Clinical and economic evaluation of risk factor guided respiratory syncytial virus prophylaxis in Colombian preterm infants
Carlos E. Rodriguez-Martinez, Jaime Ordonez, Xavier Carbonell-Estrany, John Fullarton, Ian Keary, Barry Rodgers-Gray, Ivonne D’Apremont, Daniel E. Noyola, Paulo Andre Ribeiro, Renato T. Stein, Nestor Vain, Jean-Eric Tarride, Bosco Paes

TL;DR
This study shows that using a risk scoring tool to guide RSV prophylaxis in preterm infants in Colombia is cost-effective.
Contribution
The first evaluation of the IRST-guided RSV prophylaxis in Colombia for preterm infants.
Findings
The IRST plus additional factors predicted RSV hospitalization risk with high accuracy (AUC = 0.823).
Palivizumab prophylaxis was cost-effective at COP20,225,126 per QALY for moderate- and high-risk infants.
Probabilistic analysis showed a 61.1% probability of cost-effectiveness at the GDP/capita threshold.
Abstract
The International Risk Scoring Tool (IRST) comprises three risk factors (age relative to the respiratory syncytial virus [RSV] season; household and/or maternal smoking; siblings and/or daycare attendance) and enables the cost-effective targeting of palivizumab to infants born at 32–35 weeks’ gestational age (wGA) at greatest risk of related hospitalization (RSVH). This study provides the first evaluation of IRST-guided RSV prophylaxis in Colombia. The IRST (with wGA substituted for chronological age as RSV is endemic in Colombia) plus other risk factors were assessed using data from 81 infants born 32–35 wGA with RSVH and 49 gestational- and age-matched controls. A cost-utility model comparing IRST-guided palivizumab versus no prophylaxis from the healthcare provider perspective was then adapted using Colombian costs and data (5% discounting). Infants could experience either RSVH,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
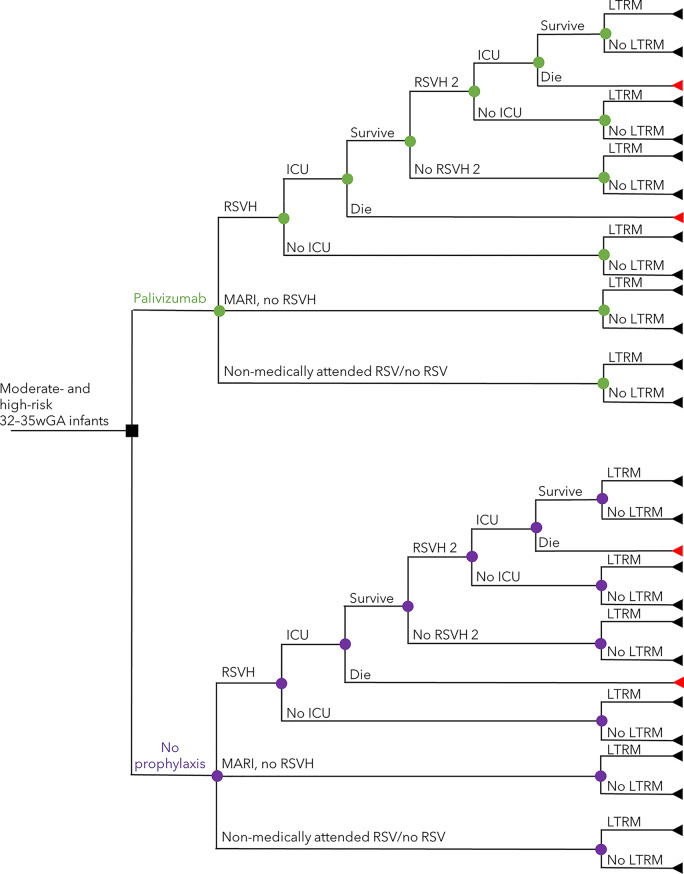 Figure 1
Figure 1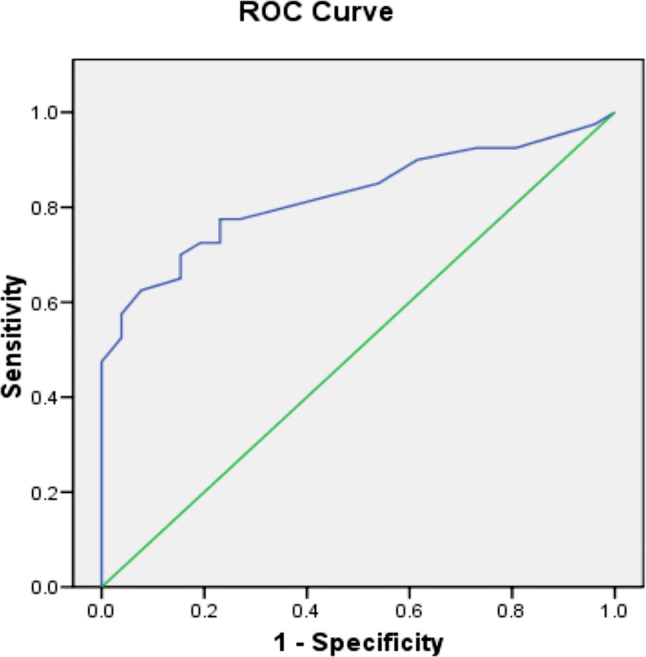 Figure 2
Figure 2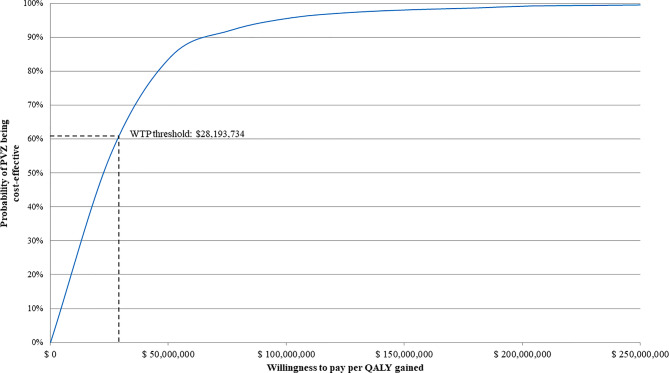 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRespiratory viral infections research · Neonatal Respiratory Health Research · Delphi Technique in Research
Introduction
