐up of 15 months, 21 patients (3.2%) were re‐referred; no head and neck cancers were identified on re‐referral, and there were no missed cancers in the follow‐up period [12]. In another study, out of the 155 low risk patients, no cancer was diagnosed (< 1%), with no re‐referrals within three months [4]. Among high‐risk consultant‐led patients, 31 cancers were identified (17% conversion rate) [11]. In the conventional consultant‐delivered standard‐of‐care pathway during the same period, 74 patients were reviewed face‐to‐face, with four cancers detected (5.4%) [11].
All five papers [8, 9, 10, 11, 12] commented on the acceptable safety profile of AHP‐delivered cancer clinics. There was no requirement for a second ENT opinion [9] and no new cancer diagnosis within follow up periods [11, 12].
Discussion
4
This scoping review examined the feasibility of remote asynchronous review of nasoendoscopes for suspected H&N cancer patients (Figure 2). Although there have been a limited number of papers published on this subject, the evidence so far suggests this is a safe, effective, and reproducible approach. The importance of risk stratification, stakeholder satisfaction, consistent clinical standards, failsafe strategies, and sustainability need to be addressed (Figure 3).
Sample algorithm of AHP‐delivered clinic.
Feasibility of AHP‐delivered H&N clinics and potential benefits.
Clinical Efficacy and Feasibility
4.1
Risk Stratification
4.1.1
Effective risk stratification is critical for selecting appropriate patients for remote review clinics. During the COVID‐19 pandemic, the British Association of Head and Neck Oncologists (BAHNO) advocated the use of a validated H&N cancer risk calculator to support patient stratification [4]. One commonly employed approach is symptom‐based risk assessment, which evaluates the presence and severity of specific clinical indicators such as persistent hoarseness, unexplained weight loss, or non‐healing ulcers [13]. In a prospective population‐based study, Hardman et al. demonstrated that remote triage incorporating symptom‐based stratification safely managed suspected H&N cancer referrals, as evidenced by a low conversion rate to cancer diagnoses, thereby reducing unnecessary hospital attendance for low‐risk patients [14]. It is important to highlight that the location of the suspected lesion should play a part in risk stratification. Asynchronous endoscopic review is most appropriate for subsites of the upper aerodigestive tract that are accessible via flexible nasendoscopy, rather than for all potential head and neck cancer presentations. As highlighted in Metcalfe et al. [11, 12] the telescopic pathway was specifically designed for low‐risk referrals requiring visualization of the larynx and pharynx. Patients presenting with neck masses without an obvious primary or lesions confined to the oral cavity or tonsils were triaged as high‐risk and either directed to face‐to‐face consultant assessment or primary imaging prior to review. Similarly, Butler et al. [9] and Occomore‐Kent et al. [8] emphasized that SLT‐led clinics are best suited to evaluating pathologies of the larynx and pharynx, where endoscopic visualization is possible and within established SLT competencies, rather than intra‐oral or submucosal lesions.
Another tool, the Head and Neck Cancer Risk Calculator (Version 2), is a statistical model that predicts an individual's H&N cancer risk by generating a percentage score based on symptoms, demographics, and lifestyle factors [4]. This calculator aids in directing patients to the appropriate referral pathways, either for urgent suspicion of cancer or for routine care. However, Ying Tan et al. reported that integrating this tool into primary care settings may increase the number of urgent referrals, even when the absolute risk remains low [15].
With the growing influence of artificial intelligence (AI), machine learning (ML) models have also been applied to risk stratification both before and after diagnosis. Notably, variational logistic regression predicts an optimal balance between the accurate identification of patients without cancer (high true negative rate) and minimisation of the misclassification of patients with cancer (low false negative rate) [16]. ML models may be applied to complex datasets, containing such data as clinical symptoms, imaging, and patient demographics, to enhance the predictive capacity of probabilistic classification [16]. This refined classification in turn improves diagnostic accuracy, expedites referrals, and optimizes treatment pathways. Improved identification of true negatives creates further opportunity for the development of alternative pathways within secondary care for managing non‐cancerous diagnoses more efficiently [16]. Such improvements could potentially reduce the overall referral rate from primary care, leading to significant efficiency savings [16].
Image Quality
4.1.2
Remote videoendoscopy, whether synchronous or asynchronous, has been trialed in other areas of ENT, including otology and rhinology [7]. Indeed, Miller et al. focused on the feasibility of remote nasendoscopy in pediatric patients [17]. In their study, 45 pediatric patients underwent nasopharyngolaryngoscopy. The examination was recorded and a second remote otolaryngologist reviewed the images [17]. Results showed adequate diagnostic accuracy and smooth operation. Elsewhere, Kokesh et al. found video‐otoscopy images to be comparable to an in‐person examination [18].
