Non-tuberculous mycobacterial infective endocarditis in a tuberculosis-endemic region after recent cardiovascular procedures: a case series
Shohael Mahmud Arafat, Chowdhury Adnan Sami, Abed Hussain Khan, Sudip Kumar Banik, Md. Mizanur Rahman Khan, Lovely Barai

TL;DR
This case series describes three patients with non-tuberculous mycobacterial infective endocarditis following heart procedures, highlighting diagnostic challenges and poor outcomes.
Contribution
The study presents a novel case series from a tuberculosis-endemic region, emphasizing the under-recognized risk of NTM-IE after cardiovascular procedures.
Findings
Three patients with NTM-IE following recent cardiovascular procedures had poor clinical outcomes despite antimicrobial therapy.
Diagnosis relied on repeated cultures and exclusion of tuberculosis, but species-level identification was not possible due to resource limitations.
Mortality was high, underscoring the need for a combined medical-surgical approach in managing NTM-IE.
Abstract
Background. Non-tuberculous mycobacterial infective endocarditis (NTM-IE) is an uncommon but increasingly recognized aetiology of culture-negative endocarditis, particularly in the context of healthcare exposure. Rapidly growing non-tuberculous mycobacteria (NTM) species present significant diagnostic and therapeutic challenges due to their indolent nature and clinical similarity to tuberculosis. Case summary. We describe a case series of three patients with native valve infective endocarditis caused by rapidly growing NTM following recent percutaneous coronary intervention. All