Layered Management of Hypertrophic Scars and Keloids: From Silicone and Intralesional Triamcinolone Acetonide Plus 5-Fluorouracil to Adjuvant Strontium-90
Osama S Abbadi, Faris Abdon, Zuhoor S Othman, Khalid Abdel Aziz

TL;DR
This paper reviews layered treatment strategies for hypertrophic scars and keloids, emphasizing early silicone use and combination therapies for better outcomes.
Contribution
The paper provides a pragmatic, evidence-based algorithm for layered treatment of fibroproliferative scars based on lesion characteristics and patient factors.
Findings
Silicone gel or sheets are most effective for early scar prevention and treatment.
Combining triamcinolone acetonide with 5-fluorouracil improves flattening and symptom control compared to steroids alone.
Strontium-90 brachytherapy may be used as consolidation or postoperative adjuvant for selected thin keloids.
Abstract
Hypertrophic scars and keloids are fibroproliferative scars that can cause disfigurement, pruritus, pain, contracture, and reduced quality of life. Outcomes remain inconsistent because phenotypes vary by anatomic site, thickness, skin type, and time since injury, and no single modality is uniformly curative. We performed a narrative review informed by a structured search of MEDLINE/PubMed, Embase, Cochrane Library, Web of Science, and Scopus (2000 to November 2025), including clinical trials, observational studies, systematic reviews, and consensus guidance with clinically actionable treatment parameters. Evidence most consistently supports early, low-risk modulation with silicone gel or sheets for the prevention and early treatment of hypertrophic scars. For established hypertrophic scars and keloids, intralesional triamcinolone acetonide combined with 5-fluorouracil provides a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
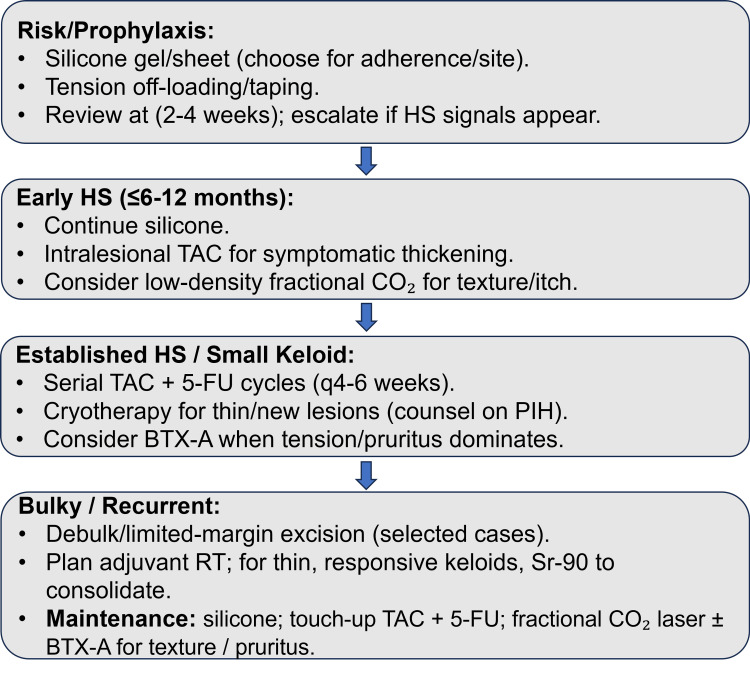 Figure 1
Figure 1| Modality | Best candidates/when to use | How it’s given (dose/parameters) | Typical outcomes/recurrence | Key risks |
| Silicone (gel or sheet) | First‑line prophylaxis and early HS; choose format for adherence (gel for mobile/visible/hot climates; sheets for flat/covered areas) | Thin film BID (gel) or near‑continuous wear (sheet) for ≥8-12 weeks | ↓ erythema/itch/height vs control in RCT; gel ≈ sheet for efficacy; gel often easier to use | Contact dermatitis (rare); adherence is the main limiter |
| Onion extract (±silicone) | When color/erythema improvement is a priority, it is best as an adjunct to silicone | Topical gel once or twice daily; combine with silicone for the best overall effect | Improves color; limited effect on height/itch alone; combo outperforms either alone at 6 months | Mild irritation/odor |
| Imiquimod 5% (post-excision) | Select cases only; inconsistent evidence-avoid routine use | Nightly to incision for several weeks post‑excision (protocols vary) | Mixed/negative data for recurrence prevention after excision | Erythema/irritation; adherence issues |
| Compression/pressure therapy | Burn scars, where garments are feasible and supervised | 20-30 mmHg garments for months | ↓ collagen I/III; improved scar profile in cohorts | Discomfort, skin breakdown, and adherence challenges |
| TAC | Symptomatic/thick HS and keloids; often used as a backbone | 10-40 mg/mL, q4-6 weeks; multiple sessions | ↓ height/pruritus; variable recurrence; monotherapy less durable than combinations | Atrophy/telangiectasia; hypopigmentation |