Respiratory syncytial virus (RSV) is a major global disease of early childhood causing approximately 12.9 million lower respiratory tract infections (LRTIs), 2.2 million related hospitalizations (RSVHs), and 66,500 deaths each year in infants [1]. Importantly, more than 95% of RSV-LRTI episodes and 97% of RSV-related deaths occur in low- and middle-income countries (LMICs) [1]. In Colombia, studies of infants hospitalized with LRTI have reported that between 26 and 38% were RSV-positive [2, 3], with associated mortality observed only in those with confirmed RSV infection [2]. The well-established high-risk populations with chronic lung disease (CLD), congenital heart disease (CHD), and prematurity who are at risk for RSVH, were identified in these Colombian cohorts [2–6]. At present, there is no effective treatment for RSV-LRTI so management is aimed at prevention either through hygiene measures or immunization.
Immunoprophylaxis with palivizumab, a humanized monoclonal antibody, has proven highly effective at preventing RSVH in high-risk infants, such as those with CLD, CHD, and premature birth at ≤ 35 weeks’ gestational age (wGA) [7–9]. A prospective, observational study of 600 Colombian infants born at ≤ 32 wGA or with CLD or CHD reported that palivizumab was well-tolerated and reduced RSVHs by an estimated 86–93% and RSV-related mortality by 97% [10]. Palivizumab is currently the only preventive intervention available in Colombia, however, its use is restricted to < 32 wGA infants and those born 32–34 wGA with CLD, primarily due to cost considerations [11, 12]. An economic analysis from 2013, commissioned by the Ministry of Health and the National Guideline for Integral Attention of Preterm Infants Study Group, determined palivizumab to be not cost-effective versus no prophylaxis in infants < 35 wGA (incremental cost-effectiveness ratio [ICER] per quality adjusted life year [QALY] gained of COP53,121,137 [USD12,481]) [11]. Conversely, a recent analysis found palivizumab to be a dominant strategy over no prophylaxis for preventing RSVH in preterm neonates ≤35 wGA and infants with CLD and CHD [13]. To date, no analysis has assessed the cost-effectiveness of palivizumab specifically in infants born 32–35 wGA.