patients initially presented with prolonged fever and systemic inflammatory signs, and routine microbiological workup results were negative. The diagnosis was based on repeated blood and/or urine cultures with the detection of rapidly growing NTM, exclusion of Mycobacterium tuberculosis by PCR analysis and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
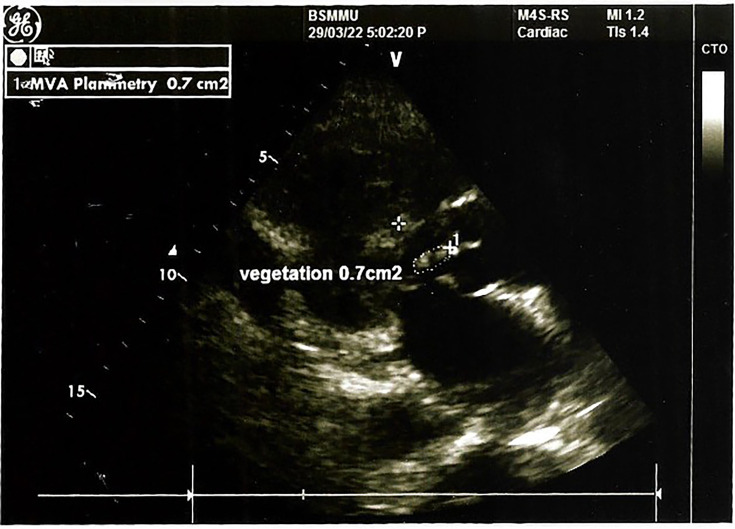 Fig. 1
Fig. 1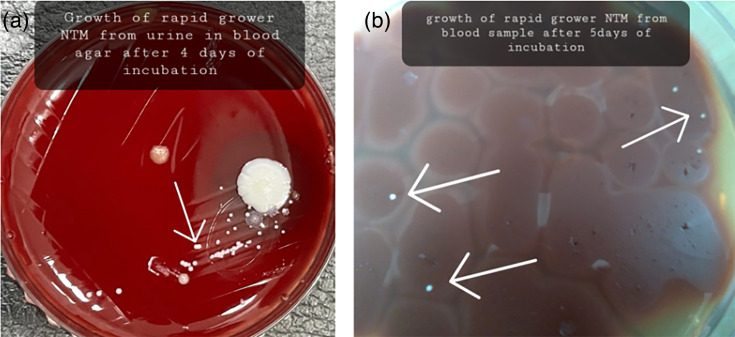 Fig. 2
Fig. 2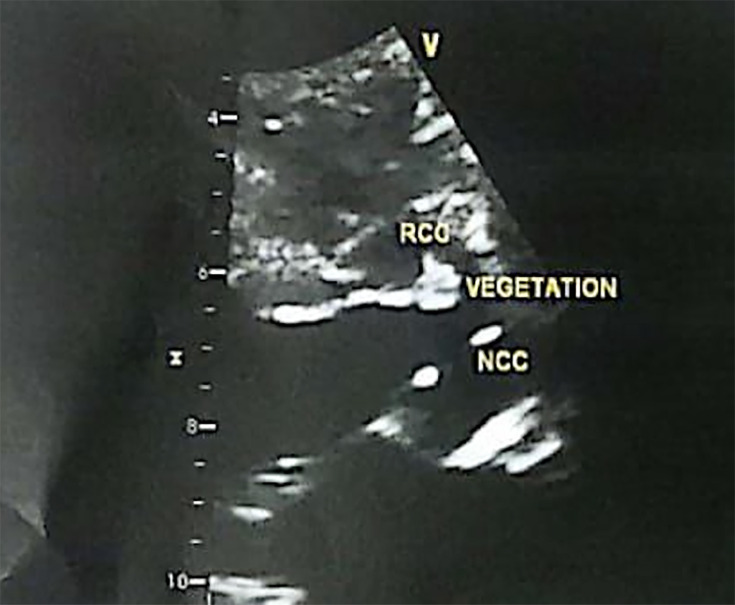 Fig. 3
Fig. 3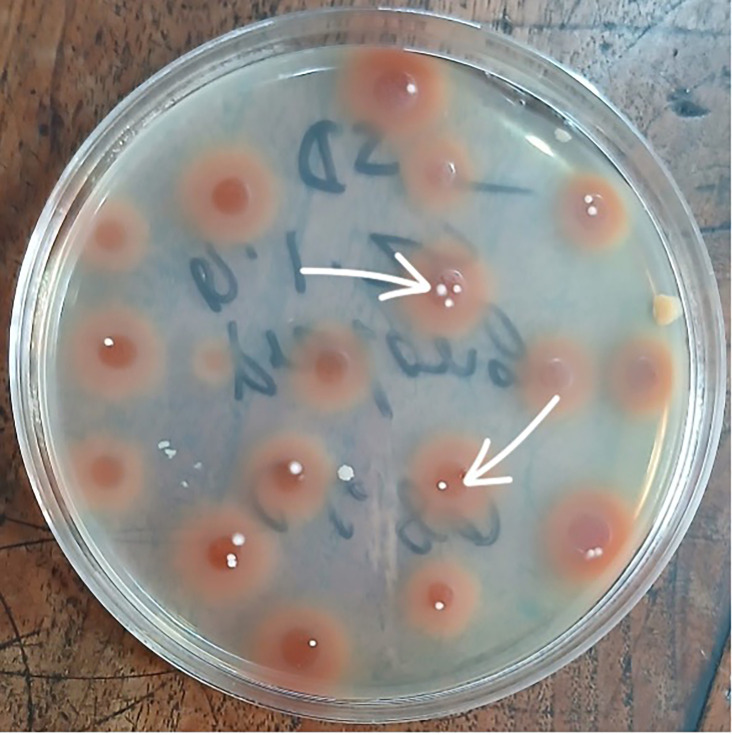 Fig. 4
Fig. 4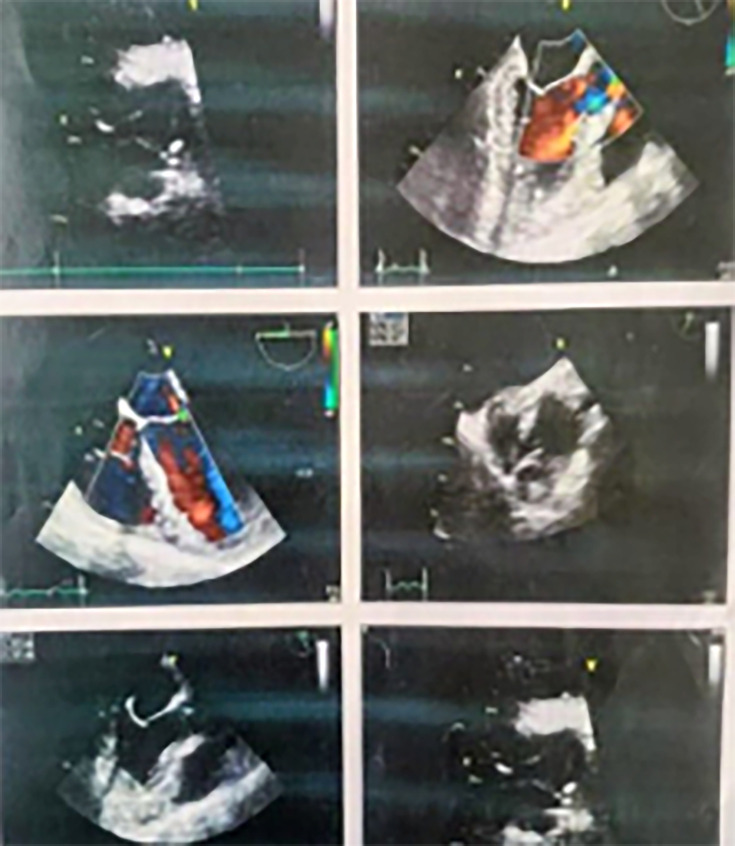 Fig. 5
Fig. 5 Fig. 6
Fig. 6| Investigation | Case 1 | Case 2 | Case 3 |
|---|---|---|---|
| Haemoglobin (g dl−1) | 9.5 | 8.3 | 7.4 |
| ESR (mm in first hour) | 120 | 45 | 06 |
| WBC×109 per litre | 7 | 4.5 | 3.5 |
| Platelets×109 per litre | 300 | 110 | 105 |
| C-reactive protein (mg dl−1) | 39.38 | 72.37 | 127.18 |
| Peripheral blood film | Dimorphic anaemia | Pancytopenia | Microcytic hypochromic anaemia |
| Creatinine (mg dl−1) | 1.11 | 3.9 | 1.28 |
| ALT (U l−1) | 54 | 39 | 42 |
| CXR P/A view | Normal | Normal | Normal |
| USG of whole abdomen | Normal | Normal | Hepatosplenomegaly |
| Transoesophageal echocardiography | Small vegetation at the tip of anterior mitral leaflet | Vegetation right coronary cusp (7×3 mm) and NCC (5×5 mm) | Vegetation attached to NCC of aortic valve (07×03 mm) |
| Blood culture | Rapid grower NTM (after 5 days of incubation) | Rapid grower NTM (after 4 days of incubation) | Rapid grower NTM (after 4 days of incubation) |