| Intralesional 5-FU ± TAC (combo preferred) | Established, thicker lesions; steroid‑sparing or steroid‑resistant | 5-FU 40-50 mg mixed with TAC (e.g., 10 mg/mL), weekly-biweekly cycles | Faster flattening and better durability than TAC alone across series; manageable local AEs | Pain/erosions; dose‑related ulceration |
| BTX-A | Prominent itch/contracture; high-tension sites; adjunct before laser or injections | Intradermal/intralesional mapping along tension lines; dose by lesion size | Improves VSS domains (pediatric RCT); helpful for pliability/symptoms | Injection pain; rare weakness if misplaced |
| Cryotherapy | Thinner, newer lesions; pigment-indifferent areas; as part of combination plans | Contact/spray techniques; multiple sessions (≥3) | Good–excellent responses in cohorts; symptom relief; plan for repeat sessions | Pain during freeze; hypopigmentation or PIH |
| Fractional CO₂ laser (±BTX-A, ±topical growth factor) | Textural/thick HS; earlier scars respond better; combine for greater gains | Device‑specific; low‑density fractional passes; consider sequence BTX‑A → CO2 → topical GF | Combo superior to monotherapy on VSS and thickness (retrospective 2024); generally safe | PIH, erythema, edema; consider test spot, conservative density, photoprotection |
| Photodynamic therapy (indocyanine green; ICG-PDT) | Refractory keloids, or when lasers/surgery are limited, are an adjunct in specialist care | Indocyanine-green + light source (protocols vary) | Suppresses fibroblast activity/collagen synthesis; early clinical signals | Photosensitivity, local reaction |
| Surgery + adjuvant radiotherapy | Bulky or recurrent keloids; plan adjuvant within 24 h post-excision | Excision/debulking → EBRT (electrons/orthovoltage/photons) or brachytherapy (HDR/LDR; source-dependent), site-dependent | Lower recurrence than surgery alone (site‑specific) | Radiation dermatitis; pigmentary change (PIH/hypopigmentation); logistics |
| Superficial β-brachytherapy with strontium-90 (Sr-90) after TAC + 5-FU | Small, relatively thin, responsive keloids where relapse risk is high | After serial TAC + 5‑FU when thinned to ~2-3 mm: 15-20 Gy in 3-4 daily fractions | Randomized data: ~half the 1‑yr recurrence vs injections alone; ultrasound shows stability | Local erythema/dryness; possible pigmentary change; careful shielding/collimation |
| Mechanotherapy/vacuum massage | Adjunct for pliability/symptom relief in specialist settings; not disease‑modifying alone | Intermittent negative‑pressure protocols; clinic‑based | Short‑term epidermal/dermal changes; clinical benefits uncertain | Bruising/discomfort; time/cost |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research · Laser Applications in Dentistry and Medicine · Hair Growth and Disorders
Introduction and background
Pathological skin scarring (principally hypertrophic scars (HS) and keloids) imposes aesthetic, functional, and psychosocial burdens. HS remains confined to the original wound and may remodel over time, whereas keloids typically extend beyond the wound edge and persist or recur after treatment; this clinicopathologic distinction guides prognosis and therapy [1-3]. Pruritus, pain, and contracture further reduce quality of life, especially when scars cross joints or visible areas [1,2].
