Bridging practice and evidence: insights from the Scandinavian Society of Anaesthesiology and Intensive Care Medicine and Saudi Critical Care Society Guidelines on trauma-related VTE
Marwa Amer, Waleed Alhazzani, Morten Hylander Møller, Faisal A. Al-Suwaidan, Mohammed Alshahrani

TL;DR
This paper presents clinical guidelines for preventing blood clots in trauma ICU patients, developed by international experts and tailored for different healthcare settings.
Contribution
The paper introduces new, evidence-based trauma VTE prophylaxis guidelines with adaptable strategies for diverse clinical contexts.
Findings
The guidelines provide actionable recommendations for timing, agent selection, and mechanical prophylaxis in trauma patients.
They emphasize adaptability for both high-resource and low-resource settings.
The guidelines highlight the importance of evidence-based practices and adherence strategies in trauma care.
Abstract
Trauma-related venous thromboembolism (VTE) represents significant challenges in clinical care for patients with critical illnesses, highlighting the need for evidence-based recommendations. The Saudi Critical Care Society (SCCS), in collaboration with international experts, developed the “VTE Prophylaxis in Trauma Intensive Care Unit Patients” clinical practice guidelines. The guidelines were developed using the Grading of Recommendations, Assessment, Development, and Evaluation methodology and provide consensus-based, actionable recommendations tailored to diverse clinical contexts. This article highlights key aspects of the guidelines, emphasizing practical implementation strategies for trauma VTE prophylaxis management. The trauma VTE prophylaxis guidelines, endorsed by the Scandinavian Society of Anaesthesiology and Intensive Care Medicine (SSAI), focus on the timing of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
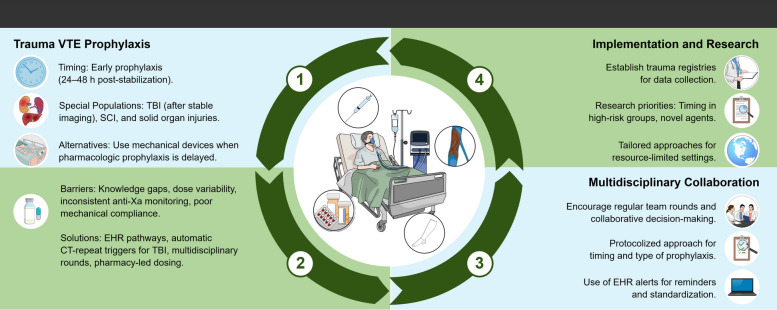 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVenous Thromboembolism Diagnosis and Management · Mechanical Circulatory Support Devices · Trauma, Hemostasis, Coagulopathy, Resuscitation
Background
Trauma-related venous thromboembolism (VTE) in patients with critical illnesses is a key challenge in intensive care, as it contributes to significant morbidity and mortality globally [1]. These challenges highlight the urgent need for standardized, evidence-based guidelines to optimize quality of care in this high-risk population [2].
The Saudi Critical Care Society (SCCS) developed the Trauma VTE Prophylaxis Guidelines to provide a structured framework for optimizing VTE prevention in patients with trauma, addressing both standard-risk and high-risk populations [2–4]. The guidelines focus on key clinical domains, including timing of prophylaxis initiation, pharmacologic agent selection, and the use of mechanical prophylaxis strategies. These guidelines were subsequently reviewed and formally endorsed by the Scandinavian Society of Anaesthesiology and Intensive Care Medicine (SSAI). The guidelines are grounded in the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology, ensuring that their recommendations are informed by high-quality evidence and structured evaluation tools, including the Population, Intervention, Comparison, and Outcome (PICO) framework [5, 6]. This systematic approach enhances transparency, standardizes decision-making, and improves the applicability of various recommendations across diverse clinical contexts [7].
The guidelines were developed by multidisciplinary expert panels from clinical pharmacy, medicine, and critical care disciplines to emphasize the importance of collaboration and patient-centered care. By integrating robust evidence frameworks, including GRADE and PICO, we ensure the credibility, feasibility, and broad applicability of these recommendations to bridge the gaps between evidence and practice.
Here, we present key highlights of the guidelines, summarize actionable recommendations, and discuss the importance of evidence-based practices. We also propose strategies to improve adherence through standardized protocols, training programs, and multidisciplinary collaboration and address their implementation in diverse settings to emphasize adaptability to resource-constrained environments and particular populations. Finally, we call for action regarding future research to refine practices, address knowledge gaps, and optimize outcomes in trauma and critical care.