| Urine microscopy (Z–N stain) | AFB present | Not present | Not present |
| Urine culture (in blood agar) | Rapid grower NTM (after 4 days of incubation) | No growth | No growth |
| Bone marrow | Normal | Normal | Normal |
| NT proBNP (pg ml−1) | 2,100 | 14,977 | 510 |
| ICT for malaria and kala-azar | Negative | Negative | Negative |
| Anti-leptospira IgM and IgG | Negative | Negative | Negative |
| Anti-HIV (1+2) | Negative | Negative | Negative |
| ANA | Negative | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMycobacterium research and diagnosis · Infective Endocarditis Diagnosis and Management · Diagnosis and treatment of tuberculosis
Data Summary
No data, tools, software or code were generated or required for our work.
Introduction
Non-tuberculous mycobacterial infective endocarditis (NTM-IE) after cardiovascular procedures, especially post-percutaneous coronary intervention (PCI), is a less frequent but serious complication [1]. NTM-IE is frequently associated with rapidly growing mycobacteria, such as Mycobacterium fortuitum and Mycobacterium abscessus, which are resistant to common treatments and are responsible for culture-negative endocarditis [2]. The clinical picture may be difficult to determine because of the insidious nature of the infection and the scarcity of blood culture results. Diagnosis is challenging because routine cultures are often negative, and the clinical presentation overlaps with that of tuberculosis [2]. Treatment of NTM-IE includes surgical and medical approaches, and in some cases, complicated regimens of antibiotics and valve replacement are required [2].
