Effect of glucagon-like peptide-1 receptor agonists on heart rate in non-diabetic individuals with overweight or obesity: a systematic review and pairwise and network meta-analysis of randomized controlled trials
Yiwen Zhang, Chuying Zhang, Xuyang Gong, Panpan Cheng, Hang Fu, Linqi Diao, Chunhua Song

TL;DR
This study finds that GLP-1 receptor agonists increase heart rate in non-diabetic individuals with overweight or obesity, with some drugs causing larger increases than others.
Contribution
The study is the first to systematically review and meta-analyze the effect of GLP-1RAs on heart rate in non-diabetic overweight or obese individuals.
Findings
GLP-1 receptor agonists significantly increase heart rate compared to placebo.
Orforglipron 36 mg causes the largest heart rate increase, while tirzepatide 5 mg causes the smallest.
Network meta-analysis confirms variability in heart rate effects across different GLP-1RA drugs.
Abstract
To explore the association of glucagon-like peptide-1 receptor agonists (GLP-1RAs) on heart rate (HR) in overweight or obese patients without diabetes. A comprehensive search of the PubMed, Web of Science, Embase, and Cochrane Library databases was conducted. Mean differences (MDs) were calculated as effect estimates for HR. Pairwise and network meta-analysis were conducted. Twelve articles were included. Pairwise meta-analysis showed significant association of increase compared with placebo in liraglutide [MD 2.37, 95% confidence interval (CI) 1.86, 2.89], semaglutide (MD = 3.35; 95% CI 1.69, 5.01), orforglipron (MD = 7.30; 95% CI 5.48, 9.12), oral semaglutide (MD = 4.50; 95% CI 3.11, 5.89), tirzepatide (MD = 2.05; 95% CI 0.96, 3.13), retatrutide (MD = 3.46; 95% CI 1.74, 5.18), and total GLP-1RAs (MD = 3.47; 95% CI 2.65, 4.29). Network meta-analysis revealed that orforglipron 36 mg…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
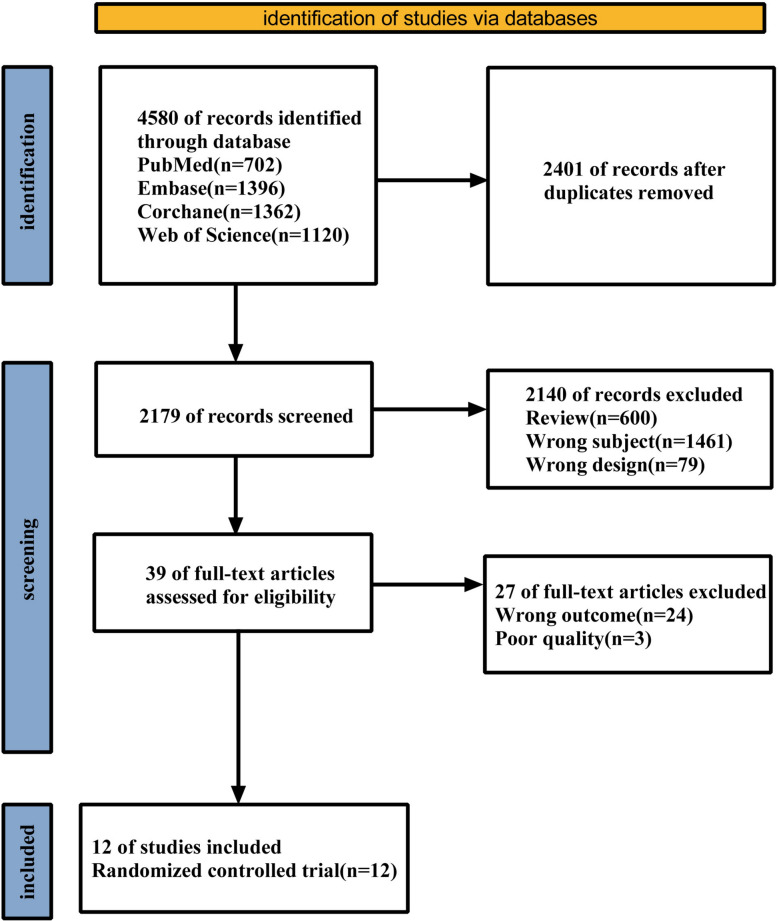 Figure 1
Figure 1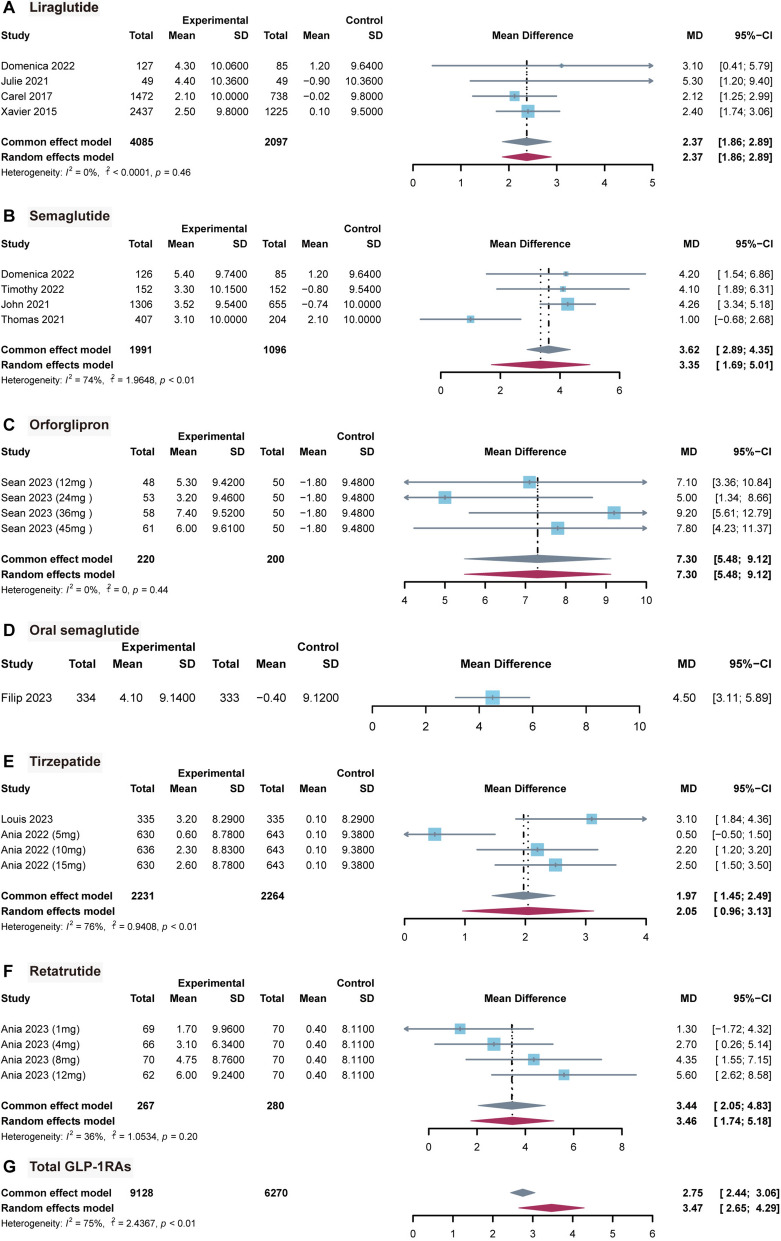 Figure 2
Figure 2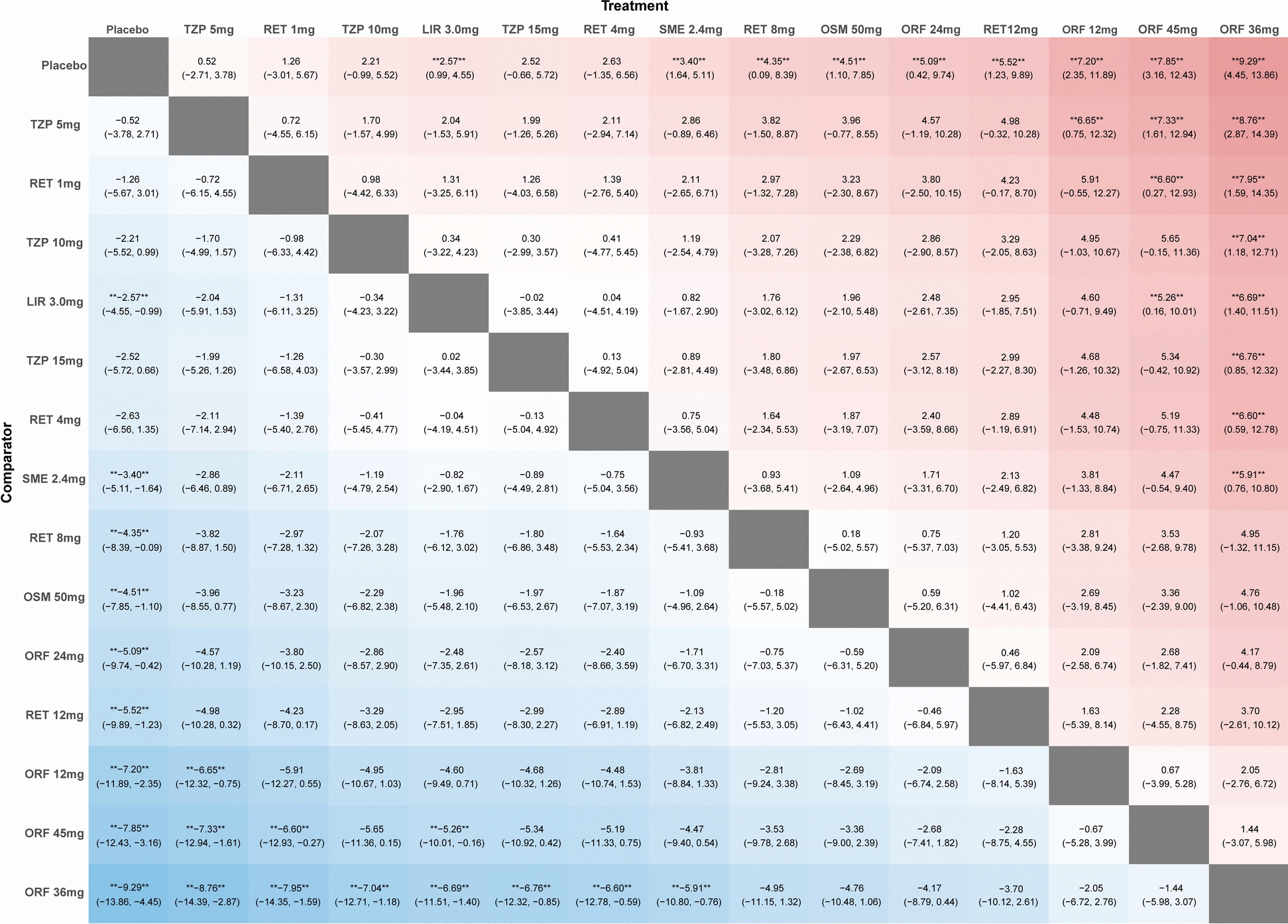 Figure 3
Figure 3- —Henan Province’s Young and Middle-aged Academic Leaders Training Program for Health Care Sciences
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart rate and cardiovascular health · Diabetes Treatment and Management · Heart Failure Treatment and Management
Introduction
Obesity is a critical global public-health concern as it is associated with a broad spectrum of serious comorbidities, including diabetes, hypertension, dyslipidemia, cardiovascular disease, and cancer [1, 2]. Over the past few decades, the global prevalence of obesity has gradually increased, and this trend is projected to persist [3]. Dietary and exercise control are insufficient to address the obesity epidemic [4, 5], prompting the development of a wide range of pharmacotherapies for weight management [6, 7]. Among these agents, glucagon-like peptide-1 receptor agonists (GLP-1RAs) have emerged as the particularly promising class, exhibiting robust weight loss effects [8, 9].