Main text
Key highlights of the guidelines
Table 1 summarizes key recommendations from the Trauma VTE Guidelines. Table 1. Key recommendations from the Trauma Venous Thromboembolism (VTE) guidelinesClinical scenarioRecommendationStrength of evidencePractical considerationsTrauma VTE guideline: the full evidence profiles and decision frameworks can be accessed hereVTE Prophylaxis in Blunt Solid Organ InjuriesInitiate pharmacological VTE prophylaxis within 24–48 h in patients with low-risk blunt solid organ injuries who are being managed non-operativelyConditional, very lowExclude patients with hemodynamic instability, active bleeding, or high-grade injuries. Regularly assess bleeding riskVTE Prophylaxis in Isolated Blunt TBIEarly pharmacological VTE prophylaxis (24–72 h post-injury) for low-risk patients with stable brain imaging and neurological examination resultsConditional, very lowAvoid patients who are considered high-risk and require neurosurgical intervention. Use mechanical prophylaxis as a bridge until stabilizationSpine Trauma or SCIFor non-operative spine trauma or SCI, initiate pharmacological VTE prophylaxis within 24–48 h. Initiate within 48 h post-fixation for surgical casesConditional, very lowBegin mechanical prophylaxis early for all patients with SCIs. Consider IVCFs if pharmacological options are delayed or contraindicatedPreferred Pharmacologic AgentPrefer LMWH (e.g., enoxaparin and dalteparin) over UFH for patients with trauma who are receiving pharmacologic prophylaxisConditional, lowUse UFH for patients with renal impairment (e.g., creatinine clearance < 30 mL/min). Monitor for HITDose of Pharmacologic VTE ProphylaxisUse either intermediate-high dose (e.g., enoxaparin 40 mg subcutaneously every 12 h) or conventional dosing of LMWH in patients who are at low risk of bleedingConditional, very lowAvoid intermediate-high dosing in patients who are at high risk of bleeding (e.g., age > 65 years, weight < 50 kg, those with low creatinine clearance, or patients with TBI or SCI who are at high risk for bleeding)Use of Mechanical ProphylaxisInitiate mechanical prophylaxis (e.g., pneumatic compression devices) for all patients with trauma who are unable to receive pharmacologic prophylaxisStrong, very lowEnsure proper device placement and monitor for skin breakdown or discomfort during prolonged useAdjunct Mechanical ProphylaxisConsider adjunct use of mechanical prophylaxis for additional protection in patients with trauma receiving pharmacologic prophylaxisConditional, very lowAdjunctive strategies can be tailored to patient-specific risk profilesRoutine Duplex Ultrasound SurveillanceIn high-risk patients with trauma who are unable to receive pharmacologic prophylaxis, use routine bilateral lower extremity ultrasound screening to detect asymptomatic DVTConditional, very lowNot applicable to ambulatory patients, low-risk patients with trauma, or those with symptoms indicating diagnostic imagingProphylactic IVCFsAvoid routine placement of prophylactic IVCFs in patients with traumaConditional, very lowTemporary retrievable IVCFs may be considered for patients who are unable to receive pharmacological VTE prophylaxis for > 7 days (e.g., because of ongoing bleeding risk)Abbreviations: DVT deep venous thrombosis, HIT heparin-induced thrombocytopenia, IBW ideal body weight, IVCFs inferior vena cava filters, LMWH low-molecular-weight heparin, SCI spinal cord injury, TBI traumatic brain injury, UFH unfractionated heparin
Risk stratification and prophylaxis timing
Personalized risk stratification is the cornerstone of VTE prevention in patients with trauma.
- Clinical Practice Point: Utilize validated tools, including the Caprini score or Padua Prediction Score, to assess VTE risk and tailor prophylaxis accordingly.
- Timing Recommendation: Initiate pharmacologic prophylaxis with low-molecular-weight heparin (LMWH) within 24–48 h of trauma stabilization, provided bleeding risks are controlled. For high-risk cases, use mechanical prophylaxis (intermittent pneumatic compression [IPC] devices) until pharmacological options are feasible [8].
Pharmacological prophylaxis
LMWH is considered the first-line agent because of its favorable safety profile and efficacy in preventing VTE (conditional recommendation, low certainty of evidence) [9].
Dosing Adjustments: Adjust doses for weight and renal function; monitor anti-Xa levels in patients with obesity or critical illnesses [10].
Mechanical prophylaxis
IPC devices serve as effective alternatives for patients with contraindications for pharmacologic prophylaxis (strong recommendation, very low certainty of evidence) [1, 2].
Practical Tip: Ensure proper device application and consider sequential compression devices for enhanced efficacy.
Special populations
- Solid Organ Injuries: Early initiation (24–48 h post-injury) is recommended in adults with blunt solid organ injuries to the liver, spleen, or kidney who are managed nonoperatively and have controlled bleeding or low hemorrhagic risk, as this strategy has been associated with reduced VTE events without increased failure of nonoperative management or bleeding complications [11–13]. Conversely, in patients at high risk of major bleeding—including those with high-grade solid organ injuries, large hemoperitoneum, or ongoing transfusion requirements—pharmacologic prophylaxis should be deferred until hemostasis and physiological stability are confirmed, with mechanical prophylaxis used as a bridging strategy during this period (conditional recommendation, very low certainty of evidence) [14, 15].
- Traumatic Brain Injury (TBI): Prophylaxis initiation requires confirmation of radiographic stability (24–72 h post-injury) [16]. Recent large-scale data from the Trauma Quality Improvement Program database demonstrate significant inter-hospital variation in the timing of VTE pharmacologic prophylaxis among patients with TBI, with earlier initiation (24–48 h) correlating with lower adjusted trauma and TBI-related mortality [17]. Despite the historical hesitation to initiate pharmacologic prophylaxis early in TBI due to bleeding risk, early VTE pharmacologic prophylaxis was not associated with higher hemorrhagic complications in this cohort of patients with non-neurosurgical TBI. Observational and propensity-matched cohort studies have demonstrated that initiation within 24–72 h of injury is associated with lower rates of VTE without increased risk of intracranial hemorrhage progression, repeat neurosurgical intervention, or mortality [18, 19]. Therefore, the SCCS recommendation to consider VTE pharmacologic prophylaxis within 24–72 h (conditional recommendation, very low certainty of evidence) based on repeat imaging and clinical stability aligns with high-performing trauma center practices and can be emphasized as a quality measure in regional trauma systems.
- Spinal Cord Injuries (SCI): Early initiation (24–48 h post-injury) is advised in adults with isolated spine trauma or fracture and/or SCI with low bleeding risk, who are managed non-operatively, thereby balancing hematoma risk with VTE prevention (conditional recommendation, very low certainty of evidence) [20, 21].