We present three cases of non-tuberculous mycobacteria (NTM)-associated native valve infective endocarditis (IE) that developed following coronary stenting.
Methods
Microbiological identification and susceptibility testing
All microbiological investigations for all three cases were performed at the Department of Microbiology, Bangladesh Institute of Research and Rehabilitation in Diabetes, Endocrine, and Metabolic Disorders (BIRDEM). The same standardized laboratory protocols and quality control procedures were uniformly applied across all cases.
The isolates recovered from blood and/or urine cultures were phenotypically identified as rapidly growing NTM based on a combination of microbiological criteria, including growth within 7 days, characteristic colony morphology, Ziehl–Neelsen positivity, Gram-stain appearance from culture growth and absence of pigmentation on subculture in Lowenstein–Jensen medium. In addition, real-time PCR was performed on DNA extracted from cultured colonies using a commercial assay capable of differentiating the Mycobacterium tuberculosis complex from NTM (Viasure Real-Time PCR Detection Kit; Certest Biotech, Zaragoza, Spain), thereby excluding M. tuberculosis as the causative organism [3].
Species-level identification could not be performed because of the unavailability of MALDI-TOF or gene sequencing facilities at our centre, which we acknowledge as a limitation. Antimicrobial susceptibility testing was performed using the broth microdilution method with cation-adjusted Mueller–Hinton broth, in accordance with Clinical and Laboratory Standards Institute (CLSI M24) (third edition) guidelines [4].
To exclude laboratory contamination, repeat blood and/or urine cultures were done over three successive days in each case, all of which yielded concordant growth of rapidly growing NTM.
Case summary
Case 1
Clinical presentation
A 63-year-old man with long-standing diabetes mellitus and hypertension underwent PCI for double-vessel coronary artery disease via the right radial artery. Two months later, he started having intermittent high-grade fever, which went up to 104 °F and persisted for 6 months, along with a weight loss of 6 kg within the same period. There was no history of tuberculosis or known contact with patient having tuberculosis.
Diagnostic work-up
Initial testing for infectious causes was performed. Urine microscopy revealed acid-fast bacilli (AFB) on Ziehl–Neelsen staining, and the interferon-gamma release assay (QuantiFERON-TB Gold) was positive, prompting suspicion of genitourinary tuberculosis. The GeneXpert MTB/RIF test and routine urine cultures were negative. The patient did not improve clinically despite the initiation of empirical first-line antitubercular therapy.
Given the persistent fever despite appropriate antituberculosis treatment, alternative diagnoses were considered. Transthoracic echocardiography was performed to evaluate IE and revealed a small vegetation on the anterior mitral leaflet (Fig. 1). Prolonged blood and urine cultures subsequently yielded rapidly growing NTM after 5 days of incubation (Fig. 2a, b). The relevant laboratory findings are presented in Table 1.
Vegetationat the tip of the anterior mitralleaflet.
Rapid grower nontuberculous mycobacterium (NTM) in (a) urine, and in (b)blood.
Differential diagnosis
Based on the clinical presentation and initial investigations, the differential diagnoses included culture-negative IE, disseminated NTM infection, renal tuberculosis and fungal endocarditis. The lack of response to antituberculosis therapy, echocardiographic evidence of valvular involvement and repeated isolation of rapidly growing NTM supported the diagnosis of NTM-IE.
Management
Following microbiological confirmation, combination antimicrobial therapy was initiated with intravenous amikacin, oral clarithromycin and oral linezolid, and subsequently adjusted in consultation with infectious disease and clinical microbiology specialists, guided by the available culture and susceptibility results. The patient became afebrile after 2 weeks of treatment. Amikacin dosing was subsequently adjusted because of rising serum creatinine levels (peak value, 2.02 mg dl^−1^). After 5 weeks of inpatient treatment, the patient was discharged against medical advice (DAMA) with instructions for close outpatient follow-up and renal function monitoring.