For otherwise healthy infants born 32–35 wGA, targeting palivizumab prophylaxis to those at greatest risk of RSVH using the International Risk Scoring Tool (IRST) has proven a cost-effective strategy in both Canada and Italy [14–16]. The IRST comprises three risk factors (birth 3 months before to 2 months after the RSV season start date; household and/or maternal smoking; siblings and/or daycare attendance) to accurately categorize the risk of RSVH in these infants (Figure S1 & Table S1) [14]. The IRST was developed and validated using data from seven studies of 14,553 infants born 32–35 wGA from high-income, Northern Hemisphere countries with a defined RSV season [14]. For adoption in Colombia, the IRST requires modification to reflect the tropical climate where RSV has an endemic, non-seasonal pattern, with increased epidemic activity associated with rainy periods [17], and where the importance (weighting) of the other risk factors may differ within the context of an upper middle-income country. The objective of this study was to generate a Colombian-specific version of the IRST and to assess whether its adoption in Colombia could guide the cost-effective use of palivizumab (versus no prophylaxis) in 32–35 wGA infants.
Materials and methods
Development of a Colombian-specific version of the IRST
Risk factor data were collected from otherwise healthy infants born at 32 weeks 0 days to 35 weeks and 6 days between November 2022 and February 2023 at two hospitals in Colombia (Fundación Hospital Pediátrico la Misericordia (HOMI) and Clínica de Marly Jorge Cavelier Gaviria). Infants had either an RSVH within the first six months of life (cases) or were gestationally and chronologically age-matched controls born at the participating hospitals but with no RSVH or other respiratory illness related hospitalization. Infants with significant morbidity other than prematurity, such as CLD, CHD and immunodeficiency, neuromuscular impairment, Down syndrome and cystic fibrosis were excluded. Information on the IRST risk factors: smokers in the household (Yes/No), maternal smoking (Yes/No), siblings (Yes/No) and daycare attendance (Yes/No) were collected. In addition, as a potential substitute for ‘birth 3 months before to 2 months after the RSV season start date’ within the original IRST, data on wGA (32, 33, 34, 35 wGA) together with two other risk factors considered important in Latin America (LATAM), breastfeeding (defined as exclusive and given or planned from birth to 3 months of age, or mixed [breastfeeding and formula]; Yes/No), and maternal education to primary level or less (as a surrogate for social deprivation; Yes/No), were investigated. Analysis of the pooled dataset underpinning the IRST revealed that, whilst not reaching statistical significance, an expected trend towards increased rates of RSVH with lower wGA at birth (Table S2) was present; hence, arose the rationale for exploring whether wGA had the discriminatory power to be a substitute for chronological age in relation to the RSV season start date in a Colombian version of the IRST. Predicated on previous RSV risk factor model assessments [18–20], a total of 100 infants (50 cases and 50 controls) with complete risk factor data and who had not received palivizumab (or any other RSV preventive intervention) were targeted. The study protocol was approved by the ethics committee of the Fundación Hospital de La Misericordia.
The Colombian risk factor data were initially subjected to logistic regression, with all variables treated as categoric, to generate the equivalent of the IRST, with wGA substituted for chronological age, and subsequently with and without the addition of breastfeeding (exclusive or mixed) and maternal education either singly or combined with the other risk factors. For each analysis, predictive accuracy was assessed by calculation of the area under the receiver operating characteristic curve (AUROC), with a value of ≥0.75 considered ‘good’ (original IRST AUROC: 0.773) [14]. The combination of Colombian risk factors with the highest AUROC was then selected for further analysis.
In the original IRST, infants classified as low-risk (score of ≤19) had a 1.0% RSVH rate, moderate-risk (score of 20–45) a 3.3% rate, and high-risk (score of 50–56) a 9.5% rate (Table S3) [14]. The combined moderate- and high-risk groups had a 6.3% RSVH rate and captured 85.2% of all RSVHs [14]. To create the final Colombian-specific version of the IRST, the RSVH rates for each risk group were adjusted using a pro rata interpolation from the IRST to the Colombian data, predicated on the predictive accuracy of the selected Colombian model. This assumed the same number of total RSVHs across the risk groups for the IRST and Colombian-specific IRST and, in the absence of any published Colombian epidemiological data for 32–35 wGA infants, an estimated RSVH rate of 7.6%. The latter was based on a single arm study of palivizumab prophylaxis in < 35 wGA infants (40.1% with CLD) that reported an RSVH rate of 1.9% (no RSVHs in 33–34 wGA infants) uplifted to reflect an assumed effectiveness of 75% risk reduction [10, 21, 22]. RSVH rates are presented as median with 95% confidence intervals (CI).