Video imaging increases the potential for dynamic assessment pathways, particularly in such cases as vocal cord pathologies. Clearly, image and video quality are pivotal to the viability of such pathways. For a consultant to make an accurate diagnosis remotely, images must be consistent and sufficiently detailed. In the reviewed studies, the quality of videos and images was not assessed formally.
Image data must also be stored in a sufficiently small size to enable transfer, without impacting quality. Metcalfe et al. used video compression to improve storage and data transfer, notably allowing for the storage of videos in patients' records for the optimisation of communication and assessment during multi‐disciplinary team (MDT) meetings and discussion [12].
Safety
4.1.3
An even more important question to be answered when assessing feasibility is whether this method is safe at detecting cancers, and what fail‐safe mechanisms are needed to mitigate risks associated with remote assessments, such as misdiagnosis or missed cancers. Studies by Butler et al. [9] and Metcalfe [12] examined the safety profile of remote assessment. The rate of high‐risk diagnosis in patients triaged to be seen by AHPs was low, but the absence of re‐referrals indicates that the clinic's assessments were comprehensive and accurate [9, 12]. In Metcalfe et al. study, there were no missed cancers during the follow‐up period, underscoring the safety of the proposed pathway [12]. The pathway also met the 28‐day faster diagnosis standard, demonstrating its efficacy in timely cancer detection. The asynchronous review of images within 1 week in the reviewed studies highlights the safety netting available [3].
Training
4.1.4
Training AHPs to safely assess patients and perform FNEs is of paramount importance in ensuring the feasibility of remote clinics. Adequacy of training, professional recognition of AHPs, and the establishment of robust governance structures to ensure patient safety and quality of care are challenges that must be addressed [8]. SLT practitioners already get training to perform fibreoptic endoscopic evaluation of swallowing (FEES) [19], and expanding these skills to the performing of FNE should be eminently practical. The use of simulation when training allows practitioners to gain confidence and repetitive experience in performing endoscopy without compromising patient care [19]. Despite this, there is very limited focus in the literature on the ideal training curriculum and requirements needed to ensure that AHPs are adequately prepared.
Stakeholder Satisfaction
4.2
For remote pathways of care to be successful, all stakeholders, including both clinicians and patients, must be satisfied. Studies indicate that clinicians generally accept remote assessment pathways, provided they are well‐structured and integrate seamlessly with existing workflows. Certainly, O Commore‐Kent et al. semi‐structured interviews with 11 UK‐based ENT surgeons highlighted a generally favorable view [8]. Workforce availability and organizational support were vital to the implementation and success of these clinics [8]. On the whole, consultants acknowledged potential advantages, including efficient management of low‐risk patients, reduced waiting times, and the effective use of AHPs' specialized skills in laryngeal examination and flexible nasoendoscopy [8].
The satisfaction of patients with remote review is as critical a consideration as that of clinicians. Although specific data on patient satisfaction were limited in the reviewed studies, convenience and reduced commuting are likely to be well‐received by patients [20, 21]. Smith et al. highlighted early diagnosis and anxiety resolution as particular factors that led to higher patient satisfaction [22]. If patients triaged into low‐risk groups are seen in the remote pathway, a higher proportion of consultants' time will be spent seeing those with more complex needs. This allows more time to be spent on those consenting to potential interventions or an explanation of their diagnosis, whereas patients with benign pathology can be reassured remotely in a timely manner. If a credible technician can procure data that are reviewed by a consultant, and results are communicated to patients by appropriate individuals in a timely manner, patient satisfaction should not be impacted negatively. For such an outcome to be achieved, it must be ensured that patients are adequately informed and comfortable with remote procedures.
The view of AHPs is another important consideration. Bradley et al. in their survey of 129 SLTs from all regions of the UK, found overall enthusiasm for expanding the scope of practice, if there is adequate training and supervision [23].
Another, somewhat less direct aspect of stakeholder satisfaction is the impact of this pathway on surgical training, particularly the training of future head and neck surgeons. While current patients will receive consultant‐led care, whether face‐to‐face or remotely, trainees may see a reduction in the number of H&N cancer referrals they encounter and assess [24]. On the other hand, recordings can provide a valuable learning resource where cases can be discussed and learnt from [25].
Sustainability
4.3
Another point in favor of streamlining cancer referral pathways and remote scoping review is the matter of sustainability. NHS England's Green initiative, as detailed in its Delivering a ‘Net Zero’ NHS strategy (NHS England, 2021) [26], recommends the transformation of outpatient services through telemedicine and digital platforms to reduce carbon emissions. Gerrard et al. quantified the environmental benefits of changing 100 appointments from face‐to‐face to remote, identifying reductions of 2150 patient travel miles, 47 occupied hospital car parking spaces, and 0.4 t of CO_2_ emissions. In this model, care can be delivered outside the hospital and therefore potentially reducing miles traveled. Transitioning to remote healthcare consultation on a larger scale should have proportionately significant ecological advantages [27].