Outcome
Six weeks after discharge, the patient presented with acute-onset chest pain and dyspnoea. Serum troponin I levels were markedly elevated (4,110.25 ng ml^−1^), and electrocardiography showed nonspecific ST-segment changes. He was managed for a non-ST-segment elevation myocardial infarction but deteriorated rapidly and died within 13 h of admission to the coronary care unit. Adherence to antimicrobial therapy during the interim period following discharge could not be determined reliably.
Case 2
Clinical presentation
A 55-year-old woman with long-standing diabetes mellitus and hypertension presented with a 1-month history of intermittent high-grade fever. She had undergone PCI through the right femoral artery for triple-vessel coronary artery disease 2 months before symptom onset. On admission, she was febrile, pale, tachycardic and tachypnoeic, with bilateral basal crepitations on chest auscultation.
Diagnostic work-up
The initial laboratory work-up demonstrated pancytopenia and significantly elevated inflammatory markers (Table 1). An extensive evaluation for infectious and autoimmune aetiologies was performed in view of the persistent fever in a patient with recent healthcare exposure, and all initial investigations were negative. Transthoracic echocardiography was used to screen for IE and showed vegetations on the right and non-coronary cusps of the aortic valve (Fig. 3).
Vegetation of non-coronary cuspNCC of aortic valve. NCC, non-coronarycusp.
Given the echocardiographic appearance and persistent systemic inflammation, prolonged blood cultures were collected and ultimately grew rapidly growing NTM after extended incubation (Fig. 4), using the standard microbiology preparation described above. At this juncture, the differential diagnoses included culture-negative IE, tuberculous endocarditis, disseminated NTM infection and fungal endocarditis. The recovery of fast-growing NTM from blood cultures, along with valvular vegetations, was consistent with the diagnosis of NTM endocarditis.
Sabouraud dextrose agar showing rapidly growing NTM
Management
The patient was started on combination therapy with linezolid, clarithromycin, amikacin and ceftazidime–avibactam. This choice was based on cultural sensitivity and the context of severe sepsis, with the advice of an infectious disease expert. The patient was initially afebrile; however, linezolid was discontinued because of worsening thrombocytopenia, and fever reappeared. Surgical treatment was recommended because of persistent infection despite the use of multiple drugs and echocardiographic findings suggesting active aortic valve disease. Owing to logistic constraints for valve replacement surgery at that time, the patient was referred outside the country.
Outcome
She was haemodynamically stable, with no further deterioration of clinical parameters during transfer until surgery. However, she experienced an unexpected cardiac arrest while undergoing anaesthesia induction for elective aortic valve replacement. She was eventually declared dead in the operating theatre despite aggressive resuscitation efforts.
Case 3
Clinical presentation
A 45-year-old man with hypertension, a college teacher from Barishal, developed an acute myocardial infarction (AMI) and was treated with PCI through the right femoral artery for AMI. He presented with a persistent high-grade fever ~1 month after PCI, which persisted for 5 months before consultation. He reported no weight loss, night sweats, cough or other constitutional symptoms that were consistent with tuberculosis. There was no history of tuberculosis or known contact with any patients with tuberculosis.
Diagnostic work-up
Clinically, the patient appeared pale and febrile. He had splinter haemorrhages on general examination and hepatosplenomegaly on abdominal examination. Laboratory studies were consistent with anaemia, leucopenia and a marked elevation of C-reactive protein levels (Table 1). Due to persistent fever, along with peripheral signs of endocarditis and a history of cardiac procedures, transthoracic echocardiography was performed, which revealed a vegetation attached to the non-coronary cusp of the aortic valve (Fig. 5).
Vegetation attached to non-coronary cusp (NCC) of aortic valve. NCC, non-coronary cusp.