Cost-effectiveness of the Colombian-specific version of the IRST at guiding palivizumab prophylaxis
Cost-utility model overview
A previously published and validated Canadian cost-utility model, that assessed IRST-guided palivizumab prophylaxis versus no prophylaxis [15], was adapted to the Colombian healthcare provider perspective. In brief, the model included a decision-tree wherein prophylaxed/non-prophylaxed infants at moderate- or high-risk of RSVH, as scored by the Colombian IRST, could experience either RSVH, emergency room medically-attended RSV infection (MARI) [23], or remained uninfected/non-attended (Fig. 1). Palivizumab efficacy (82.2% relative reduction in RSVH) for 32–35wGA infants was drawn from the IMpact-RSV trial (Table 1) [22]. The RSVH rate for infants assessed at moderate- or high-risk not receiving prophylaxis was as per the final Colombian-specific IRST. Infants with RSVH (mean stay 8.6 days) could be admitted to the intensive care unit (ICU; 7.8%) and suffer potential mortality (3.6%), commensurate with published Colombian data [2, 24, 29]. All surviving infants, irrespective of RSV infection status, had the potential to experience respiratory morbidity for up to 18 years of age over a lifetime horizon (Table S4). In the absence of any Colombian-specific data or such data from a country similar in terms of healthcare systems, genetic backgrounds and socioeconomic conditions, long-term morbidity was modelled using Spanish [30] and Swedish data [31–33]. The impact of palivizumab was then applied using data from three studies: Simoes et al. [34], Blanken et al. [35] and Yoshihara et al. 2013 [36]. Utility values for RSVH, MARI and for respiratory morbidity were unchanged from the Canadian cost-utility analysis, with the rates for each respective variable for the prophylaxed and non-prophylaxed infants used as multipliers to calculate aggregated utilities for the two populations (Table 1) [15, 25–28].Fig. 1. Decision tree describing the clinical pathway utilized within the model. Nodes represent points where more than one event is possible; the square node represents a decision addressed by the model. Branches represent possible events experienced by patients. Triangles represent decision tree endpoints. ICU intensive care unit, LTRM long-term respiratory morbidity, MARI medically-attended RSV infection without hospitalization, RSV respiratory syncytial virus, RSVH RSV-related hospitalization.Table 1. Input parameters for the cost-utility modelParameterPoint estimatesReference source(s)PalivizumabNo palivizumab**Palivizumab efficacy (RRR)**82.2%-Notario et al. 2014 [22]RSVH^a^- Overall rate3.3%18.6%^f^Colombian-specific IRST- Ward LOS, mean days8.68.6Piñeros et al. 2013 [2]- ICU rate7.8%7.8%Rodriguez-Martinez et al. 2020 [24]- Utility in hospital0.600.60Weiner et al. 2012 [25] and Leidy et al. 2005 [26]- Utility post discharge - No sequelae0.880.88Greenough et al. 2004 [27] - Long-term sequelae^b^0.790.79Chiou et al. 2005 [28]- Mortality^c^3.6%3.6%Villamil et al. 2020 [29]MARI- Rate^d^2.95%16.57%Carbonell-Estrany et al. 2010 [23]- Utility no sequelae or respiratory symptoms0.950.95Greenough et al. 2004 [27]Utility long-term sequelae or respiratory symptoms^e^0.790.79Chiou et al. 2005 [28]No RSV^e^Utility No sequelae or respiratory symptoms0.950.95Greenough et al. 2004 [27]Utility long-term sequelae or respiratory symptoms^e^0.790.79Chiou et al. 2005 [28]^a^First and subsequent RSVHs. ^b^ Long-term respiratory morbidity following RSVH or MARI was assumed to last until age 18, but only until age 6 in infants without an RSV infection or who had a non-medically attended RSV infection, using the same rates as for MARI (Table S4). ^c^ Applied only to patients in ICU. ^d^ Emergency department only. ^e^ Infants without an RSV infection or not requiring medical management. ^f^S ee Table 3 for full details. ICU intensive care unit, LOS length of stay, MARI medically-attended RSV infection without hospitalization, RRR relative risk reduction, RSV respiratory syncytial virus, RSVH RSV-related hospitalization, wGA weeks’ gestational age
Costs