However, the marked therapeutic benefits of GLP-1RAs are often accompanied by significant adverse effects that may lead to treatment discontinuation and, in some cases, serious clinical consequences [10]. Thus, a comprehensive understanding of these side effects is essential to facilitate precise medicine in obesity management. Previous work has indicated that the use of GLP-1RAs in Type 2 diabetes mellitus (T2DM) was usually accompanied by an increased heart rate (HR) [11, 12]. Elevated resting HR is a well-established risk factor for adverse cardiovascular events [13]. In addition, a negative correlation has been observed between HR and survival in the general population and patients with cardiovascular disease [14]. While several investigations have evaluated the effects of GLP-1RAs on HR, few have focused specifically on populations with obesity. These studies are also limited to a single drug and lack systematic synthesis of HR data or direct comparisons among different GLP-1RAs [15, 16]. Meanwhile, although GLP-1RAs could significantly increase HR, some evidence shows that liraglutide (LIR) does not raise HR during acute myocardial infarction [17, 18]. Overall, evidence regarding the impact of GLP-1RAs on HR in patients with obesity remains limited and inconsistent. Nevertheless, clarifying the magnitude and variability of HR effects across different GLP-1RAs is of paramount importance, as it enables accurate medication selection for patients who cannot tolerate HR elevation.