Inferior vena cava filters
The guideline discourages routine use of inferior vena cava filters for primary prophylaxis due to potential complications and limited evidence of survival benefits. Selective use is recommended for patients with VTE who have contraindications to anticoagulation, accompanied by structured follow-up to ensure retrieval and minimize complications (conditional recommendation, very low certainty of evidence) [22].
Ultrasound surveillance
Routine duplex ultrasonography surveillance in patients with trauma remains controversial, and practice varies substantially across trauma systems. While some centers continue scheduled (e.g., weekly) screening of selected high-risk, asymptomatic patients—particularly when pharmacologic prophylaxis is delayed or contraindicated—routine surveillance is not recommended for most patients with trauma. Consistent with our guidelines’ recommendation, a selective approach may be considered for patients at elevated VTE risk who are not candidates for pharmacologic prophylaxis (conditional recommendation; very low certainty of evidence) [1, 2]. This recommendation reflects the limited and methodologically heterogeneous evidence base, which consists largely of single-center observational studies and one randomized trial showing reduced in-hospital pulmonary embolism (PE) without a demonstrable mortality benefit [23].
Routine surveillance substantially increases detection of asymptomatic or distal deep vein thrombosis, raising concern for overdiagnosis and potential downstream anticoagulation-related harm without clear improvement in patient-important outcomes. In this context, the potential benefits of surveillance should be weighed against surveillance bias, increased detection of clinically uncertain events, and uncertain impact on patient-important outcomes, particularly PE [24–26]. Diagnostic ultrasonography should remain reserved for patients with clinical signs or symptoms of deep vein thrombosis, and routine surveillance should be avoided in ambulatory or low-risk patients.
Bridging global and local practices
The guidelines integrate global evidence with region-specific considerations, ensuring practical applicability across diverse healthcare environments. While aligned with international standards, including those of the Western Trauma Association (WTA) and the American Association for the Surgery of Trauma (AAST) Critical Care Committee Clinical Consensus Document, the SCCS guidelines prioritize flexibility to address unique challenges in high- and low-resource settings [25, 26]. Table 2 compares the SCCS guidelines to those of the WTA and AAST. The WTA algorithms and AAST Critical Care Committee Clinical Consensus Document emphasize expert-driven consensus and pragmatic decision-making, whereas the SCCS guideline prioritizes formal evidence certainty grading and explicit benefit–harm trade-offs through GRADE. Table 2. Comparison of trauma-related VTE prophylaxis recommendations across SCCS, WTA, and AAST guidanceAspectSCCS Guidelines (Endorsed by SSAI)WTA algorithmsAAST critical care committee clinical consensus documentAgent SelectionRecommend LMWH over UFH as the preferred pharmacological agent (conditional recommendation, low certainty of evidence)Recommend LMWH over UFH based on strong evidence for VTE prevention and reduced risk of HITRecommends LMWH over UFH based on similar evidenceStandard LMWH DoseAdvocate for either intermediate–high dose LMWH (enoxaparin 40 mg every 12 h) or conventional dosing LMWH (conditional recommendation, very low certainty of evidence)Recommend 40 mg of LMWH every 12 h to achieve target anti-factor Xa levels, which is higher than older recommendations (30 mg every 12 h)Recommends 40 mg of LMWH every 12 h for most patientsTiming of InitiationEmphasize early initiation, ideally within 24–48 h of trauma stabilization if bleeding risks permit (conditional recommendation, very low certainty of evidence)Recommend initiation within 24 h of injury if bleeding is controlledRecommends immediate initiation for patients without active bleeding or high-risk injuries; otherwise, delays depend on specific conditionsHigh-Risk InjuriesHighlight special considerations for TBI, SCI, and solid organ injuries with tailored timingRecommend starting within 24 h of bleeding cessation or stabilization of injuriesRecommends using Modified Berne–Norwood Criteria for TBI and starting within 48 h for spinal cord or solid organ injuriesProphylaxis Dose in High-Risk PopulationsSuggest lower initial doses for patients with high-risk injuries, particularly TBI, SCI, and high risk of bleeding (conditional recommendation, very low certainty of evidence)Recommend a lower dose (30 mg LMWH every 12 h) for high-risk injuries, reflecting safety concerns with higher dosesFollows similar dosing for high-risk populations (30 mg every 12 h)Missed DosesStress the importance of continuous thromboprophylaxis, minimizing interruptions unless clinically unavoidableEmphasize continuous prophylaxis without interruption. Missed doses significantly increase VTE riskStresses continuous prophylaxis and advises against holding LMWH for most surgical procedures, except spinal fixationDose AdjustmentsAdvocate for adjusting LMWH doses based on weight, anti-Xa levels, renal function, and specific populationsDiscuss weight-based dosing (0.5 mg/kg every 12 h) and adjustments to achieve target anti-Xa levelsRecommends similar weight-based dosing and anti-Xa adjustments. Additionally, emphasizes adjustments for renal impairmentSpecial PopulationsSuggest dose adjustments for older patients, those with low body weight, pregnant individuals, and those with renal impairmentRecommend lower dosing (30 mg every 12 h) for CrCl 30–60 mL/min, older patients (aged > 65 years), those with low body weight (< 50 kg), and pregnant patientsSimilar recommendations for these populations, adding the use of UFH for those with CrCl values of < 30 mL/minAbbreviations: AAST American Association for the Surgery of Trauma, CrCl Creatinine Clearance, HIT heparin-induced thrombocytopenia, LMWH low-molecular-weight heparin, SCI spinal cord injury, SCCS Saudi Critical Care Society, TBI traumatic brain injury, UFH unfractionated heparin, VTE venous thromboembolism, WTA Western Trauma Association
Discussion
Role of evidence-based guidelines in trauma management
Evidence-based guidelines are central to optimizing trauma care in the setting of profound patient heterogeneity, competing risks of thrombosis and bleeding, and time-critical decision-making. The SCCS guidelines for VTE prophylaxis in patients with trauma provide structured, actionable recommendations grounded in systematically appraised evidence and transparent benefit–harm assessment [1, 2]. By explicitly prioritizing patient safety, feasibility, and resource stewardship, the guidelines offer a pragmatic framework for navigating complex clinical scenarios frequently encountered in trauma intensive care units (ICUs). These priorities closely align with Scandinavian trauma and critical care systems, which emphasize equity, data-driven practice, and continuous quality improvement supported by national registries and standardized care pathways.