Scar biology reflects persistent inflammation and dysregulated extracellular matrix (ECM) turnover with excessive collagen I/III, altered fibronectin and periostin, and reduced matrix modulators (e.g., decorin, dermatopontin), alongside aberrant fibroblast signaling in TGF-β/PI3K/Akt/mTOR and microRNA networks [2,4]. Transcriptional data implicate a wound-response signature (e.g., SERPINE1/PAI-1) that promotes myofibroblast activity and impaired remodeling [5]. In contrast, scarless fetal repair features higher hyaluronic acid, reduced inflammatory cytokine signaling, and a distinct MMP/TIMP balance-mechanistic clues that favor early hydration/occlusion and anti-inflammatory strategies [6]. These insights support pairing (pathway-targeted) therapies with approaches that modulate the mechanical and inflammatory microenvironment.
Clinically, no single modality is curative. Conventional options (silicone/compression, intralesional corticosteroids, 5-fluorouracil (5-FU), cryotherapy, lasers, surgery, and adjuvant radiotherapy) provide benefit but are limited by recurrence, side effects, and heterogeneity across phenotypes and sites [2,7]. Practical frameworks organize care into non-invasive, minimally invasive, and invasive strategies, emphasizing stepwise combinations tailored to lesion type, location, and symptoms [1,8].
Among non-invasive measures, topical silicone has randomized evidence for prophylaxis after surgery, improving scar symptoms and reducing HS/keloid formation compared with control [3]. When choosing format, a prospective comparison found similar efficacy between silicone gel and sheets on Vancouver Scar Scale (VSS) outcomes at one to three months, with greater convenience and adherence reported for gel-useful in mobile or exposed sites and warm climates [9]. Onion extract (Allium cepa) may improve color, but height reduction is driven by silicone; the combination achieved the best overall therapeutic index in a three-arm study and can be considered when erythema is prominent [10].
For established lesions, intralesional corticosteroids remain a cornerstone, but adding a second agent improves durability. Prospective and retrospective series support 5-FU alone or in combination with triamcinolone, with better flattening and symptom control and acceptable safety [11,12]. Meta-analytic syntheses similarly favor combinations over steroid monotherapy, and tension-modulating adjuncts are rational, given mechanotransduction in scar biology [13,14]. Cryotherapy helps reduce thickness but is limited by pain and pigmentary change, particularly in darker skin [7]. Energy-based devices (e.g., pulsed-dye and fractional CO_2_ lasers) can improve vascularity, pliability, and thickness, often as part of multimodal regimens [7,14]. Botulinum toxin-A (BTX-A) showed improvement in pediatric post-burn HS/keloids in an intra-patient randomized trial and is increasingly used to reduce tension and symptoms as an adjunct to intralesional or laser therapy [14,15]. Photodynamic therapy using indocyanine green (ICG-PDT) demonstrates fibroblast inhibition and early clinical signals; it is a plausible option for refractory disease within specialist pathways [16,17].
Surgery alone carries a high recurrence rate for classic keloids; combination strategies are preferred [8]. Adjuvant radiotherapy has evolved with a focus on timing and dose. Guidance emphasizes delivery within ~24 hours post-excision when indicated, with fractionation tailored to site and depth [8]. Randomized and prospective data show that strontium-90 (Sr-90; β-radiation) (as a superficial brachytherapy) can lower recurrence and stabilize ultrasound-measured thickness/elastic modulus, particularly for small, early keloids after response to intralesional therapy [18]. These findings support a pathway in which bulky or recurrent keloids undergo limited-margin excision followed by immediate adjuvant radiotherapy, with intralesional consolidation as needed [8,18]. Adjuvant radiotherapy is delivered using multiple techniques, most commonly external beam radiotherapy (EBRT) (including electron beam and X-ray-based approaches) or brachytherapy (interstitial or surface), depending on target depth and institutional resources [19,20]. In this review, Sr-90 is highlighted not as a universal radiotherapy solution, but because its highly superficial β-dose profile makes it a practical consolidation option for selected thin lesions within a layered treatment pathway [8,18].