In the present study, we performed paired and network meta-analyses to thoroughly evaluate the impact of GLP-1RAs on HR in patients with obesity by comprehensively searching and synthesizing the latest clinical trial evidence. The findings of this study were intended to provide critical evidence for the rational use of GLP-1RAs and inform clinical decision-making in obesity management.
Materials and methods
Pairwise and network meta-analysis were conducted in adherence to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [19, 20] and prospectively registered (PROSPERO ID: CRD42024537690).
Search strategy and study selection
Publications were retrieved from PubMed, Embase, Web of Science, and the Cochrane Library from database inception to July 31, 2025. In addition, manual searches of relevant journals and ClinicalTrials.gov were conducted within the same time frame. The databases were searched using the following Medical Subject Headings (MeSH) terms or keywords: (1) glucagon-like peptide-1 receptor agonist AND (2) randomized OR controlled trial randomized AND (3) overweight or obesity. Two independent reviewers (Z.Y.W and Z.C.Y) searched the databases and screened the titles, abstracts, and full-text articles to select the studies. Discrepancies during the screening process were resolved through consultation with other members of the research team. The complete search strategy is detailed in Table S1.
Inclusion and exclusion criteria
Studies that reported data on HR in research on GLP-1RAs were included. The study population was restricted to overweight or obese patients without diabetes. We included only randomized controlled trials (RCTs) of at least 26 weeks that compared GLP-1RAs with another GLP-1RAs or placebo. Studies were excluded if they involved patients of age under 18 years, with a history of renal, hepatic failures, or other serious diseases. Moreover, phase I studies, secondary analyses, and unpublished data were not used. Two independent reviewers (Z.Y.W and Z.C.Y) evaluated the eligibility of studies for inclusion in the analysis. Disagreements were discussed with other team members until consensus was reached to include only those articles that best met the criteria.
Outcome definitions
The only outcome of this systematic review and meta-analysis was the change in HR from baseline to the study endpoint.
Quality assessment
The Cochrane Risk of Bias Tool, version 2, for randomized trials was used to assess the overall risk of bias [21]. Trials with all domains at low risk of bias were considered to have an overall low risk of bias, whereas trials with at least one domain at high risk of bias were considered to have an overall high risk of bias. Quality assessment was performed by two independent reviewers (C.P.P. and G.X.Y), and disagreements were resolved by consensus.
Data extraction
Data extraction was performed by two independent reviewers (Z.Y.W and Z.C.Y), and the extracted content included the following: study details including author(s), publication year, study design, sample size; population characteristics including patients, age, gender, body weight, body mass index, waist circumference, baseline HR, and inclusion/exclusion criteria; intervention and comparison including types of GLP-1RAs, oral or injectable medications; and outcome indicators, primarily changes in HR from baseline.
Data synthesis
The mean and standard deviation (SD) of baseline and post-intervention HR were extracted from each study for the intervention and control groups. Some trials reported multiple time-point results, but only the most recent time point was extracted for analysis. When the SD of HR variability was not provided directly, the SD of the mean group was calculated using the formulas in the Cochrane Handbook chapter based on the standard error of the mean (SEM) or 95% CI (SD = SEM * \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\sqrt{{\boldsymbol{n}}}$$\end{document} or SD = \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\sqrt{{\boldsymbol{n}}}$$\end{document} * (upper limit − lower limit)/3.92) [22]. When not reported, change from baseline SDs were estimated using the equation from the Cochrane Handbook chapter, assuming a correlation coefficient of 0.50 between baseline and post-intervention HR ( \documentclass[12pt]{minimal} \usepackage{amsmath} \usepackage{wasysym} \usepackage{amsfonts} \usepackage{amssymb} \usepackage{amsbsy} \usepackage{mathrsfs} \usepackage{upgreek} \setlength{\oddsidemargin}{-69pt} \begin{document}$$\sqrt{{SD}_{baseline}^{2}+{SD}_{final}^{2}-2*0.5*{SD}_{baseline}{* SD}_{final}}$$\end{document} ) [23, 24].
Conventional pairwise meta-analyses were pooled using a random-effect model comparing means with their SDs. The Higgins I^2^ was used to assess statistical heterogeneity between studies; an I^2^ statistic of > 50% was considered significant heterogeneity, and a value of < 50% was considered acceptable. Subgroup analyses were performed based on different medications and population characteristics. In all cases, a two-tailed p value < 0.05 was deemed statistically significant for all analyses.