Methodological considerations in trauma guidelines development
The conditional nature of many trauma-related VTE prophylaxis recommendations reflects fundamental methodological limitations within the trauma evidence base rather than a lack of clinical importance or equipoise. A recent systematic review of randomized trials in traumatic hemorrhage demonstrated frequent overestimation of treatment effects, inaccurate baseline risk assumptions, and high rates of futility-driven trial termination, undermining confidence in effect estimates and limiting the certainty of downstream recommendations [27]. These challenges help explain why many widely adopted trauma practices continue to rest on low- or very low-certainty evidence.
This methodological fragility is particularly evident in the literature addressing the timing of pharmacologic VTE prophylaxis in TBI. Despite decades of observational research, the optimal initiation strategy remains unresolved—not because of contradictory findings, but due to pervasive bias, heterogeneity, and lack of clinically meaningful endpoints. A contemporary systematic review identified 21 studies evaluating prophylaxis timing in adult TBI; 20 were judged to be at critical risk of bias using the ROBINS-I tool, and none provided high-certainty evidence applicable to patients with severe TBI or those undergoing neurosurgical intervention [28]. Substantial heterogeneity in definitions of “early” prophylaxis, injury severity classification, radiographic stability criteria, pharmacologic agents, and neurosurgical management precluded meta-analysis and limited generalizability. Consequently, the field remains unable to definitively answer the core clinical question: when is it safe to initiate pharmacologic prophylaxis in TBI?
These evidence limitations carry important clinical consequences. Concern regarding intracranial hemorrhage progression remains a dominant driver of delayed prophylaxis, particularly in patients with severe injuries, evolving radiographic findings, or recent neurosurgical procedures. Although observational data increasingly suggest that earlier prophylaxis may be feasible in carefully selected low-risk patients, these data lack the granularity required to inform decision-making in higher-risk scenarios.
From a guideline methodology perspective, this uncertainty explains why contemporary trauma guidelines, including the SCCS recommendations endorsed by the SSAI, deliberately avoid rigid, time-based initiation thresholds for VTE prophylaxis in TBI. Instead, recommendations emphasize radiographic stability on repeat computed tomography and neurological stability on clinical examination as the most reliable anchors for clinical judgment. This stability-based approach acknowledges the low certainty of evidence, accommodates biological heterogeneity, and aligns with Parkland- and Berne–Norwood-style risk stratification frameworks, prioritizing patient safety over arbitrary temporal targets.
Implementation and adherence to guideline challenges
Despite the availability of comprehensive, methodologically robust guidelines, real-world adherence to trauma-related VTE prophylaxis recommendations remains inconsistent, driven by challenges in dissemination, education, and bedside implementation [29]. Persistent practice variation reflects not only operational barriers but also the unresolved nature of the underlying evidence, particularly in high-risk populations such as patients with TBI.
A large contemporary survey of trauma surgeons illustrates this evidence–practice gap. Although more than 90% of respondents reported an intention to initiate pharmacologic prophylaxis within 72 h of TBI, self-reported adherence to institutional protocols ranged from only 25% to 75% of eligible patients [30]. Common drivers of deviation included concern for intracranial hemorrhage progression, disagreement between trauma and neurosurgical teams, and clinical scenarios insufficiently addressed by existing guidelines. These findings highlight a critical tension between guideline intent and bedside decision-making, wherein clinicians are compelled to rely on individualized judgment in the absence of high-certainty evidence—particularly for patients with severe TBI or following neurosurgical intervention [31]. In this context, guideline recommendations emphasizing radiographic stability, neurological examination, and multidisciplinary consensus—rather than rigid time-based thresholds—represent a pragmatic and methodologically defensible response to uncertainty. Such recommendations acknowledge residual evidence gaps while providing clinically meaningful anchors for decision-making in complex and evolving trauma scenarios.
Importantly, non-adherence is not limited to decisions regarding when to start prophylaxis. Even after pharmacologic VTE prophylaxis is prescribed, missed doses of LMWH represent a frequent and clinically meaningful implementation failure. Evidence from implementation studies indicates that most missed doses are attributable to patient refusal rather than clinical contraindications, highlighting that adherence challenges extend beyond clinician decision-making to patient understanding and engagement [32]. These failures contribute to preventable variation in care delivery despite nominal guideline compliance.
Enhancing adherence and making guidelines implementable
Improving adherence to trauma VTE prophylaxis guidelines requires translation of recommendations into reliable clinical workflows rather than further expansion of the evidence base [33–35].