Emerging multimodal protocols intentionally pair the pathway with the physics. A recent analysis reported that sequential BTX-A + fractional CO_2_ laser + topical growth factor outperformed monotherapies on thickness and validated scar scales without new safety signals, especially when started earlier after scar formation [14]. On the biologic front, topical formulations that down-regulate phosphorylated PI3K/Akt/mTOR reduced keloid size in experimental models, underscoring the translational potential of mTOR-axis modulation [21].
This review synthesizes established and emerging interventions for HS and keloids, grading their practical value (efficacy, durability, safety, and feasibility) and proposing a phenotype-aware, escalation-ready algorithm that integrates prevention, intralesional and energy-based combinations, and surgery with adjuvant radiotherapy where appropriate [1-3,5-15,18].
Review
Methods
Search Strategy and Study Selection
We conducted a narrative review informed by a structured literature search, aimed at summarizing clinically actionable evidence and parameters for stepwise (layered) management of HS and keloids. We searched MEDLINE/PubMed, Embase, the Cochrane Library, Web of Science, and Scopus for English-language literature published from 2000 to November 2025 using combinations of terms related to HS/keloids and common interventions (e.g., silicone gel/sheets, intralesional corticosteroids, 5-FU, cryotherapy, lasers including fractional CO_2_, BTX-A, surgery, radiotherapy, and Sr-90). Reference lists of eligible studies and relevant guideline/consensus documents were manually screened to identify additional studies. This work was designed as a narrative review with structured searching and was not intended as a formal systematic review.
Eligibility and Data Handling
We included human studies addressing prevention and/or treatment of HS and keloids, including randomized trials, controlled studies, prospective/retrospective cohorts, and case series with clinically interpretable outcomes, as well as systematic reviews/meta-analyses and guideline/consensus statements. Translational/experimental studies were included when they directly informed therapeutic rationale or clinically used parameters. We excluded non-clinical papers without interpretable endpoints and studies lacking sufficient intervention detail to support practical implementation. From the included studies, we extracted key clinical information, including treatment modality, dose/parameters, treatment interval/session number when reported, follow-up duration, outcomes/recurrence definitions, and adverse effects.
Outcomes and Measures
Primary outcomes included scar severity and treatment response as reported using validated clinical measures and recurrence definitions used by the source studies. Where validated scales were used, the most common measures were the VSS and the Patient and Observer Scar Assessment Scale (POSAS), which capture domains such as vascularity/pigmentation, pliability, height/thickness, and patient-reported symptoms/appearance impact [22,23]. Objective adjunct outcomes (when reported) included ultrasound-based thickness and related biomechanical metrics, as well as symptom outcomes such as pruritus and pain.
Appraisal and Synthesis
Because interventions, dosing/parameters, follow-up periods, and outcome definitions varied substantially across studies, we did not attempt quantitative pooling. Instead, findings are presented as a structured narrative emphasizing: (1) first-line low-risk measures for prevention/early disease, (2) a practical pharmacologic backbone for established lesions (intralesional triamcinolone ± 5-FU), (3) phenotype- and site-informed adjuncts (e.g., cryotherapy, fractional CO_2_ laser, BTX-A), and (4) escalation/consolidation strategies including surgery with adjuvant radiotherapy and, in selected candidates, superficial β-brachytherapy using Sr-90.