Pecuniary inputs included those for RSVH (including ICU admission), MARI, ongoing respiratory morbidity, and societal costs, in addition to both acquisition and administration costs relating to palivizumab in Colombia (Table 2). The total average cost for palivizumab per 32–35 wGA infant was COP7,790,674 (USD1,830). This assumed an average of 4 injections for all infants irrespective of date of parturition since RSV is endemic (50 mg vial: COP1,416,724 [USD333]; 100 mg vial: COP2,804,887 [USD659] [37]) with 70% vial sharing (5% wastage) [Note: palivizumab vials are single use only], in line with local clinical practice (Dr Rodriguez-Martinez) and studies [10, 21], and a weight at each administration calculated by applying a growth algorithm [41] to an estimated average birth weight of 1991 g [42, 43]. Administration costs assumed 70% of injections were given by a nurse and 30% by a clinician, resulting in a blended cost of COP72,812 [USD17] per infant [24, 38]. The annual cost of long-term respiratory morbidity per child was COP2,229,920 (USD524), representing a cost of COP3,428,872 (USD806) for 0–6 years of age [39] and 1,630,444 (USD383) for 7–18 years of age [40], using Colombian age-group specific wheezing and asthma data.Table 2. Direct costs for cost-utility modelParameterCost(COP)UnitsReference source(s)Palivizumab- 50 mg vial- 100 mg vial1,416,724.002,804,887.19Lowest combination of vials per infant weightCalculated from prices paid data [37]- Administration - Clinician - Nurse specialist32,450.2312097.001 per injection, assuming 30% clinician and 70% nurse administeredRodriguez-Martinez et al. 2020 [24]Economic Research Institute [38]**RSVH total stay (including preadmission and ICU costs)**7,240,740.14^c^1 per RSVH^b^Rodriguez-Martinez et al. 2020 [24]MARI- ED visit69,663.411 per affected infant^a^Rodriguez-Martinez et al. 2020 [24]**Respiratory morbidity (per annum)**2,229,919.861 per affected infant^b^Years 0–6: Buendía et al. 2022 [39]Years 7–18: Flóres-Tanus et al. 2018 [40]Costs uplifted as required to Colombia 2022 levels using the latest World Bank Data available at the time of writing. ^a^See Table 1 for rates. ^b^See Table S4 for rates. ^c^Specific cost for preterm infants without CLD
All costs were derived from publicly available sources and, if required, adjusted for inflation to Colombia 2022 levels using the latest World Bank Data available at the time of writing. A 5.0% discount was applied to costs and utilities as per Colombian recommendations [44].
Outputs
Outcomes were expressed as the cost per QALY (incremental cost-utility ratio [ICUR]) for palivizumab versus no intervention [44]. The willingness-to-pay (WTP) threshold in Colombia was determined to be COP28,193,734 (USD6,624), the gross domestic product (GDP) per capita [45].
Sensitivity analyses
Probabilistic (PSA) and deterministic (DSA) sensitivity analyses were performed with limits of plus or minus 10% and 20%, respectively, applied on the values of the tested variables. The PSA (10,000 Monte Carlo simulations) used gamma distribution as the default for costs, beta distribution for utilities and RSVH and associated rates, and normal distribution for discount rates and mortality rate (as an approximation of Poisson distribution) (Table S5).
Scenario analyses
The following scenario analyses were performed: i) inclusion of indirect/societal costs, which were adapted from a Colombian study on pediatric cutaneous leishmaniasis [46] in the absence of any RSV-specific data (Table S6); ii) no vial sharing; iii) attenuating the duration of long-term respiratory morbidity at 6 or 13 years of age.
Software
All analyses and modelling were undertaken using WinBUGS, SPSS and Microsoft Excel 365.
Results
Colombian-specific version of the IRST
Data on 81 cases and 49 controls were collected (Table S7). Generating the IRST using Colombian data with wGA substituting for chronological age resulted in an AUROC of 0.751 (Figure S2). Predictive accuracy was improved by adding lack of exclusive breastfeeding or mixed breastfeeding, with the latter providing the higher AUROC (0.791 vs 0.803, respectively; Figure S3 & Figure S4). Adding maternal education to primary level together with mixed breastfeeding proved the most predictive combination with an AUROC of 0.823 (95% CI 0.723–0.923; Fig. 2). Within this analysis, wGA contributed approximately 16% to the overall discrimination between infants with versus without RSVH.Fig. 2. Predictive accuracy of the Colombian-specific version of the IRST. AUROC: 0.823 (95%CI 0.723 – 0.923). Included risk factors: Gestational age; smokers and/or maternal smoking; siblings and/or daycare attendance; mixed breastfeeding (lack of breastfeeding plus formula); maternal education to primary level or less. AUROC Area under the receiver operating characteristic curve, with 1 representing perfect predictive accuracy, IRST International Risk Scoring Tool