Figure 1 illustrates algorithmic decision-making pathways used in trauma-related VTE prophylaxis guidelines, emphasizing injury severity, radiographic stability, and neurological assessment to enhance bedside applicability.Fig. 1. Summary of key insights and implementation priorities. The figure provides a visual synthesis of how the guidelines translate into real-world ICU care and highlights their adaptability across diverse clinical contexts. • Trauma VTE Prophylaxis: Emphasizes early pharmacologic prophylaxis (within 24–48 h post-stabilization), with special considerations for high-risk populations such as those with TBI, SCI, and solid organ injuries. Mechanical prophylaxis is recommended when pharmacologic options are delayed or contraindicated. • Multidisciplinary Collaboration: Encourages structured team communication, protocol-driven prophylaxis, and integration of electronic health record (EHR) alerts to standardize practice. • Implementation and Research: Calls for establishing trauma registries, prioritizing research in high-risk groups, and tailoring guidelines for resource-limited settings. Abbreviations: VTE – Venous thromboembolism; TBI – Traumatic brain injury; SCI – Spinal cord injury; EHR – Electronic health record; CT – Computed tomography; anti-Xa – Anti–factor Xa (activity/assay)
Several implementation-focused strategies have demonstrated effectiveness in reducing preventable practice variation:
- Targeted Education and Communication: Patient-centered education interventions, combined with nurse-focused training, directly address a common cause of missed prophylaxis doses—patient refusal. Implementation studies demonstrate that structured education bundles supported by real-time electronic prompts reduced missed LMWH doses from 12.9% to 9.3% and decreased patient refusal by approximately 50%, without altering pharmacologic strategy. These findings emphasize that communication quality, rather than drug selection or dosing, is a primary determinant of successful prophylaxis delivery.
- Standardized, Electronic Health Record (EHR)-Integrated Protocols: Institution-wide protocols aligned with guideline recommendations simplify decision-making and reduce unwarranted variation. Embedding these protocols into EHRs through order sets, reminders, and automated reassessment prompts supports consistent execution once prophylaxis is deemed safe to initiate. Beyond protocol embedding, system-level strategies to address missed or delayed prophylaxis are gaining attention. A pragmatic randomized clinical trial protocol describes an artificial intelligence (AI)–driven, EHR-integrated clinical decision support “nudge” that identifies hospitalized patients at high risk for hospital-acquired VTE who are not receiving prophylaxis and prompts reconsideration of prophylaxis orders [36]. Although this approach is not trauma-specific and outcome data are pending, it illustrates how AI-enabled decision support may complement standardized EHR protocols by improving adherence and reducing gaps in prophylaxis delivery; trauma-specific validation and effectiveness data remain necessary before such systems can inform guideline recommendations.
- Contextual and Regional Adaptation: Guideline implementability depends on alignment with local infrastructure and resources. In resource-limited settings, mechanical prophylaxis may serve as an interim strategy when pharmacologic options are delayed or unavailable. In Scandinavian trauma systems, high digital maturity, multidisciplinary ICU teams, and national quality registries—such as the Swedish Intensive Care Registry and the Danish Trauma Database—enable real-time monitoring of adherence, feedback, and continuous quality improvement. Within Saudi trauma systems, pragmatic approaches include embedding nurse-facing prompts and brief education scripts into EHRs; tracking missed-dose rates as a core VTE quality metric; and delivering concise patient-facing messages explaining the rationale for LMWH, the persistence of post-trauma VTE risk, and the safety of prophylaxis once imaging stability is confirmed.
- Interdisciplinary Collaboration: Close collaboration among pharmacists, intensivists, anesthesiologists, surgeons, and nurses mitigates implementation challenges by enabling shared risk assessment and coordinated decision-making. Routine multidisciplinary rounds allow dynamic reassessment of bleeding and thrombotic risk and support individualized, high-fidelity application of guideline recommendations—a practice increasingly adopted within Scandinavian and Saudi ICU cultures [37, 38].
Future research directions
Although the guidelines are comprehensive, critical knowledge gaps remain, particularly in high-risk subgroups and post-acute phases of care, where current recommendations rely largely on low- or very low-certainty evidence (Tables 3 and 4). Future research should prioritize studies that enroll under-represented trauma phenotypes, use standardized and clinically meaningful definitions and endpoints, and incorporate realistic baseline-risk estimates and effect-size assumptions to reduce trial futility and improve interpretability.
- High-risk injury patterns and timing decisions
- TBI: Prospective studies are needed in patients with severe TBI, especially those undergoing neurosurgical interventions (e.g., craniotomy, external ventricular drain placement, intracranial pressure monitoring), who remain systematically under-represented in existing datasets. Future trials should standardize definitions of radiographic stability, neurological stability, and clinically meaningful hemorrhage progression to enable reproducible, patient-centered risk stratification. Comparative effectiveness studies should evaluate stability-based initiation strategies versus fixed time-based thresholds using outcomes that reflect both safety and benefit (intracranial hemorrhage progression, VTE events, neurosurgical reintervention, and mortality) [39].
- SCI: Studies should determine whether earlier prophylaxis (< 48 h) confers clinically meaningful benefit across injury severity strata, including prospective risk stratification by neurological impairment (e.g., ASIA grade) and surgical versus non-surgical pathways.
- Solid Organ Injury: Evidence remains limited for penetrating trauma and high-grade injuries; future studies should explicitly examine these subgroups and report standardized bleeding and re-intervention outcomes to support safer generalization of timing recommendations.
- Cross-Cutting Priority: Across TBI and SCI populations, the field would benefit from harmonized definitions of “early” prophylaxis, standardized imaging-stability criteria, and consistent reporting of baseline risk to support pooled analyses and guideline certainty upgrades.
- Dose optimization and monitoring
- Dosing Strategies: Comparative trials should evaluate weight-based dosing, anti-Xa–guided adjustment, and viscoelastic testing–informed approaches using patient-important outcomes (symptomatic VTE, bleeding requiring intervention, mortality), rather than surrogate endpoints alone.
- Novel agents and evolving anticoagulant strategies
- Novel Agents: Non-heparin strategies remain investigational in trauma. Aspirin may warrant evaluation in carefully selected, lower-risk post-acute pathways where LMWH is not feasible; however, robust trauma-specific evidence is limited [40]. Direct oral anticoagulants (DOACs) raise important safety and reversibility concerns in bleeding-prone phenotypes (e.g., TBI) and should be avoided until trauma-specific safety data are available.