Differential diagnosis
A comprehensive work-up for infectious and autoimmune aetiologies was performed. Tests for tuberculosis, viral infections, connective tissue disease and haematologic malignancy were all negative. Blood cultures were processed using standardized microbiology procedures, as described earlier, and repeatedly produced rapidly growing NTM (Fig. 6).
Blood agar media showing rapidly growing NTM.
Based on the clinical contexts and investigations, culture-negative IE, NTM infection, tuberculosis and haematological malignancy were part of the differential diagnoses. Valvular vegetation, recurrent isolation of rapidly growing NTM from blood cultures and the exclusion of other diagnoses confirmed the diagnosis of NTM-IE involving the native aortic valve.
Management
The patient was started on combination antimicrobial therapy involving amikacin, macrolide and linezolid based on the culture sensitivity of the organism, clinical severity, tolerability and expert opinion. Treatment was complicated by cytopenias and the need for close monitoring of renal function and haematological parameters. Despite antimicrobial therapy, the patient showed progressive clinical deterioration. Surgical intervention was considered; however, definitive surgical planning could not be undertaken because of the advanced disease and rapid clinical decline.
Outcome
The patient continued to deteriorate, with features of progressive IE and a systemic inflammatory response. The patient was DAMA because he was unable to bear the hospital expenses due to financial constraints. During the second month of treatment, he collapsed at home and was brought to a local hospital, where he was declared dead. The cause of death was most likely cardiac decompensation secondary to advanced NTM-related aortic valve IE.
Discussion
Changing epidemiology and risk factors
NTM-IE remains a rare diagnosis but is being reported with increasing frequency owing to the widespread use of intravascular devices and cardiovascular interventions. In the largest systematic review to date (167 patients), rapidly growing species accounted for nearly all native valve infections, and the overall mortality approached 45% [2]. Conservative management without surgery was associated with far poorer survival than combined medical–surgical therapy (mortality, 66.7% versus 30.6%) [2], underscoring the seriousness of these infections. Prosthetic valves were the most common risk factor in that review (63.5% of cases) [2]; however, native valve infections, such as those in our series, have also been linked to rapidly growing mycobacteria. NTM are ubiquitous environmental bacteria. They are classified into rapid-growing species (growth within 7–14 days) and slow-growing species (growth after 14 days) [25]. Outbreak investigations have implicated contaminated water sources, heater-cooler devices, hydrotherapy equipment, intravenous infusions and other invasive procedures as vehicles for transmission [56]. Our three patients developed fever within weeks to months of PCI; although a causal relationship cannot be established, these procedures represent plausible healthcare-associated exposures.
Diagnostic challenges and microbiological considerations
Blood culture negativity and missed diagnosis
NTM-IE frequently presents as blood culture-negative IE (BCNE). BCNE is defined as endocarditis in which three or more aerobic and anaerobic blood cultures remain negative despite prolonged incubation beyond 1 week [7]. Routine blood cultures may be falsely negative in NTM-IE because rapidly growing species can take 7–10 days to appear, and slow-growing species require more than 2 weeks [2]. In our first case, an AFB smear of urine suggested renal tuberculosis, and the patient received standard antitubercular therapy. AFB smears cannot differentiate the M. tuberculosis complex from NTM, and other organisms may stain acid-fast [8]. Only prolonged mycobacterial cultures can detect small numbers of bacilli (up to 8 weeks of incubation), and species-level identification usually requires technologies such as MALDI-TOF mass spectrometry [9]. In the absence of these resources, clinicians should maintain a high index of suspicion for NTM when culture-negative endocarditis follows a recent invasive procedure or when acid-fast organisms are observed.