The RSVH rate for the moderate- and high-risk group in the Colombian-specific IRST was recalculated to be 18.6% (Table 3).Table 3RSVH rates for each risk group in the Colombian-specific IRSTRisk groupRSVH risk, median % (95% CI)High41.0% (22.7–100.0%)High and moderate18.6% (12.3–31.9%)Moderate7.4% (3.6%–16.4%)Low1.8% (0.7–3.0%)CI Confidence interval, IRST International Risk Scoring Tool, RSVH respiratory syncytial virus hospitalization
Cost-effectiveness of the Colombian-specific version of the IRST at guiding palivizumab prophylaxis
For 32–35wGA infants scored at moderate- and high-risk by the Colombian-specific IRST, palivizumab increased treatment costs, but resulted in reduced direct and indirect healthcare costs and improved quality of life compared to no prophylaxis (Table 4). The resultant ICUR/QALY was COP20,225,126 (USD4,752), over 25% below the Colombian WTP threshold of COP28,193,734 (USD6,624).Table 4. Incremental costs and utilities for palivizumab versus no prophylaxis using the Colombian-specific IRST to identify 32–35wGA infants at moderate- and high-risk of RSVHNo Palivizumab****PalivizumabTreatment costs (COP)0.007,790,674.32Direct costs (COP)4,576,068.981,077,500.22Difference in costs (COP)4,292,105.56QALYs20.20720.419Difference in QALYs0.212**ICUR (COP) per QALY gained**20,225,126.34COP Colombian peso*, ICUR* incremental cost utility ratio*, IRST* international risk scoring tool*, QALY* quality adjusted life year*, RSVH* respiratory syncytial virus hospitalization, wGA weeks’ gestational age
Sensitivity analyses
The PSA resulted in a mean ICUR of COP22,193,734/QALY (USD5,214), with an 61.1% probability of palivizumab being cost-effective at a COP28,193,734 (USD6,624) WTP threshold (Fig. 3 and Figure S5). In the DSA, the cost-utility model was found to be most sensitive to: the mean number of palivizumab injections; palivizumab cost (100 mg); utility scores; RSVH rate; and palivizumab efficacy (Figure S6).Fig. 3. Cost-effectiveness acceptability curve for palivizumab prophylaxis (vs no prophylaxis) in moderate- and high-risk 32–35 wGA infants identified by the Colombian-specific IRST. Results are based on the probabilistic analysis after 10,000 Monte Carlo simulations. The curve represents the difference in costs and benefits between prophylaxis and no prophylaxis. COP Colombian peso, IRST international risk scoring tool, PVZ palivizumab, QALY quality-adjusted life year, wGA weeks’ gestational age
Scenario analyses
Inclusion of societal costs improved the ICUR/QALY gained for palivizumab versus no prophylaxis to COP18,282,582 (USD4,296) (Table 5). Conversely, removing vial sharing and attenuating the duration of long-term respiratory morbidity to 6 or 13 years of age increased the ICUR/QALY to COP29,059,655 (USD6,828), COP38,015,084 (USD8,932), and COP26,350,141 (USD6,191), respectively, albeit the latter was still under the Colombian WTP threshold (COP28,193,734 [USD6,624]).Table 5. Results of scenario analysesICUR per QALY gained(COP)ScenarioAs per scenarioBase caseInclusion indirect/societal costsBase case: direct costs only18,282,582.1320,225,126.34No vial sharingBase case: 70% vial sharing (5% wastage)29,059,654.6613 years duration of long-term respiratory morbidity in affected infants6 years duration of long-term respiratory morbidity in affected infantsBase case: 18-year respiratory morbidity26,350,141.1738,015,084.47COP Colombian peso, ICUR incremental cost-utility ratio, QALY quality adjusted life year, RSVH respiratory syncytial virus hospitalization
Discussion
In this first assessment of the IRST in LATAM, a localized version of the IRST was found to be highly predictive at determining the risk of RSVH in Colombian 32–35 wGA infants. Utilization of this Colombian-specific version of the IRST to target palivizumab prophylaxis to 32–35 wGA infants at moderate- or high-risk of RSVH was subsequently demonstrated to be a cost-effective strategy (versus no prophylaxis) from the perspective of the Colombian healthcare system. These results support the relevance of the IRST across LATAM and that use of the Colombian version should be adopted and assessed prospectively to guide palivizumab prophylaxis to 32–35 wGA infants in routine clinical practice in Colombia.