- Factor XI/XIa Inhibition: Emerging agents targeting factor XI or XIa (e.g., abelacimab, osocimab, milvexian) have shown reduced bleeding compared with DOACs in non-trauma populations; however, they have not been evaluated in acute trauma, TBI, or solid organ injury [41]. Accordingly, LMWH remains the foundation of pharmacologic prophylaxis in trauma care, and factor XI inhibitors should be regarded as investigational until trauma-specific trials establish safety and net clinical benefit.
- Post-discharge prophylaxis and late eventsAn under-recognized gap in trauma-related VTE prevention is the persistence of thrombotic risk after hospital discharge, with a substantial proportion of events occurring within the first three months following injury. Randomized trauma-specific trials are needed to define which phenotypes benefit from extended prophylaxis, optimal duration, and the safest regimens. Until such evidence is available, future studies should focus on defining risk thresholds (e.g., pelvic/lower-extremity fractures, SCI, prolonged immobility), bleeding-risk stratification, and patient-centered outcomes (symptomatic VTE, readmissions, patient-reported burden, and adherence) [42, 43].
- Economic evaluation and trial efficiencyCost-effectiveness analyses should be embedded within future trauma VTE research to evaluate economic viability across high-resource and resource-limited settings, including the incremental value of dose-adjustment strategies and post-discharge prophylaxis pathways. Scandinavian centers with experience in adaptive platform trial infrastructure (e.g., INCEPT) are well-positioned to support efficient multicenter evaluation using pragmatic enrollment and registry-enabled follow-up where feasible [44]. Future trials should also incorporate prognostic enrichment, realistic baseline-risk estimates, and clinically meaningful endpoints to strengthen the evidentiary foundation underpinning guideline updates. Table 3. Novel therapeutic medications for Venous Thromboembolism Prophylaxis (VTE)Therapeutic agentMechanism of actionPotential benefitsClinical considerationsDOACsInhibit specific clotting factors (e.g., Factor Xa and thrombin)- Fixed dosing and no routine monitoring- Oral administration- Limited data in populations with trauma- Contraindicated in active bleeding or unstable injuries- Availability and cost of reversal agents. Drug interactions with anticonvulsants in TBIAspirinInhibits platelet cyclooxygenase, reducing thromboxane A2 production and platelet aggregation- Simple administration- Potentially lower bleeding risk- Cost-effective for low-risk patients (Some orthopedic data available after a fracture) particularly in resource-constrained environments- Limited efficacy in high-risk patients with trauma- Not a substitute for anticoagulation in severe casesFactor XI / XIa InhibitorsSelective inhibition of factor XI or activated factor XIa, attenuating thrombin generation through the intrinsic pathway while preserving hemostasis mediated by the extrinsic pathway- Promising bleeding-sparing signals in selected non-trauma populations- No clinical data in trauma populations, including patients with TBI, solid organ injury, or active bleeding risk- Safety, timing, reversibility, and net clinical benefits in trauma remain unknown-LMWH remains the foundation of pharmacologic VTE prophylaxis in traumaAbbreviations: DOACs direct oral anticoagulants, LMWH low-molecular-weight heparin, TBI traumatic brain injuryTable 4Summary of strategies, findings, recommendations, and gaps in trauma-related VTE ProphylaxisAspectKeyfindingsRecommendationsResearch gapsCurrent Practices- LMWH is the preferred agent for pharmacological VTE prophylaxis- Fixed dosing regimens (e.g., 30 or 40 mg two times daily)- Mechanical prophylaxis using intermittent pneumatic compression devices for patients at high bleeding risk- Delayed initiation in high-risk patients (e.g., those with TBIs or solid organ injuries)- Continue the use of LMWH as a first-line agent- Implement fixed dosing with weight-based adjustments for patients with high body mass indexes- Utilize mechanical prophylaxis where pharmacological prophylaxis is contraindicated- Data comparing the effectiveness and safety of DOACs versus LMWH in trauma patients remain sparse, particularly among bleeding-prone phenotypes such as those with TBIs- Limited data on the long-term impact of extended prophylaxis in patients with traumaSolid Organ InjuriesEarly VTE prophylaxis (< 48 h) post-injury reduces VTE risk without increasing bleeding or failure of non-operative management- Initiate prophylaxis within 48 h in patients with blunt solid organ injuries being managed non-operatively, after confirming hemodynamic and radiographic stability- Limited evidence for high-grade injuries and penetrating trauma regarding safe prophylaxis timingTBILMWH post-radiographic stability (24–48 h) reduces VTE risk and may improve mortality- Confirm stability of intracranial bleeding before initiating prophylaxis within 48 h, using repeat imaging and clinical assessment- Limited data on heterogeneous TBI presentations, neurosurgical subgroups, and optimal timing for varied clinical scenariosSCIEarly initiation (< 72 h) is beneficial; evidence supports earlier use (< 48 h) in stable cases- Tailor prophylaxis based on injury level (cervical versus thoracic versus lumbar) and completeness of injury (ASIA classification)- Limited prospective data to define optimal timing thresholds across SCI severity, surgical pathways, and bleeding-risk strataImplementation Strategies- Education campaigns targeting clinicians to improve awareness- Real-time electronic alerts and reminders for timely prophylaxis- Audit and feedback loops to monitor adherence- Multidisciplinary rounds to tailor personalized patient care- Standardize education campaigns for hospital-wide implementation- Integrate electronic reminders into existing EHR systems- Foster collaboration through regular multidisciplinary meetings- Limited studies on long-term retention of knowledge from education programs- Inadequate data on the scalability of audit processes in low-resource settings- Few studies on the cost-effectiveness of these interventionsPatient-Centered InterventionsPersonalized education and involvement in care decisions improve acceptance of prophylaxis- Develop patient education materials and involve patients in prophylaxis planning, particularly for those who refuse injections such as LMWH- Sparse data on the effectiveness of patient-centered approaches in trauma-specific