Contamination control and laboratory reproducibility
Because NTM are ubiquitous in water and soil, repeated isolation is essential to distinguish between infection and contamination. Each of our patients had blood and/or urine cultures repeated on consecutive days; the cultures grew the same rapidly growing NTM, and the isolates were processed at a single reference laboratory using standard protocols, thus minimizing the likelihood of contamination. These findings meet the spirit of the American Thoracic Society (ATS), European Respiratory Society (ERS), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), and Infectious Diseases Society of America (IDSA) guideline recommendation to document more than one positive culture of the same species to confirm the disease [10]. We differentiated NTM from the M. tuberculosis complex using a commercial real-time PCR assay; however, species-level identification and susceptibility testing could not be performed because of resource limitations. The inability to perform MALDI-TOF or sequencing is acknowledged as a major limitation of our report. Nevertheless, repeated isolation from sterile sites, the presence of echocardiographic vegetations and the fatal clinical course in all three cases strongly support true infection rather than contamination.
Therapeutic considerations
Antimicrobial therapy
Evidence-based treatment recommendations for NTM-IE are lacking because most of the experience comes from small case reports and series. The ATS/ERS/ESCMID/IDSA guidelines for NTM pulmonary disease emphasize that treatment should be tailored to the infecting species, extent of disease, drug susceptibility and comorbidities, and that regimens require multiple agents, prolonged courses and careful monitoring for toxicity [10]. Even with appropriate therapy, outcomes remain suboptimal, and reinfection is common [11]. In our series, amikacin and a macrolide (clarithromycin or azithromycin) formed the backbone of therapy, supplemented with linezolid or ceftazidime–avibactam when disease severity or toxicity required. These combinations were empirical and reflected the paucity of standardized regimens; ceftazidime–avibactam was used as salvage therapy in one case of severe sepsis. Drug toxicity was frequent: nephrotoxicity necessitated dose adjustment of amikacin, and thrombocytopenia required the discontinuation of linezolid. These adverse effects underscore the guidelines’ cautioning against prolonged multi-drug therapy [12]. While susceptibility testing would have allowed for more rational regimens, such testing for NTM is often unavailable, especially in resource-limited settings.
Surgical management
Surgical removal of infected tissue remains a cornerstone of IE management, especially when caused by virulent or resistant organisms such as Pseudomonas aeruginosa. General IE guidelines emphasize that once an indication for surgery exists, such as heart failure, large vegetations, persistent bacteraemia or infection with highly resistant organisms, surgery should not be delayed [13]. Expert opinion advocates ‘operate sooner rather than later’ because damaged valves will not recover and tissue destruction will only progress [13]. In a systematic review of NTM-IE, patients managed without surgery had a much higher mortality rate than those who underwent surgery [2]. Rapidly growing NTM form biofilms that are difficult to eradicate and may require debridement [14]. Despite these principles, surgery was either delayed or not performed in our cases because of diagnostic delay, resource constraints and patient choice. One patient died during induction of valve replacement, and the other two deteriorated before surgery could be arranged. These outcomes highlight the need for early recognition and referral to centres capable of combined medical and surgical management.
Association with PCI
Our cases occurred after PCI; however, we cautiously describe the relationship as temporal rather than causal. No procedural breach was documented, and we could not trace a point-source outbreak. Nevertheless, the Centers for Disease Control and Prevention (CDC) notes that NTM can colonize hospital water systems and be disseminated via injections, catheter flushes, hydrotherapy equipment and medical devices [1516]. The time lag between PCI and the onset of fever (1–5 months) suggests latent contamination, as evident by other healthcare exposures [17]. Therefore, clinicians should consider NTM-IE in any post-procedural patient with persistent fever and negative routine cultures, particularly in settings with limited infection-control infrastructure. In all our three patients, the PCI procedures were uneventful.
Outcomes
Recent evidence shows that NTM-IE is a rare but highly lethal disease. In a systematic review of 167 reported cases, 84% of patients had disseminated NTM infection, and the overall mortality approached 45%; mortality was much higher among patients managed medically (66.7%) than among those who underwent combined medical and surgical treatment (30.6%) [2]. Early series of prosthetic valve endocarditis caused by rapidly growing NTM reported mortality rates nearing 88% [18], although more recent case series using aggressive surgical intervention reduced overall mortality to ~23% [18]. These data underscore that invasive NTM infections often require early suspicion, prolonged multi-drug therapy guided by susceptibility testing and timely surgical or device-removal interventions to improve survival [218]. All three patients in our series died despite careful medical treatment. High mortality in NTM-IE is consistently reported and may reflect diagnostic delay, advanced disease at presentation, drug toxicity and lack of timely surgery.