Discussion
Management of HS and keloids remains challenging because biology and biomechanics conspire to sustain fibroproliferation long after the inciting injury has resolved. Across the studies reviewed, a coherent picture emerges: outcomes improve when care is layered, beginning with low-risk measures that modulate hydration and inflammation, moving to intralesional anti-proliferative therapy for established disease, and reserving procedures and adjuvant radiotherapy for selected phenotypes with a propensity to recur [1,2,7,8,13,18]. Key modalities, typical dosing parameters, expected outcomes or recurrence, and principal risks are summarized in Table 1 [3,7-18,24-29].
Prevention and very early management should be adherence-friendly and straightforward. Randomized evidence supports topical silicone as a foundation therapy after closure, with reductions in erythema, pruritus, and early thickening versus control, and excellent acceptability [3]. When patients choose between formats, comparative data show similar efficacy for gels and sheets; gels are often preferred for mobile or visible sites and hot climates, while sheets suit flat, covered areas, so the practical choice is whichever format maximizes use rather than chasing a non-existent efficacy gap [9]. Onion extract adds value mainly for colour/erythema and works best when combined with silicone; by itself, it does little for height or itch [10]. Imiquimod 5% has been inconsistent after excision and should not be relied upon as a standalone prophylactic measure [17].
Once a scar is established and symptomatic, intralesional therapy becomes the workhorse. Corticosteroids alone retain utility, but converging prospective data indicate that adding 5-FU improves flattening and durability in many patients, with manageable local adverse effects that are mitigated by technique and dosing adjustments [11-13,25,26]. This combination also appears to limit steroid-related atrophy and telangiectasia compared with triamcinolone alone in some series [13,25,26]. BTX-A is an attractive adjunct when tension, pruritus, or surface rigidity dominate the phenotype; an intra-patient randomized pediatric trial demonstrated improvements across VSS domains with good tolerability, suggesting a role where symptom relief and pliability gains are priorities [30]. These findings align with the broader principle that reducing mechanical load and myofibroblast drive can amplify drug effects.
Energy-based procedures and photodynamic therapy can be sensibly integrated rather than used in isolation. Fractional CO_2_ laser improves texture and thickness and pairs well with anti-proliferative strategies. A contemporary multimodal sequence (BTX-A followed by fractional CO_2_ and a topical growth factor) outperformed monotherapies on validated scales and thickness, particularly when instituted relatively early [14]. ICG-PDT shows mechanistic and early clinical signals (suppression of keloid fibroblast activity and collagen synthesis), making it a plausible option in refractory disease where access to lasers or surgery is limited. However, controlled clinical trials are still needed [16,17]. Cryotherapy remains useful for thinner, newer lesions, with consistent symptom relief and flattening across cohorts; its trade-offs are pain and pigmentary change, which warrant careful counseling in darker skin types and thoughtful pairing with other modalities [7,25,27].
For keloids with significant bulk or a track record of relapse, surgery should rarely stand alone. Contemporary guidance emphasizes combination care and, when surgery is chosen, the importance of well-timed adjuvant radiotherapy to reduce recurrence, ideally within 24 hours of excision, depending on the site and modality [8]. Superficial β-brachytherapy with Sr-90 offers a pragmatic, targeted option in carefully selected non-surgical or post-injection scenarios. In a randomized setting, adjuvant Sr-90 delivered in short courses (e.g., 15-20 Gy over three to four days) approximately halved one-year recurrence compared with injections alone, not by further debulking but by stabilizing a good response; efficacy is most significant when lesions are pre-thinned to ~2-3 mm, so dose is deposited where it is needed [18]. This consolidation concept aligns with the broader theme of making early gains and then maintaining them.