VTE preventionTailored Interventions for High-Risk PopulationsInjury-specific, tailored protocols may reduce practice variability and improve safety in patients with TBIs, SCIs, and solid organ injuries- Create tailored prophylaxis plans that incorporate injury patterns, timing and agent selection based on individual risks- Limited robust data for standardizing dose adjustments and initiation timing in high-risk populationsCost-Effectiveness StudiesEvaluating the financial implications of implementation strategies can justify investments in adherence-improving interventions- Conduct cost-effectiveness studies focusing on low-resource settings- Include economic evaluations in VTE research protocols to provide evidence for scaling successful interventions- Minimal evidence from low-resource settings on economic feasibility- Lack of comprehensive cost–benefit analyses comparing strategies such as electronic alerts and extended prophylaxisAbbreviations: DOACs direct oral anticoagulants, EHR electronic health record, LMWH low-molecular-weight heparin, SCI spinal cord injury, TBI traumatic brain injury, UFH unfractionated heparin, VTE venous thromboembolism
Evolving models of guideline development
Traditional clinical practice guidelines remain the cornerstone of evidence-based medicine because of their comprehensive scope, multidisciplinary consensus processes, and rigorous application of the GRADE framework. By addressing multiple PICO questions through full systematic reviews, these guidelines enable transparent balancing of benefits, harms, values, and resource considerations. However, their development is inherently resource-intensive, time-consuming, and dependent on sustained volunteer engagement, rendering them vulnerable to obsolescence in rapidly evolving clinical domains such as trauma and critical care [45].
To address these limitations, alternative guideline models have emerged. Rapid practice guidelines prioritize timeliness by focusing on narrowly defined, practice-changing clinical questions, enabling faster translation into care at the expense of breadth. Living guidelines extend this approach through continuous evidence surveillance and iterative updating but require substantial methodological infrastructure, stable funding, and coordinated expertise to remain sustainable. Each model, therefore, reflects a trade-off between scope, agility, and resource requirements.
Despite these differences, the GRADE framework remains foundational to trustworthy guideline development and clinical credibility. Hybrid approaches that integrate traditional GRADE methodology with streamlined evidence synthesis, prioritized question selection, and early engagement of end users may be particularly well-suited to trauma care, where evidence evolves incrementally, and implementation feasibility is as critical as statistical certainty [46].
Toward personalized VTE prophylaxis in trauma care
Beyond classical immobility-related risk factors, trauma induces a delayed prothrombotic phenotype characterized by platelet hyperreactivity, fibrinolysis shutdown, endothelial dysfunction, and immunothrombotic pathways, providing biological plausibility for sustained venous thromboembolism risk despite resolution of early bleeding concerns [47].
Against this biologically heterogeneous backdrop**,** most contemporary clinical practice guidelines are based on average treatment effects derived from randomized trials; however, these averages may not reflect individual patient responses—a phenomenon known as heterogeneity of treatment effects [48]. This limitation is particularly salient in trauma and critical care, where patients vary widely in injury patterns, bleeding risk, inflammatory response, and dynamic coagulation profiles.
Emerging work in critical care demonstrates that phenotype-informed strategies—such as individualized oxygen targets based on predicted treatment effects—may outperform population-level recommendations [49]. Translating similar principles to trauma-related VTE prophylaxis represents an important conceptual advance toward personalized thromboprophylaxis, particularly in populations where both thrombotic and hemorrhagic risks evolve rapidly over time.
Viscoelastic hemostatic testing can identify trauma-associated hypercoagulable phenotypes such as fibrinolysis shutdown, which are consistently associated with increased VTE risk [47]. While these modalities are well-established for guiding transfusion and hemorrhage management, current evidence is insufficient to support their routine use for individualizing pharmacologic VTE prophylaxis, and such applications should be regarded as investigational, given the predominance of observational data, heterogeneous definitions of hypercoagulability, and limited predictive performance for patient-important thrombotic outcomes [50].
Beyond viscoelastic hemostatic testing, multi-omics and biomarker-based approaches offer additional promise for individualized risk stratification. Early metabolomic and proteomic studies have demonstrated strong discriminatory performance for thrombotic risk prediction, although external validation and demonstration of clinical utility are still required before clinical adoption [51]. In trauma-specific cohorts, proteomic signatures distinguishing patients who develop VTE despite standard prophylaxis are beginning to reveal pathways related to coagulation, innate immunity, and endothelial activation, supporting future development of biomarker-informed strategies while remaining investigational at present [52].
Advances in digital health and AI may further support personalized and timely VTE prevention. AI-assisted radiology workflows have already reduced time to detect incidental PE, and future real-time risk prediction models integrating imaging, laboratory data, and clinical variables may eventually support adaptive, patient-centered decisions regarding prophylaxis initiation and escalation [53]. Collectively, these developments signal a shift from static, population-based recommendations toward dynamic, individualized thromboprophylaxis paradigms.
Call to action: “strengthening trauma research and implementation infrastructure”
Addressing persistent evidence and implementation gaps in trauma care will require sustained investment in research infrastructure and coordinated international collaboration [54]. Partnerships among funding agencies, professional societies, and healthcare institutions are essential to enable multicenter trials, facilitate data sharing, and accelerate innovation.