Similarly, the Royal College of Surgeons underscores the importance of environmental sustainability in its Sustainability and Environment Report (Royal College of Surgeons, 2022), advocating the integration of remote consultation technologies within surgical pathways [28]. A systematic review by Ravindrane et al. found that all 14 included studies reported environmental benefits to telemedicine over face‐to‐face consultations, primarily through reduced greenhouse gas emissions from travel [29].
Future Perspectives
4.4
Despite the limited number of studies identified that focused on the use of AHPs performing FNEs in H&N cancer clinics, the overarching theme of those reviewed here is that low‐risk patients could safely be seen by AHPs, with images reviewed shortly after by a consultant. The low rate of cancer diagnosis in patients identified by remote review as low‐risk further highlights both the efficacy of triage systems, whilst the low rates of re‐referral and missed cancers highlight the proficiency and safety of AHP‐led clinics.
Our review identified three main gaps in the literature. Firstly, there is no formal study on the cost‐effectiveness of this remote review compared to traditional pathways. Although asynchronous review may be cost‐effective at the time that it is performed, the cost of setting up AHP‐delivered clinics, equipment and training must be considered. Secondly, more studies are needed to evaluate the views of AHPs in the expansion of their practice, the training and responsibility that would come with this expansion, and the implications for AHP workforce planning. Finally, there are few adequate validation studies on the software needed for recording, storing and transferring imaging data.
Conclusion
5
This scoping review demonstrates that AHP‐delivered nasoendoscopy for suspected H&N cancer patients with asynchronous consultant review is a safe and promising approach. This is, however, contingent on the integration of robust risk stratification, stakeholder engagement, and stringent clinical governance. Such pathways support faster diagnosis and operational efficiency while aligning with broader aspirations to modernize care delivery and reduce environmental impact. Overall, the evidence supports the clinical efficacy and safety of remote pathways, although further research is required to refine these protocols and assess their long‐term impact on service efficiency and patient outcomes.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NHS England , “Cancer Waiting Times Referral Conversion Detection Dashboard,” accessed 2025 May 4, https://digital.nhs.uk/ndrs/data/data‐outputs/cancer‐data‐hub/urgent‐suspected‐cancer‐referrals.
- 2NHS England , “Care Excellence: Head and Neck Cancer—Implementing a Timed Diagnostic Pathway,” (2024), https://www.england.nhs.uk/wp‐content/uploads/2018/04/B 1130‐head‐and‐neck‐cancer‐implementing‐a‐timed‐diagnostic‐pathway‐07‐06‐2024.pdf.
- 3A. Rovira , S. Brar , T. Munroe Gray , E. Ofo , C. Rodriguez , and D. Kim , “Telephone Consultation for Two Week Wait ENT and Head and Neck Cancer Referrals: Initial Evaluation Including Patient Satisfaction,” Journal of Laryngology and Otology 136, no. 7 (2022): 615–621.34698005 10.1017/S 0022215121003157 · doi ↗ · pubmed ↗
- 4T. Tikka , K. Kavanagh , A. Lowit , et al., “Head and Neck Cancer Risk Calculator (Ha NC RC)–v.2: Adjustments and Addition of Symptoms and Social History Factors,” Clinical Otolaryngology 45, no. 3 (2020): 380–388.31985180 10.1111/coa.13511 PMC 7318185 · doi ↗ · pubmed ↗
- 5A. Hariri , S. Jawad , and S. R. Otero , “Rethinking the ‘One Stop’ Neck Lump Clinic: A Novel Pathway Beyond Coronavirus Disease 2019,” Journal of Laryngology and Otology 137, no. 6 (2023): 704–708.36815299 10.1017/S 002221512300021 X · doi ↗ · pubmed ↗
- 6D. Spinos , C. Coulson , T. Beech , et al., “Advances in Remote Otology and Rhinology Service Delivery: A Scoping Review,” American Journal of Otolaryngology 45, no. 6 (2024): 104399.39153399 10.1016/j.amjoto.2024.104399 · doi ↗ · pubmed ↗
- 7B. Petrucci , S. Okerosi , R. H. Patterson , et al., “The Global Otolaryngology Head and Neck Surgery Workforce,” JAMA Otolaryngology. Head & Neck Surgery 149, no. 10 (2023): 904–911, 10.1001/jamaoto.2023.2339.37651133 PMC 10472262 · doi ↗ · pubmed ↗
- 8L. C. Occomore‐Kent , J. C. Hardman , J. W. G. Roe , P. Bradley , P. N. Carding , and J. M. Patterson , “Speech and Language Therapist‐Led Clinics for Low‐Risk Suspected Head and Neck Cancer Referrals: A Qualitative Study of Ear, Nose and Throat Surgeons' Views,” International Journal of Language & Communication Disorders 60, no. 1 (2025): e 13137.39660964 10.1111/1460-6984.13137 PMC 11633375 · doi ↗ · pubmed ↗