Generating a Colombian version of the IRST, with wGA substituted for chronological age, resulted in an AUROC of 0.751, which compared very favourably with an AUROC of 0.773 for the original IRST and 0.707 in the validation exercise using data from the RSV Preterm Risk Estimation Measure for RSVH in Ireland study (PREMI) [14, 47]. Importantly, our results indicate that in endemic (non-seasonal) RSV environments, such as in Colombia, wGA may be a suitable substitute for birth relative to the RSV season start. The Colombian version of the IRST was further refined by adding maternal education to primary level (as a surrogate for social deprivation) together with mixed breastfeeding, two risk factors considered of particular relevance in LATAM, producing a highly predictive AUROC of 0.823. Social deprivation is known to be associated with poorer health outcomes and more limited access to healthcare, particularly in LMICs [48], as well as being a specific risk factor for RSVH [49]. Similarly, lack of breastfeeding is well-recognized as an important risk factor for RSVH in 32–35 wGA infants and, indeed, was the next most predictive variable apart from those included in the original IRST [50, 51]. In addition to increasing the predictive power, the inclusion of mixed breastfeeding in the Colombian IRST provides an opportunity to encourage exclusive breastfeeding for these premature infants, in line with WHO recommendations [52]. The RSVH rate for the moderate- and high-risk group in the Colombian-specific IRST was 18.6%, which is similar to that reported for infants with CLD [4], who receive routine palivizumab prophylaxis in Colombia [12].
We recognize that the risk factor data collected in this study is limited both in terms of including only two Colombian hospitals over a brief, 4-month period and a relatively small sample size (81 cases; 49 controls). This may have resulted in overperformance of the Colombian-specific IRST (AUROC 0.823) and wide confidence intervals (CIs) on the RSVH rates, particularly for the high-risk group (95% CI 22.7–100.0%). Albeit the latter is somewhat mitigated by the fact that the cost-utility analyses were predicated on infants classified as moderate- or high-risk for RSVH where the uncertainty was more constrained (95% CI 12.3–31.9%). The substitution of chronological age for gestational age engenders a different predictive mechanism, from seasonal timing (including immune maturation, declining maternal antibodies, and exposure patterns) to static developmental status at birth, respectively, and requires further study and confirmation of validity. Despite these caveats, this study has demonstrated the value of undertaking localization of the IRST for populations that are not well represented in the underlying dataset. The improved predictive power engendered by localizing the IRST enables prophylaxis to be better targeted to those 32–35 wGA infants at greatest risk of RSVH specifically in Colombia. It is recommended that a larger prospective validation be included as part of the deployment of the IRST in any other country.
When the Colombian-specific IRST was used to identify 32–35 wGA infants at moderate- and high-risk of RSVH for prophylaxis, a new cost-utility analysis produced an ICUR/QALY of COP20,225,126 (USD4,752) (mean: COP22,193,734/QALY [USD5,214]) for palivizumab versus no prophylaxis. This equated to a 61.1% probability of palivizumab being cost-effective against a WTP threshold of COP28,193,734 ([USD6,624], the Colombian GDP per capita). Of note, palivizumab was borderline cost-effective with no vial sharing (COP29,059,655 [USD6,828]) and was below the WTP threshold in an analysis where respiratory morbidity was curtailed at 13 years (COP26,350,141 [USD6,191]). It is now widely acknowledged that long-term respiratory morbidity following RSVH in infancy can extend throughout childhood [33, 53]; hence, this scenario can be viewed as conservative.
It is difficult to compare our cost-utility analysis to those previously published for palivizumab use in Colombia, one of which found prophylaxis not to be cost-effective [11] and the other dominant (cost saving) [13], due to several salient differences in the comparative model structures, assumptions and inputs. Most importantly, our analysis focused on healthy 32–35 wGA infants at moderate- or high-risk of RSVH as identified by the Colombian-specific IRST, whereas the previous models assessed all < 35 wGA infants (with [11] or without CLD [13]). This resulted in differing RSVH rates being used in the analyses, further amplified by the limited epidemiological data on RSV in Colombia. In the analysis from 2013 [11], the RSVH rate of 10.6% was drawn from the IMpact study [7], whereas the 2024 study used a very high rate of 34.9% derived from hospitalized infants in the SENTINEL1 study [13, 54]. Due to the aforementioned lack of Colombian epidemiological data, we assumed an RSVH rate of 7.6% in our analysis, which was used to adjust the RSVH risk for the low-, moderate- and high-risk groups within the IRST. A 7.6% RSVH rate can be considered reasonable and somewhat conservative with reports of rates between 10 and 12% in preterm infants < 36–37 wGA from Brazil and Peru, albeit these studies included those with CLD who were born < 32 wGA [55, 56]. Further studies are required to quantify the true burden of RSV in healthy Colombian 32–35 wGA infants. Other differences between our analysis and the two previous publications include the efficacy rates used for palivizumab drawn from the IMpact study [7, 21] (82.2% in our model for 32–35 wGA infants; 78.1% in the 2024 analysis for ≤35 wGA infants without CLD [13]; 54.7% in the 2013 analysis for ≤35 wGA infants including those with CLD) [11], and the inclusion (our analysis and 2024 analysis [13]) or not (2013 analysis [11]) of MARI, further compromise direct comparisons. Limitations for all three analyses include a universal lack of country-specific utility scores and long-term respiratory morbidity data [11, 13], which have been addressed in detail elsewhere [15]. In brief, whilst recent data have further elucidated the impact of RSV on QoL [57, 58] these data are derived from a much broader population of children than considered in our model and did not report a disutility for hospitalized infants. As such, the data from Greenough et al. [27] used herein arguably remain the best source of utilities following RSVH in premature infants. Similarly, utility data on the ongoing effect of long-term respiratory morbidity on a child’s health following RSVH is not available, necessitating the use of a surrogate value derived from a study of the QoL impact of asthma. Finally, whilst there is a growing body of evidence that palivizumab [34–36], and the newer long-acting monoclonals [59], can reduce long-term respiratory morbidity, there remains some degree of uncertainty about the size and, particularly, duration of effect. Utilization of data from three studies of palivizumab in our model minimizes some of this uncertainty [34–36].
