Rapunzel Syndrome in a Pediatric Female Patient: A Case Report of Trichobezoar Causing Intestinal Obstruction
Ali T Alamer, Osama Kattih, Ahmed A Al-Amoudi, Husain A Althani, Abdulaziz J Almarzooq

TL;DR
A six-year-old girl with no psychiatric history was diagnosed with Rapunzel syndrome, a rare condition involving a hair mass causing intestinal blockage, highlighting the need for early recognition in children.
Contribution
This case report increases awareness of Rapunzel syndrome in children without psychiatric backgrounds and emphasizes early diagnosis and treatment.
Findings
A six-year-old girl was diagnosed with Rapunzel syndrome despite having no psychiatric history.
Endoscopic removal of the trichobezoar failed, requiring surgical intervention.
The case underscores the importance of early recognition to prevent complications.
Abstract
Rapunzel syndrome is a very rare type of trichobezoar in which a hair mass extends to the stomach and small intestine forming a body and tail. It usually affects young females with a psychiatric background. Symptoms are usually nonspecific and often delay the diagnosis. We present in this report a case of a six-year-old previously healthy girl who presented with two months of intermittent abdominal pain, vomiting, and constipation. Initial laboratory tests and two times abdominal ultrasounds were unremarkable. Abdominal X-ray showed moderate dilatation of the bowel. Further physical examination revealed patchy scalp alopecia, raising suspicion for hair ingestion. Upper endoscopy showed a large trichobezoar in the stomach and duodenum, but endoscopic removal failed. The patient underwent open laparotomy, and an 11 × 4 cm bezoar with a tail extending into the duodenum was removed. This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
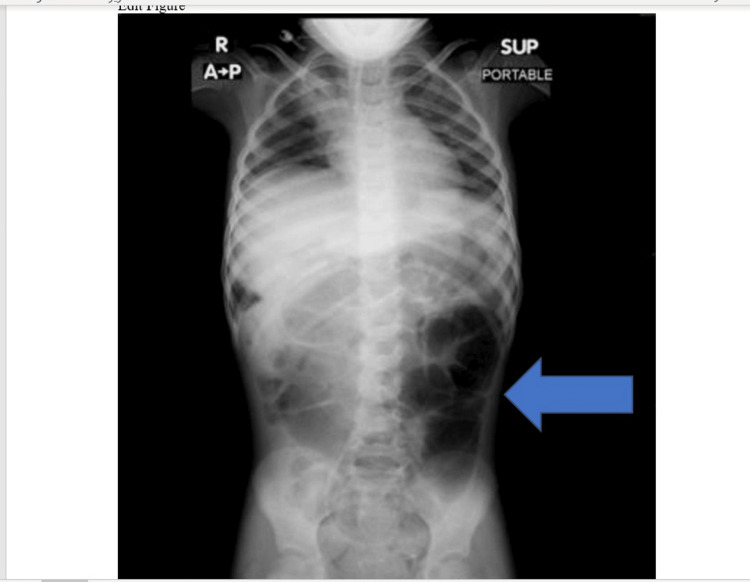 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3| Test | Result | Reference value |
| WBC | 6.5x103/uL | 5-15.5x103/uL |
| Hemoglobin | 12.8 g/dL | 11.5-15.5 g/dL |
| Platelets | 250x103/uL | 150-350x103/uL |
| AST | 30 U/L | 21-44 U/L |
| ALT | 22 U/L | 9-25 U/L |
| Na | 139 mEq/L | 135-145 mEq/L |
| K | 4.2 mEq/L | 3.5-5 mEq/L |
| Ferrtin | 18 Ng/mL | 14-79 Ng/mL |
| TIBC | 380 mcg/dL | 250-400 mcg/dL |
| Iron | 45 mcg/dL | 16-128 mcg/dL |
| Glucose | 88 mg/dL | 70-140 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal and Peritoneal Adhesions · Kidney Stones and Urolithiasis Treatments · Omental and Epiploic Conditions
Introduction
Bezoar is derived from the Persian word “Padzahr,” which means antidotes, as they believed historically that some materials from plants or animals have anti-poison effects. However, in recent medical terminology, bezoar means an accumulation of ingested materials that are insoluble or indigestible in the gastrointestinal tract [1-7].
Rapunzel syndrome is an extremely rare and unusual form of gastric trichobezoar, characterized by the accumulation of hair in the stomach, which may extend into the small intestine and reach the ileum, forming a Bezoar with a tail [1]. It usually affects children and adolescents, specifically females with a history of psychiatric disorders such as hair-pulling (trichotillomania) and hair-eating (trichophagia), or children with trisomy 21 [2]. The clinical presentation of Rapunzel syndrome is usually vague gastrointestinal symptoms such as generalized abdominal pain, nausea, vomiting, weight loss, or the presence of a palpable abdominal mass [3]. Most of the time, diagnosis is delayed or missed, and many patients are diagnosed when there is a clinical suspicion or when the trichobezoar becomes large enough to cause gastric or intestinal obstruction [4]. Complications of untreated Rapunzel syndrome include gastric or small bowel obstruction, gastric ulcers, perforation, gastrointestinal bleeding, and anemia [5]. Early recognition and interventions, including behavioral therapy, are crucial to avoid complications and surgical intervention [6].