Radiotherapy for keloid control can be delivered as EBRT (including electron beam radiotherapy and X-ray-based techniques) or as brachytherapy, where a source is positioned close to the target to achieve a steep dose gradient [19,20]. Clinical practice has used multiple radiotherapy modalities and sources, including electron beam radiotherapy, Ir-192 high-dose-rate (HDR) brachytherapy, and Sr-90 surface (plaque/dermal plate) brachytherapy, confirming that Sr-90 is one option within a broader radiotherapy toolkit [31,32]. We focus on Sr-90/Sr-90Y not to imply superiority over all radiotherapy techniques, but because it has a distinct niche in (layered) care as superficial consolidation: Sr-90 is a β-emitter, and its dose falls rapidly with depth to approximately 1-3% at 5 mm; about 75% of β-radiation is absorbed within the first 2 mm, with the remaining dose absorbed within the subsequent 1 mm of tissue [8]. This physical profile supports Sr-90 use when lesions are small and relatively thin, particularly after intralesional therapy has achieved meaningful thinning and symptom control, and the clinical objective becomes maintaining stability and reducing recurrence [8]. In a prospective, randomized, controlled trial, Sr-90 given after three triamcinolone acetonide (TAC) + 5-FU intralesional injections reduced the one-year recurrence rate from 85.7% to 44.4% in small, relatively young keloids, supporting its role as an adjuvant consolidation strategy rather than a primary debulking tool [18].
Technique selection should be guided by target depth and lesion geometry. Sr-90 is most appropriate when the intended target is superficial and thin, where rapid depth-dose fall-off is advantageous, and exposure to deeper tissues should be minimized [8]. For bulkier or deeper lesions, modalities that can prescribe dose at greater depths may be more appropriate, such as EBRT (commonly electrons or selected X-ray approaches) or interstitial HDR brachytherapy, where catheter placement and prescription depths typically aim to cover deeper target tissues (e.g., prescribed dose depth 4-7 mm has been reported for interstitial HDR after excision) [8,19]. Consistent with this, Ir-192 HDR brachytherapy has been used as an adjuvant approach in difficult recurrent cases, with protocols such as 15 Gy in three fractions reported in salvage settings [32]. Accordingly, Sr-90 should be presented as a selective superficial option within an overall radiotherapy toolkit rather than a universal substitute for EBRT or interstitial brachytherapy [8,19].
The biological rationale for these layered strategies is increasingly apparent. Aberrant signaling through TGF-β and PI3K/Akt/mTOR sustains collagen I/III deposition, alters fibronectin and periostin, and suppresses matrix modulators such as decorin and dermatopontin [2,4]. Transcriptional work highlights a wound-response program involving SERPINE1/PAI-1 that propagates myofibroblast activity and impaired remodeling [5]. In contrast, scarless fetal repair features higher hyaluronic acid levels, lower profibrotic cytokine tone, and a remodeling-favouring MMP/TIMP balance [6]. Interventions that hydrate/occlude, reduce inflammatory drive, down-shift fibroblast proliferation, and relieve mechanical tension therefore make mechanistic sense, and, in practice, combinations that (pair the pathway with the physics) consistently perform better than single agents [1,2,6,8,13,18,21].
Safety and practicality are central to real-world choices. Silicone is safe and inexpensive; adherence is the primary determinant of benefit [3,9]. Intralesional TAC + 5-FU typically requires weekly sessions early on; transient pain and superficial erosions are common trade-offs that can be reduced with smaller aliquots, the fanning technique, and spacing [11,12]. Cryotherapy and lasers carry a risk of post-inflammatory hyperpigmentation (PIH); therefore, parameter selection and sun protection are essential, particularly in individuals with darker skin types [7,27,33-35]. With Sr-90, careful patient selection and shielding are needed; reported acute toxicity is low when lesions are thin, and fields are well collimated [18]. BTX-A has been well tolerated in both pediatric randomized studies and adult series, and its effect on tension likely complements intralesional and laser-based treatment plans [13,30].
Considerations in Darker Skin Types and Pigmentary Change Risk
Keloids disproportionately affect individuals with more pigmented skin (Fitzpatrick skin types IV-VI), and pigmentary safety and counseling are therefore central to real-world management [36,37].
Pigmentary adverse effects are particularly relevant when using cryotherapy and energy-based devices. In the keloid cryotherapy series, hypopigmentation is a recognized adverse effect [7,33-35,38]. Fractional laser procedures in higher Fitzpatrick phototypes also carry a risk of PIH [7,33-35,38].