A network meta-analysis was conducted using Bayesian methods to evaluate the relative effects of treatment on HR for each study group. This approach synthesizes all available evidence, including both direct and indirect comparisons, when a connected evidence network exists. Point estimates and 95% confidence intervals (CIs) were assessed using the Markov chain Monte Carlo method with a random-effect model, and 95% CIs excluding 0 were considered significant. A network plot of all interventions was made to identify possible direct and indirect comparisons. Ranking probabilities for all inventions were estimated using the surface under the cumulative ranking curve (SUCRA) and mean ranks to rank the effect of each invention. Forest plots (versus placebo) and league tables were generated to visually present the results of the network meta-analysis [25]. Subgroup analyses were conducted to explore potential sources of heterogeneity in HR responses to GLP-1RAs. These exploratory analyses included stratification by formulation, dosing frequency, number of activated channels, treatment duration, age and baseline heart rate. Publication bias was assessed by visual inspection of the Begg’s funnel plots and Egger’s asymmetry test. Sensitivity analyses were conducted by comparing fixed effects with random effects and randomly deleting a reference to assess the stability of the result. A p value greater than 0.05 indicated that inconsistency was not evident.
All statistical analyses in this study were performed in this study using R version 4.5.2 (http://www.r-project.org/) with the BUGSnet, netmeta, and gemtc packages [26, 27].
Results
Study selection and characteristics
The PRISMA flowchart of the included studies is shown in Fig. 1. A total of 4580 studies were initially retrieved from four databases. After excluding studies that did not meet the criteria or were repeated, 12 RCTs were included. Among them, 10 were phase 3 controlled clinical trials and 2 were phase 2 controlled trials. The study duration was 36–160 weeks. Three studies were treated with semaglutide (SME) [28–30], three with LIR [31–33], one with SME or LIR [34], one with oral semaglutide (OSM) [35], one with orforglipron (ORF) [36], two with tirzepatide (TZP) [37, 38] and one with retatrutide (RET) [39]. A total of 15 313 patients were included, 9 128 in the GLP-1RAs group and 6 185 in the control group. The mean baseline HR was observed to range from 69.0 bpm to 74.0 bpm, and the changes in HR from baseline exhibited a range of 0.6 bpm to 7.4 bpm. The detailed characteristics of the included studies are shown in Table 1. In addition, concomitant medications were permitted to be used in all studies and the detailed medication requirements in the experiment are shown in Table S2.Fig. 1PRISMA flowchart of the included studies.Table 1. Characteristics of included studiesStudy, First author yearClinicalTrials.gov IdentifierStudy phaseStudy armSample sizeStudy duration, weeksAge, yearsMale, %BMI, kg/m^2^Waist circumference, cmBaseline HR, bpm Mean ± SDHR change from basine, bpm Mean ± SDLouis 2024NCT04660643IIITZP 10 or 15 mg335884999(30)38.4107.3 ± 22.372.0 ± 9.03.2 ± 8.29Placebo3354898(30)0.1 ± 8.29Sean 2023NCT05051579IIORF 12 mg503649.819(38)37.7114.4 ± 16.573.9 ± 9.15.3 ± 9.42ORF 24 mg535723(43)38.1120.1 ± 19.171.9 ± 12.13.2 ± 9.46ORF 36 mg5855.911(38)38117.3 ± 15.569.4 ± 9.37.4 ± 9.52ORF 45 mg6153.726(43)37.8116.9 ± 13.869.8 ± 10.06.0 ± 9.61Placebo505421(42)37.8115.5 ± 15.469.6 ± 10.6− 1.8 ± 9.48Filip 2023NCT05035095IIIOSM 50 mg334684987(26)37.3112.6 ± 13.671.0 ± 10.04.1 ± 9.14Placebo3335095(29)37.7114.5 ± 15.472.0 ± 10.0− 0.4 ± 9.12Ania 2023NCT04881760IIRET 1 mg694850.636(52)37.5114.8 ± 14.771.1 ± 11.21.7 ± 9.96RET 4 mg6748.835(52)37.4116.2 ± 15.469.9 ± 10.73.1 ± 6.34RET 8 mg7047.436(51)37.2114.5 ± 13.570.6 ± 10.14.8 ± 8.76RET 12 mg6245.832(52)37.4116.5 ± 16.469.3 ± 9.26.0 ± 9.24Placebo704836(51)37.3115.1 ± 13.974.0 ± 10.70.4 ± 8.11Domenica 2022NCT04074161IIISME 2.4 mg126684824 (19)37111.8 ± 16.371.0 ± 9.05.4 ± 9.74LIR 3.0 mg1274930 (24)37.2113.5 ± 15.071.0 ± 10.04.3 ± 10.06Placebo855119 (22)38.8115.4 ± 15.172.0 ± 10.01.2 ± 9.64Ania 2022NCT04184622IIITZP 5 mg6307245.6204(32)37.4113.2 ± 14.372.3 ± 9.60.6 ± 8.78TZP 10 mg63644.7209(33)38.2114.8 ± 15.871.8 ± 9.62.3 ± 8.83TZP 15 mg63044.9205(33)38.1114.4 ± 15.672.5 ± 10.02.6 ± 8.78Placebo64344.4207(32)38.2114.0 ± 14.972.9 ± 9.30.1 ± 9.38Timothy 2022NCT03693430IIISME 2.4 mg15210447.329 (19)38.6115.8 ± 14.373.0 ± 11.03.3 ± 10.15Placebo15247.439 (26)38.5115.7 ± 15.572.0 ± 9.0− 0.8 ± 9.54John 2021NCT03548935IIISME 2.4 mg13066846351(27)37.8114.6 ± 14.872.0 ± 10.03.5 ± 9.54Placebo65547156(24)38114.8 ± 14.472.0 ± 10.0− 0.7 ± 10.00Thomas 2021NCT03611582IIISME 2.4 mg407684692 (23)38.1113.6 ± 15.171.0 ± 10.03.1 ± 10.00Placebo2044624 (12)37.8111.8 ± 16.271.0 ± 10.02.1 ± 10.00Julie 2021NCT04122716IIILIR 3.0 mg495243–32.6100.3 ± 10.069.0 ± 12.04.4 ± 10.36Placebo49–− 0.9 ± 10.36Carel 2017NCT01272219IIILIR 3.0 mg147216047.5364(24)38.8116.5 ± 14.4–2.1 ± 10.00Placebo73847.3176(23)39116.7 ± 13.9–− 0.02 ± 9.80Xavier 2015NCT01272219IIILIR 3.0 mg24875645.2530(21)38.3115.0 ± 14.4–2.5 ± 9.80Placebo122445273(22)38.3114.5 ± 14.3–0.1 ± 9.50BMI: body mass index; HR: heart rate; bpm: beats per minute; SD: standard deviation; TZP: tirzepatide; ORF: orforglipron; OSM: oral semaglutide; RET: retatrutide; SME: semaglutide; LIR: liraglutide
Risk-of-bias analysis
The risk of bias of the included RCTs is presented in Figure S1. Among these RCTs, three studies may have a certain impact on outcome events due to loss to follow-up, two may not have been double blind, and the other biases were low in all studies. In general, these studies had a low or moderate level of risk.
Pairwise meta-analysis
Twelve articles were included in the pairwise meta-analysis. Six study were summarized from original research [LIR, SME, ORF, OSM, TZP, and RET]. Overall, the results indicated a statistically significant association between GLP-1RAs and increased HR when compared with placebo [median deviation, (MD) = 3.47; 95% CI 2.65, 4.29; Fig. 2G]. Specifically, a statistically significant association between LIR use and elevated HR was observed with a relatively smaller magnitude (MD = 2.37; 95% CI 1.86, 2.89; Fig. 2A), as well as similar associations in SME (MD = 3.35; 95% CI 1.69, 5.01; Fig. 2B) and TZP (MD = 2.05; 95% CI 0.96, 3.13; Fig. 2E). For ORF and RET, pronounced statistically significant associations with greater HR elevation were identified (MD = 7.30; 95% CI 5.48, 9.12, Fig. 2C; MD = 3.46; 95% CI 1.74, 5.18; Fig. 2F). In addition, one study reported HR data for OSM with a combined association indicating elevated HR (MD = 4.50; 95% CI 3.11, 5.89; Fig. 2D).Fig. 2. Forest plots for pairwise meta-analysis. GLP-1 RAs: glucagon-like peptide-1 receptor agonists; MD: mean difference
Network meta-analysis
Eleven studies were included in this network meta-analysis (one study was excluded because of unclear TZP dosage). Network plots of all outcomes are illustrated in Figure S2. Compared with placebo, TZP 5 mg (MD = 0.52; 95% CI − 2.71, 3.78), TZP 10 mg (MD = 2.21; 95% CI − 0.99, 5.52), TZP 15 mg (MD = 2.52; 95% CI − 0.66, 5.72), SME 2.4 mg (MD = 3.40; 95% CI 1.64, 5.11), LIR 3.0 mg (MD = 2.57; 95% CI 0.99, 4.55), RET 1 mg (MD = 1.26; 95% CI − 3.01, 5.67), and RET 4 mg (MD = 2.63; 95% CI − 1.35, 6.56) were associated with weaker magnitude of HR elevation. In addition, RET 8 mg (MD = 4.35; 95% CI 0.09, 8.39), RET 12 mg (MD = 5.52; 95% CI 1.23, 9.89), OSM 50 mg (MD = 4.51; 95% CI 1.10, 7.85), ORF 12 mg (MD = 7.20; 95% CI 2.35, 11.89), ORF 24 mg (MD = 5.09; 95% CI 0.42, 9.74), ORF 36 mg (MD = 9.29; 95% CI 4.45, 13.86), and ORF 45 mg (MD = 7.85; 95% CI 3.16, 12.43) showed more pronounced associations with HR elevation. More detailed information can be found in Figs. 3 and S3. When all drugs were ranked based on their observed associations with HR, ORF 36 mg was linked to the greatest magnitude of HR increasing and TZP 5 mg was associated the minimum. The detailed SUCRA is in Figure S4, and no evidence of inconsistency was found in this network analysis (Figure S5).Fig. 3. League table for network meta-analysis. TZP: tirzepatide; ORF: orforglipron; OSM: oral semaglutide; RET: retatrutide; SME: semaglutide; LIR: liraglutide
Subgroup analysis