This study has several important limitations. First, species-level identification of the NTM isolates could not be performed because advanced diagnostic platforms such as MALDI-TOF mass spectrometry or gene sequencing were unavailable, precluding organism-specific therapeutic optimization. Second, comprehensive molecular sequencing was not performed, which limited phylogenetic characterization and comparison with previously reported strains. Third, the antimicrobial regimens were heterogeneous and individualized, reflecting differences in clinical severity, drug tolerance and resource availability rather than standardized, evidence-based protocols. Fourth, we did not conduct a formal procedural audit or environmental investigation of catheterization laboratory practices to evaluate the possibility of point-source contamination or infection-control breaches. Finally, all cases occurred after recent PCI and provided a temporal rather than causal association; we cannot conclude that the procedures caused the infections. Nevertheless, detailed clinical histories, prolonged culture incubation, repeated isolations and NTM-PCR confirmation using standardized laboratory methodologies can significantly characterize this rare entity.
Conclusions
This case series highlights the diagnostic complexity and high mortality associated with NTM-IE. Persistent fever after invasive cardiovascular procedures or prolonged, culture-negative endocarditis should prompt consideration of NTM infection. Medical therapy alone is frequently inadequate in NTM-IE, according to most studies, and a combined medical–surgical approach may be required in selected patients, despite inadequate evidence about when and which patients should be operated on.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bouchiat C Saison J Boisset S Flandrois J-P Issartel B et al Nontuberculous mycobacteria: an underestimated cause of bioprosthetic valve infective endocarditis Open Forum Infect Dis 20152 ofv 04710.1093/ofid/ofv 04726213691 PMC 4511745 · doi ↗ · pubmed ↗
- 2Meena DS Kumar D Bohra GK Midha N Garg MK Nontuberculous mycobacterial infective endocarditis: a systematic review of clinical characteristics and outcomes Open Forum Infect Dis 202411 ofae 68810.1093/ofid/ofae 68839660020 PMC 11629984 · doi ↗ · pubmed ↗
- 3Brown-Elliott BA Nash KA Wallace RJ Jr Antimicrobial susceptibility testing, drug resistance mechanisms, and therapy of infections with nontuberculous mycobacteria Clin Microbiol Rev 20122554558210.1128/CMR.05030-1122763637 PMC 3416486 · doi ↗ · pubmed ↗
- 4Clinical and Laboratory Standards Institute (CLSI) Susceptibility Testing of Mycobacteria, Nocardia Spp., and Other Aerobic Actinomycetes, 3rd ed Wayne (PA): CLSICLSI standard M 24201831339680 · pubmed ↗
- 5Mercaldo RA Marshall JE Cangelosi GA Donohue M Falkinham JOIII et al Environmental risk of nontuberculous mycobacterial infection: strategies for advancing methodology Tuberculosis 202313910230510.1016/j.tube.2023.10230536706504 PMC 10023322 · doi ↗ · pubmed ↗
- 6Sommerstein R Rüegg C Kohler P Bloemberg G Kuster SP et al Transmission of Mycobacterium chimaera from heater-cooler units during cardiac surgery despite an ultraclean air ventilation system Emerg Infect Dis 2016221008101310.3201/eid 2206.16004527070958 PMC 4880077 · doi ↗ · pubmed ↗
- 7Mc Hugh J Saleh OA Updates in culture-negative endocarditis Pathogens 202312102710.3390/pathogens 1208102737623987 PMC 10459830 · doi ↗ · pubmed ↗
- 8Desikan P Tiwari K Panwalkar N Khaliq S Chourey M et al Public health relevance of non-tuberculous mycobacteria among AFB positive sputa Germs 20177101810.18683/germs.2017.110328331837 PMC 5348212 · doi ↗ · pubmed ↗