Practical risk-reduction measures include explicit expectation setting, baseline photography, conservative parameter selection, considering test spots when feasible, strict photoprotection, and close follow-up to detect and manage pigmentary change early [34,35].
When adjuvant radiotherapy or brachytherapy is used as consolidation or post-excision control, patients should also be counseled that pigmentary change and telangiectasia can occur, even though acute reactions are typically mild and self-limited [18-20,31,32].
Our phenotype-aware, layered approach is presented in Figure 1 (clinical treatment algorithm) [3,7-15,17,18,25-27], which maps prevention/early modulation (silicone; tension off-loading), the intralesional backbone (TAC + 5-FU), escalation options (cryotherapy, fractional CO_2_, BTX-A), and consolidation with Sr-90 in selected cases.
Clinical algorithm for layered management of hypertrophic scars and keloidsEarly measures emphasize hydration and tension reduction (silicone as first-line treatment); TAC + 5-FU is the pharmacologic backbone for established disease, with cryotherapy, fractional CO2, and BTX-A added based on phenotype. In selected, relatively thin keloids, Sr‑90 can consolidate response or follow excision at high‑risk sites.Sources (article/s): silicone [3,9]; TAC + 5‑FU [11-13,25,26]; cryotherapy [7,25,27]; BTX‑A and multimodal sequences [14,15]; fractional CO2 combinations [14]; adjuvant radiotherapy/Sr‑90 [8,18]; adjuncts (onion extract [10]; imiquimod negative [17]).HS: hypertrophic scars; TAC: triamcinolone acetonide; 5-FU: 5-fluorouracil; BTX-A: botulinum toxin type A; Sr-90: strontium-90; RT: radiotherapy
The algorithm is intended as a pragmatic escalation pathway rather than a rigid protocol, and site, thickness, symptoms, skin type, and tolerance should be used to individualize reassessment intervals. As a practical guide, early noninvasive therapy with silicone can be reassessed at about 8-12 weeks (consistent with common trial follow-up structures) to confirm symptomatic improvement and early flattening and to address adherence [3,9] For established lesions treated with intralesional corticosteroids, a response check after approximately three sessions given every four to six weeks is a reasonable trigger to either continue the same regimen or add/transition to combination therapy when improvement is clinically small or plateaus [13,25,26,39]. When 5-FU-based injection regimens are used weekly to biweekly, reassessment after roughly four to six sessions is typically sufficient to judge whether meaningful flattening and symptom control are progressing [26].
For procedural adjuncts, both cryotherapy and fractional laser protocols are commonly delivered as multi-session courses; therefore, a minimum trial of about three sessions is a practical benchmark before declaring non-response, unless adverse effects, intolerance, or pigmentary risk necessitate earlier modification [7,27,38,40]. Across modalities, escalation should be accelerated when there is functional impairment (e.g., contracture), rapid progression, early relapse after an initial response, recurrent ulceration, or unacceptable adverse effects with the current modality [13,25,26,39].
Taken together, the evidence supports a pragmatic, phenotype-aware approach. After surgery or trauma at high-risk sites, begin silicone promptly and consider tension-offloading; move to intralesional TAC + 5-FU if hypertrophy develops despite early measures. For small, relatively thin primary keloids, TAC + 5-FU, with or without cryotherapy, is a reasonable first step; if responses are good but short-lived, consolidation with Sr-90 can extend remission [7,18]. Bulky or recurrent lesions fare better with staged debulking or limited-margin excision embedded in a program that plans adjuvant radiotherapy from the outset, rather than as a last resort [8]. Across scenarios where tension, pruritus, or stiffness predominate, BTX-A and fractional CO_2_ laser (sometimes in sequence with topical growth factors) are logical additions [30]. Photodynamic therapy can be considered in specialist pathways for refractory disease or when resource constraints limit other options [16,17]. Onion extract is best reserved as a color-directed adjunct alongside silicone [10].