We conducted subgroup analyses to explore potential associations between different medications, population characteristics and HR changes. Exploratory findings suggested that oral medication may be associated with a greater increase compared to hypodermic injection medication (Figure S6). Similarly, medication once a week may be linked to greater relative to medication once a day (Figure S7). We observed that single-channel activation was associated with a greater increase in heart rate (Figure S8). Furthermore, results indicated potential relationships that longer treatment duration, younger patient age, and lower baseline HR were each linked to a smaller magnitude of HR elevation (Figures S9–11).
Sensitivity analysis and publication bias
For each incorporation effect, we simultaneously applied fixed effects, and the results (Fig. 2) were similar to random effects. We also randomly deleted one study, and the results did not change significantly (Figure S12). These findings indicated that our results were stable. Funnel plots of pairwise and network meta-analyses were visually symmetrical (Figures S13, 14). Egger's test showed the total GLP-1RAs group may have some publication bias (Table S3).
Discussion
This pairwise and network meta-analysis comprehensively evaluated and compared the effect of six GLP-1RAs on HR in obese adults, encompassing three novel drugs (ORF, RET, and TZP). Our pooled data analysis, based on high-confidence estimates, demonstrated that all GLP-1RAs were significantly associated with elevated HR. In terms of the associations between individual GLP-1RAs and HR elevation, ORF was linked to the most magnitude of increasing HR, whereas TZP was associated with the least. A potential dose-dependent pattern was apparent. The 36 mg dose of ORF was correlated with the most pronounced HR increase and the 5 mg dose of TZP was linked to the minimum. Furthermore, our findings suggested that oral and long-acting GLP-1RAs may be associated with a more substantial increase. In addition, a trend was identified, wherein the association between heart-rate-increasing and these drugs diminished over the course of treatment.
The precise mechanism underlying GLP-1RA-induced HR elevation remains incompletely understood, though several potential explanations have been proposed. The GLP-1 receptor is directly expressed in human cardiac sinus node cells, and GLP-1RAs activate this receptor to mediate an increased HR [40, 41]. This is corroborated by clinical studies conducted on patients with T2DM [42]. Nevertheless, the isolated atrial GLP-1R does not exert a direct chronotropic effect upon exposure to GLP-1RAs in intact hearts [43]. This finding indicates that the rise in HR is at least partially attributable to an increase in central or local sympathetic nervous system activity or to a reduction in parasympathetic nervous system inputs [44]. Recent studies show that GLP-1RAs may regulate HR via preproglucagon neurons in the nucleus tractus solitarius [45]. This increase in HR has also been previously postulated to be a compensatory response to the decrease in blood pressure caused by vasodilation induced by GLP-1 [41]. However, in a head-to-head study, no significant correlation was found between blood pressure and HR [46]. GLP-1RAs have been demonstrated as well to decrease HR variability while simultaneously increasing HR [11]. Interestingly, although a substantial body of evidence indicates that elevated HR is an independent risk factor for cardiovascular events and mortality [13], a number of clinical studies and meta-analyses have demonstrated that the utilization of GLP-1RAs is associated with reduced incidence of cardiovascular events [47, 48]. At present, the cardioprotective effect of GLP-1RAs after synthesis through multiple pathways is indisputable, which may be related to the powerful weight loss, antihypertensive, anti-inflammatory, and other metabolism-improving effects of GLP-1RAs. Conversely, their direct effect on the heart remains unclear and requires further study. Meanwhile, the gastrointestinal adverse effects of GLP-1 progressively decrease with the duration of drug administration. In this study, the trend was the same as the effect of increasing HR, which may be related to a decrease in the sensitivity of the corresponding receptor [10, 49].