Despite these limitations, confidence in the results of our cost-utility analysis comes from the ICUR/QALY (COP20,225,126 [USD4,752]) not only being lower than the Colombian cost-effectiveness threshold of 1 GDP per capita derived from the World Bank [45] (COP28,193,734 ([USD6,624]) but also that reported by the Central Bank of Colombia [60] (COP26,222,387 [USD6,161]), and two alternative WTP thresholds that have been postulated (USD5,043 [61] and USD6,060 [62]). Under the guidance from the World Health Organization (WHO) [63], our base case can be considered ‘highly cost-effective’, being under 1 GDP, with the more conservative scenarios (including when respiratory morbidity was curtailed at 6 years of age) classed as ‘cost-effective’, falling withing the range 1–2x GDP. These facts, combined with the sensitivity and scenario analyses conducted, enhance the validity of our findings against any uncertainty in the assumptions and inputs.
Conclusion
Our study has confirmed that the Colombian specific IRST provides a potentially effective method to identify 32–35 wGA infants who are most likely to benefit from palivizumab prophylaxis. Furthermore, prophylaxis of these moderate- and high-risk 32–35 wGA infants with palivizumab was demonstrated to be cost-effective versus no intervention. These results also encourage the exploration and use of the IRST to guide the cost-effective use of palivizumab in 32–35 wGA infants across LATAM.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ministerio de Salud y Protección Social. Actualización de La Recomendación Sobre El Uso de Palivizumab. Available at: https://gpc.minsalud.gov.co/gpc_sites/Repositorio/Conv_500/GPC_rnp/gpc_rnp_completa.aspx. Accessed October 29, 2024.
- 2Colombia Prices Paid Data. 2022 Available at: https://web.sispro.gov.co/Web Publico/Consultas/Consultar CNPM Cadena Comercializacion Circu 2y PA_028_2_2.aspx. Accessed October 29, 2024.
- 3Economic Research Institute. Registered Nurse Salary in Colombia. 2022. Available: https://www.erieri.com/salary/job/registered-nurse/colombia#:%7E:text=The%20average%20pay%20for%20a,education%20for%20a%20Registered%20Nurse. Accessed October 29, 2024.
- 4Dirección de Censos y Demografía (DANE). Weeks of gestational age and weight 2021. Available at: https://www.dane.gov.co/index.php/acerca-del-dane/informacion-institucional/organigrama/direccion-de-censos-y-demografia. Accessed October 29, 2024.
- 5Instituto de Evaluación Tecnológica en Salud. Manual para la elaboración de evaluaciones económicas en salud. 2014. Available at: https://www.iets.org.co/Archivos/64/Manual_evaluacion_economica.pdf. Accessed October 29, 2024.
- 6The World Bank. GDP per capita. Available at: https://data.worldbank.org/indicator/NY.GDP.PCAP.CN?locations=CO. Accessed 14 September, 2023.
- 7World Health Organization. Breastfeeding. 2024. Available at: https://www.who.int/health-topics/breastfeeding#tab=tab_2. Accessed October 29, 2024.
- 8Central Bank of Colombia. Available: https://www.banrep.gov.co/es. Accessed October 29, 2024.