The literature remains heterogeneous. Definitions of recurrence vary, follow-up is often brief, and many studies are single-center with modest sample sizes. Mechanotherapy (vacuum massage/negative-pressure massage) shows measurable, short-term structural changes and plausible mechanotransduction effects, but clinical endpoints are inconsistent, and studies are small with risk of bias; at present, it is best viewed as an adjunct for pliability and comfort within a broader plan rather than a disease-modifying therapy [28,29]. These limitations suggest conservative, combination-oriented recommendations and emphasize the need for standardization. Priorities for future work include harmonized outcome sets that pair POSAS/VSS with objective ultrasound or elastography, consensus definitions and timepoints for recurrence (at least 12 months), and pragmatic comparisons of common sequences (e.g., cryotherapy followed by TAC + 5-FU then an adjuvant modality) versus monotherapies. Mechanism-guided trials (targeting PI3K/Akt/mTOR or related nodes and testing ICG-PDT in controlled designs) are also warranted [5,16,17,21].
In summary, durable control of HS and keloids is most likely when clinicians match treatment to phenotype, start early with adherence-friendly measures, deploy intralesional combinations as a backbone, and stabilize good responses with procedures or adjuvant radiotherapy where appropriate. This strategy is supported by randomized and prospective data for silicone, BTX-A, TAC + 5-FU, and Sr-90 in defined contexts, anchored by an increasingly coherent mechanistic rationale [3,8-13,18,30,41,42].
Conclusions
A single therapy rarely controls HS and keloids. The most consistent gains come from layered care: begin with prevention and early modulation (silicone; tension control), anchor treatment of established lesions with intralesional TAC + 5-FU, and add phenotype-specific options (cryo, fractional CO_2_, BTX-A) to address thickness, texture, pruritus, and tension. In selected, relatively thin keloids that respond to injections (or after excision at high-risk sites), adjuvant radiotherapy, including superficial beta-brachytherapy with Sr-90, can reduce recurrence. In darker skin types, management should explicitly address pigmentary risk when selecting cryotherapy, lasers, or radiotherapy. This framework balances efficacy, safety, and feasibility and can be adapted to lesion site, patient preferences, and resource availability.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Update on hypertrophic scar treatment Clinics (Sao Paulo) Rabello FB Souza CD Farina Júnior JA 5655736920142514111710.6061/clinics/2014(08)11PMC 4129552 · doi ↗ · pubmed ↗
- 2Skin scarring BMJ Bayat A Mc Grouther DA Ferguson MW 889232620031252197510.1136/bmj.326.7380.88PMC 1125033 · doi ↗ · pubmed ↗
- 3The use of silicone gel in the treatment of fresh surgical scars: a randomized study Clin Exp Dermatol de Giorgi V Sestini S Mannone F Papi F Alfaioli B Gori A Lotti T 6886933420091950858010.1111/j.1365-2230.2008.03096.x · doi ↗ · pubmed ↗
- 4Regenerative healing, scar-free healing and scar formation across the species: current concepts and future perspectives Exp Dermatol Ud-Din S Volk SW Bayat A 6156192320142486307010.1111/exd.12457 · doi ↗ · pubmed ↗
- 5Identification of a transcriptional signature for the wound healing continuum Wound Repair Regen Peake MA Caley M Giles PJ 3994052220142484433910.1111/wrr.12170 PMC 4230470 · doi ↗ · pubmed ↗
- 6Fetal wound healing Front Biosci Colwell AS Longaker MT Lorenz HP 088200310.2741/118312957846 · doi ↗ · pubmed ↗
- 7Cryotherapy in treatment of keloids: evaluation of factors affecting treatment outcome J Cutan Aesthet Surg Barara M Mendiratta V Chander R 185189520122311251410.4103/0974-2077.101376 PMC 3483575 · doi ↗ · pubmed ↗
- 8Radiotherapy for keloids: a comprehensive narrative review Cureus Nien HH Yu PC Yen YH Tsai YL Wang LY Hsieh CH 017202510.7759/cureus.93869 PMC 1258488141194850 · doi ↗ · pubmed ↗