To the best of our knowledge, this study is the first systematic review and network meta-analysis to evaluate the effect of HR in obese adults. Previous meta-analyses have either focused on a limited number of GLP-1RAs and lacked comprehensive comparisons across agents [11, 15, 42]. In contrast, this study provides the most extensive and up-to-date data to support evidence-based clinical decision-making, particularly for patients unable to tolerate HR elevation. This study is comparable to a net meta-analysis conducted with T2DM 10 years ago, which concluded that GLP-1RAs increase HR [18]. Another research has provided reliable evidence of TZP in T2DM, but it includes only one drug and lacks comparisons with other GLP-1RAs [50]. Most studies have primarily investigated the effect on HR but not the factors that may influence this effect. The article investigated exenatide and LIR and concluded that these two increase the HR [51]. They also found that longer-acting medications may cause a more pronounced increase in HR [42].
Although the increase in HR caused by most GLP-1RAs agents is relatively small, its clinical significance varies among different populations. For high-risk groups, including patients with existing cardiovascular damage, such as heart failure, arrhythmia, or coronary artery disease, as well as adults aged 65 or older, even this minor increase in HR may have clinical significance. It is well-known that aging impairs the regulation of HR by the autonomic nervous system and increases sensitivity to hemodynamic changes [52]. It is noteworthy that in the group of patients with heart failure, per 5 bpm higher HR is associated with worse prognosis [53]. This study provides detailed data related to HR, which can guide personalized medication. For high-risk patients, if the GLP-1RAs used can reduce the magnitude of the increase in heart rate, then while retaining the benefits of GLP-1RAs in metabolism and cardiovascular aspects, minimizing the burden related to heart rate may be more beneficial.
Our work had several strengths. It incorporated almost all GLP-1RA drugs for the treatment of obesity. The effects of different GLP-1RAs, different dosages, and characteristics of the drug or the patients were also assessed using scientific statistical methods, allowing for a comprehensive evaluation. Our inclusion of only high-quality RCTs lent credibility to the results, and sensitivity analyses demonstrated the robustness of our findings.
Nevertheless, this study also had some limitations. First, our analysis is the potential inclusion of participants with prediabetes. This raises the possibility that the observed associations between GLP-1RAs and HR elevation may be partially confounded by underlying prediabetes status. Second, factors such as background medication and exercise that may influence HR were not considered when combining effects. Third, the random-effect model was inadequate for addressing the substantial heterogeneity observed in some of the included studies, which diminished the credibility of the results. In addition, the heterogeneity of the baseline characteristics of each trial included in this study may indirectly affect the results. Furthermore, after excluding one study with the largest difference in outcome, the heterogeneity of the associations between semaglutide and HR elevation (MD = 4.23; 95% CI 3.42, 5.05; I^2^ = 0%; Figure S15) and between tirzepatide and HR elevation (MD = 2.53; 95% CI 1.91, 3.15; I^2^ = 0%; Figure S16) was significantly reduced. This observation suggests a potential link between the previously observed heterogeneity in the tirzepatide subgroup and variations in dosage. Fourth, some trials were at potential risk of bias, including open-label design and pharmaceutical industry funding. In addition, publication bias may overestimate the true magnitude of GLP-1RA-induced HR elevation. Finally, strict inclusion criteria to ensure literature quality resulted in a relatively small number of studies for some agents, with certain GLP-1RAs evaluated in only a single trial, introducing potential randomization bias. As additional GLP-1RA clinical trials are conducted, we plan to update our analyses to enhance result reliability.
In conclusion, this study suggested significant associations between GLP-1RAs and elevated HR in obese patients versus placebo. ORF 36 mg links to the most pronounced HR elevation, and TZP 5 mg to the least. Treatment duration, baseline HR, and other factors may relate to HR elevation variability. Our findings inform GLP-1RA clinical consideration in obese patients, especially those with cardiovascular comorbidities or HR intolerance, and aid formulation selection. Further studies are needed to explore GLP-1RA–HR association mechanisms and broader cardiovascular relationships. Future research should include larger, well-powered trials for newer agents and publication of negative or neutral findings to reduce publication bias and enhance the robustness of conclusions.
Supplementary Information
Supplementary material 1.