Here, we report a case of Rapunzel syndrome in a six-year-old female patient previously healthy, who presented with vague abdominal pain and vomiting, with no previous psychiatric history, emphasizing the importance of clinical suspicion even when psychiatric history is absent. We talk over diagnostic challenges, surgical and non-surgical management, including dietary and psychiatric follow-up.
This study aims to describe a rare presentation of Rapunzel syndrome in order to increase awareness among physicians and emphasize the importance of early recognition and treatment to prevent serious complications.
Case presentation
A six-year-old previously healthy female patient presented to the pediatrics ER with a history of recurrent generalized abdominal pain for around two months, associated with vomiting containing gastric contents and constipation for three weeks. Two previous abdominal ultrasounds were done and were unremarkable.
On examination, the patient was conscious, alert, active, not jaundiced or pale, with no signs of dehydration or respiratory distress. Weight and height were within the 50th percentile. Abdominal examination was unremarkable with no palpable mass. Initial laboratory tests are shown in Table 1.
Stool culture for bacterial pathogens was negative, and stool was negative for viral agents, ova, and parasites. Fecal blood occult was negative.
Upon PICU admission, an abdominal X-ray was done and showed moderate dilation of the bowels (Figure 1). Abdominal ultrasound was repeated as normal.
Abdominal X-ray shows moderate dilatation of bowelsAntero-posterior erect abdominal X-ray showing moderate dilatation of bowels as shown by the arrow.
On detailed physical examination, patches of alopecia were seen on the head, which raised the suspicion of foreign body ingestion. As per the recommendations of the gastrointestinal consultant, the patient underwent upper gastrointestinal endoscopy. A mass of hair was found in the stomach and duodenum, but could not be removed by endoscopy. Upon surgical consultation while the patient was in the operation room, laparotomy was recommended to remove the hair mass. After open laparotomy, a mass of hair was removed from the stomach and duodenum, measuring around 11 cm x 4 cm bezoar specimen showing tail (Figures 2-3).
11 cm x 4 cm trichobezoar specimen showing tail.
11 cm x 4 cm trichobezoar specimen showing tail.
One day later, the patient was discharged home with a psychiatry appointment for further management to prevent recurrence.
Discussion
Ingestion of hair leads to the formation of a trichobezoar in the stomach because hair is indigestible and resistant to bowel peristalsis. Over time, it accumulates and forms a solid mass; when the mass extends beyond the stomach into the small bowel, the condition is termed Rapunzel syndrome [1,2]. Although bezoars of different kinds are common, trichobezoars represent a minority of all human bezoars. Rapunzel syndrome is extremely rare, with less than 100 cases reported and published worldwide [1,3]. Rapunzel syndrome usually presents with non-specific GI symptoms, generalized abdominal pain, vomiting, weight loss, signs of obstruction such as constipation or a palpable abdominal mass, and sometimes nutritional deficiencies [3-6]. Because symptoms are vague and often chronic, suspicion may be low; thus, imaging (ultrasound, CT) and/or endoscopy are needed to establish a diagnosis [3-6]. Endoscopic removal may be enough for small trichobezoars; however, in numerous cases, especially in those with large bezoars expanding into the small bowel, surgical intervention such as laparotomy is needed [3-6]. After management, nutritional support and psychiatric counselling are critical to prevent recurrence [5,6].
Conclusions
Even though Rapunzel syndrome is extremely rare, it should be considered as a differential diagnosis of young female patients, specifically if they have a psychiatric background presenting with chronic nonspecific gastrointestinal symptoms, weight loss, or a palpable abdominal mass, even in the absence of a clear history of hair-pulling or witnessed hair-eating by family. Early confirmation of diagnosis using imaging and endoscopy, followed by rapid surgical removal with good psychiatric intervention, is crucial to reduce life-threatening complications and prevent recurrence. Reporting of such cases remains important to boost awareness among physicians and improve early management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rapunzel syndrome J Ayub Med Coll Abbottabad Ahmed Bashir E Samiullah Samiullah Attique Sadiq M Yusuf O Khan K 218220222010 http://www.ayubmed.edu.pk/JAMC/PAST/22-4/Eitezaz.pdf 22455302 · pubmed ↗
- 2Every tangle has a story - Rapunzel syndrome: a case report J Pediatr Adolesc Surg Aziz Khan Y Zaib Z Tufail F Rafiq K Muhammad K 10911122024
- 3Rapunzel syndrome Saudi Med J Al-Wadan AH Al-Absi M Al-Saadi AS Abdoulgafour M 19121914272006 https://pubmed.ncbi.nlm.nih.gov/17143376/17143376 · pubmed ↗
- 4Rapunzel syndrome: a review of unusual case Int Surg J Modh FA 3764376652018
- 5Rapunzel syndrome in a 7-year-old boy: a case report Int J Surg Sci Vora S Godhani C Patel S 52953232019
- 6Rapunzel syndrome: an infrequent cause of severe iron deficiency anemia and abdominal pain presenting to the pediatric emergency department BMC Pediatr Cannalire G Conti L Celoni M 1251820182961498610.1186/s 12887-018-1097-8PMC 5883293 · doi ↗ · pubmed ↗
- 7Gastric trichobezoar: case report and literature review Mayo Clin Proc Phillips MR Zaheer S Drugas GT 653656731998966319410.1016/S 0025-6196(11)64889-1 · doi ↗ · pubmed ↗