The SCCS–SSAI collaboration provides a strong foundation for advancing trauma care globally, emphasizing equity, contextual adaptability, and patient-centered outcomes. Nordic countries benefit from mature national trauma registries and critical care databases that support benchmarking, policy refinement, and data-driven practice improvement. Saudi Arabia and other Middle East and North Africa (MENA) countries are actively developing similar infrastructures, presenting a strategic opportunity to align registry development with guideline implementation and research priorities.
Establishing national ICU trauma registries with standardized data elements will be pivotal for tracking injury patterns, interventions, outcomes, and guideline adherence in real time. Such platforms—modelled in part on Scandinavian registry systems—can support continuous quality improvement and enable future multinational trauma trials linking MENA and Nordic institutions [55].
Contextualizing recommendations: ADOLOPMENT in MENA and Low- and Middle-Income Countries (LMIC) settings
The guidelines were intentionally designed for adaptability across diverse healthcare environments and were jointly developed by experts from Saudi Arabia and Nordic countries—two regions with distinct infrastructure and care-delivery models. This collaboration enhances external validity and real-world applicability.
In high-resource settings, advanced monitoring tools and comprehensive training facilitate full implementation, including anti-Xa–guided LMWH dosing. Conversely, resource-constrained environments may require simplified protocols, such as prioritizing mechanical prophylaxis when pharmacologic options or monitoring are unavailable. These context-sensitive adaptations support equitable delivery of evidence-based care.
The ADOLOPMENT framework provides a pragmatic pathway to operationalize such adaptations. By enabling health systems to adopt, adapt, or develop de novo recommendations based on local capacity and needs, ADOLOPMENT preserves methodological integrity while promoting feasibility and cultural relevance. This approach empowers national societies, policymakers, and frontline clinicians to align international standards with local realities, fostering sustainable critical care practices.
Addressing implementation barriers in the MENA context
Implementation of clinical practice guidelines across the MENA region is frequently hindered by systemic and environmental barriers, including limited resources, inadequate training and dissemination strategies, and concerns regarding guideline trustworthiness. Regional evidence and Delphi consensus studies further highlight clinician reliance on experiential practice, limited leadership support, and insufficient contextualization as dominant obstacles [56].
Importantly, experience from LMIC trauma registry initiatives indicates that implementation failure most commonly occurs at the level of information management, including data capture, completeness, and governance [57]. Effective mitigation strategies include standardized data-collection tools, early stakeholder engagement, protected data-management roles, and sustainable multi-site funding models linked to quality-improvement deliverables.
Top-ranked facilitators consistently include awareness and education, point-of-care access to guidelines, local customization, and strong organizational endorsement. These findings reinforce the importance of early stakeholder engagement, institutional alignment, and integration of guideline training into broader health-system improvement agendas. Collaborations such as the SCCS–SSAI initiative exemplify how Scandinavian trauma systems can support scalable implementation while promoting contextual validation across diverse care environments.
Conclusions
The guidelines represent a significant advancement in trauma management, providing evidence-based recommendations to address key clinical practice challenges. By emphasizing risk stratification, early intervention, and personalized care, the guidelines aim to optimize patient outcomes and promote standardized practices across diverse healthcare settings. A key strength of the guidelines is their joint development by the SCCS and SSAI, bringing together diverse healthcare perspectives and enhancing their generalizability to various populations. This collaboration ensures that the recommendations are grounded in globally relevant evidence while remaining adaptable to local contexts.
The guidelines highlight the importance of multidisciplinary collaboration and adaptable protocols to address the varying needs of high- and low-resource settings. Implementation strategies that prioritize education, protocol standardization, and teamwork are essential for ensuring equitable and effective adoption.
Future iterations of the guidelines should be guided by robust research, particularly in under-represented regions, to fill knowledge gaps and refine recommendations. Establishing trauma registries and fostering sustained investment in critical care research represent crucial steps toward generating data-driven insights and improving global trauma care.
This call to action encourages the broader adoption of evidence-based practices, expansion of research, and commitment to education to ensure that patients with critical illnesses receive high-quality, patient-centered care that bridges the gap between evidence and practice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rappold JF, Sheppard FR, Carmichael SP, Cuschieri J, Ley E, Rangel E, et al. Venous thromboembolism prophylaxis in the trauma intensive care unit: an American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document. Trauma Surg Acute Care Open. 2021;6(1):e 000643. 10.1136/tsaco-2020-000643.10.1136/tsaco-2020-000643 PMC 790828833718615 · doi ↗ · pubmed ↗
- 2Major Extremity Trauma Research Consortium (METRC); O’Toole RV, Stein DM, O’Hara NN, Frey KP, Taylor TJ et al. Aspirin or low-molecular-weight heparin for thromboprophylaxis after a fracture. N Engl J Med. 2023;388(3):203–13. 10.1056/NEJ Moa 2205973.10.1056/NEJ Moa 220597336652352 · doi ↗ · pubmed ↗
- 3Granholm A, Møller MH, Kaas-Hansen BS, Jensen AK, Munch MW, Kjær MN, et al. INCEPT: the Intensive Care Platform Trial-Design and protocol. Acta Anaesthesiol Scand. 2025;69(4):e 70023. 10.1111/aas.70023.10.1111/aas.70023 PMC 1190738440084471 · doi ↗ · pubmed ↗
- 4La Croix IS, Dzieciatkowska M, Cendali F, Sanders K, Wade CE, Cotton BA, et al. Multiomics reveal plasma constituents associated with thrombosis among trauma patients who do not respond to enoxaparin. Blood Vessels Thrombosis Hemostasis. 2025;2(4):100102. 10.1016/j.bvth.2025.100102.10.1016/j.bvth.2025.100102 PMC 1259491641210697 · doi ↗ · pubmed ↗